I don’t know the answer, rather I am afraid to answer that question.
Read this article , that may help find answer to this forbidden question.

Posted in Uncategorized, tagged ethics in modern medicine on March 27, 2016| Leave a Comment »
I don’t know the answer, rather I am afraid to answer that question.
Read this article , that may help find answer to this forbidden question.
Posted in Uncategorized, tagged 2015 annual report dr s venkatesan on January 1, 2016| 1 Comment »
On this special day , wishing all the readers and followers of this blog an energetic, creative , insightful and of-course a happy new year 2016 !
Just wanted to share the 2015 annual report of this site with the readers.
Posted in Uncategorized on December 20, 2015| Leave a Comment »
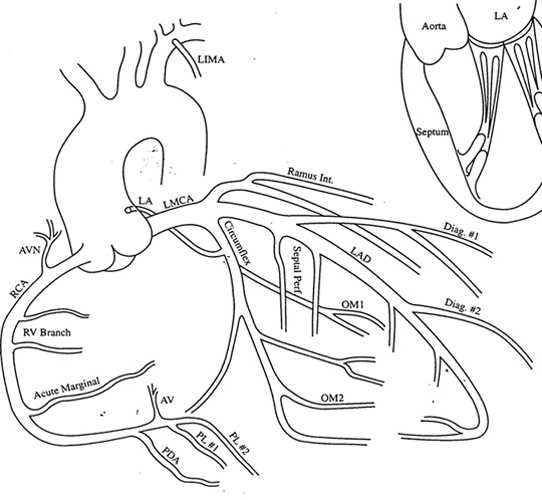
Co-dominant coronary circulation is defined as , when posterior crux of the heart receives twigs from both right and left system making this water shed area with advantage of twin innervation.They essentially supply inferior and posterior aspect of both left and right ventricle including the posterior aspect of interventricular septum.
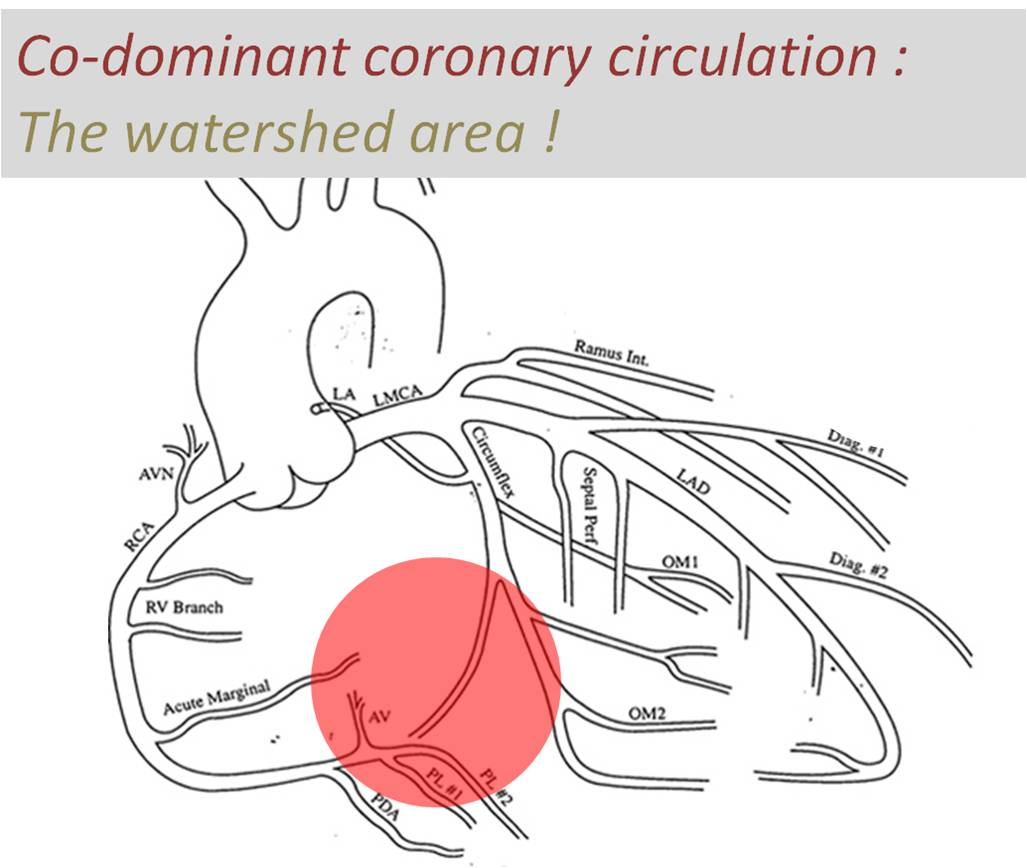
Image courtesy modified from :http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/image4.JPG
Traditionally inferior and basal aspects of heart are perceived (wrong tough !) as less important than anterior surface of heart.Infero posterior MI can be extensive and cause significant LV dysfunction and poor outcome. Longitudinal function (AV grooval velocity) and Mitral valve function is critically dependent on posterior circulation.
Is there an advantage for co-dominant circulation with reference to ischemic mitral regurgitation ?
Obviously ,one would expect there is some advantage in co-dominant circulation when ACS occurs either LCX or RCA.It could theoretically protect against development of MR as posterior papillary muscles could receive supportive twigs from its companion.
However , there is a caveat .The antero-lateral papillary muscle normally has twin blood supply from LAD(Diagonal ) and LCX (OM) . But in co-dominant circulation this pap muscle is at risk of becoming single blood supply as the dominant RCA has a trade off with OM with its large PLV branch. It is likely in co-dominant circulations if LAD is the culprit outcomes are likely to be worse.
Final message
A rare study involving more than 200,000 patients which specifically addressed this issue of dominance and outcome , threw some surprising findings. In concluded PCI outcomes with left or co-dominance has a worse outcome than Right dominant system.
Reference
2.Papillary Muscle Perfusion Pattern A Hypothesis for Ischemic Papillary Muscle DysfunctioPaolo Voci, Federico Bilotta, Quintilio Caretta,Circulation. 1995; 91: 1714-1718
Posted in Uncategorized, tagged fibrinolysis vs priamry pci, indications for coronary angiogram following stemi, priamry pci vs thrombolysis, revascularisation for cad, stemi guidelines, stemi management controversy, timing of coroanry angiogram in stemi, when to do coronary angiogram stemi ? on December 15, 2015| 2 Comments »
Verdict ?
Only complicated or high risk STEMI, would require immediate anatomy based management. Please note, this population at worst is never beyond 20 % of all STEMI. Hence more than majority of patients can be managed effectively without CAG.
My reasoning tells me,though knowing the coronary anatomy appear vital , it is rather the physiological impact of those anatomical lesions that will determine the outcome. So,post STEMI, if at all , we need to investigate, it should be about the adequacy of the over all blood supply to left ventricle.This is done by a pre or post discharge sub maximal stress /nuclear test .If it’s negative with a good exercise tolerance CAG will never be required as any critical flow limiting lesion ( that would require intervention )is excluded with near 100% surety.
Postamble :Try asking any neurologist , how often they demand to know cerebral arterial anatomy for managing stroke ? You will get a real surprise answer !
Posted in Uncategorized on December 11, 2015| Leave a Comment »
Holter monitoring is the Initial test for all those with documented syncope (or Pre syncope ) with suspected cardiac arrhythmia .It is a 24 hour ambulatory ECG monitoring , expected to pick up any electrical abnormality and its correlation with the resultant symptom if any. Though the test looks attractive , the diagnostic yield is far less. (About 10%) .The reason being the episodes can be rare to be missed by 24hr sample time. We have extended Holter (48hr) , Event monitors , Loop recorders and implantable devices that can record ECG for extended periods.(18 Months ,Reveal Plus Medtronic) that improve the yield up to 45%.
One common issue that often confuse us while reporting Holter is, the pauses that occur during day / night .
What is the significance of these pauses * ? Nocturnal vs Daytime
Pauses are obviously significant when the patient is awake . It is generally accepted pauses more than 3 seconds during day time (ie Heart rate of < 20/mt ) is significant . This is logical , as pauses more than that, is expected to cause syncope ( or atleast pre-syncope ).The problem comes when you document pauses more than 3 seconds without any symptoms . Then this difficult question comes up ,At what degree of pause syncope occurs ? How is that some persons mange even prolonged pauses with just giddiness.(Good overall vascular integrity and tone ! )
We know such pauses are especially common during sleep. How does the brain react when pauses occur during sleep ? as there is no question of fall as such and loss of muscle tone is non existing.
*Please note ,when we say pause we mean only Sinus pause , Pauses due to AV blocks are very significant
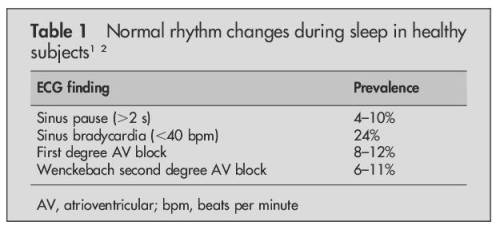
Source : Brodsky M, Wu D, Denes P,et al.Am J Cardiol 1977; .
Dramatic pauses during sleep do occur
There has been prolonged pauses reported during sleep without fatality . A 35 second nocturnal pause resulting in seizures has been documented by implantable recorders.(Mairesse 2003)
Causes for prolonged pauses
Final message
Most bradycardic episodes during sleep are benign.This is due to depressed autonomic control during sleep. Holter interpretation is primarily done with awake rhythm data in most individuals .So, empirically shall we fix a 5 second pause as significant during sleep ? We don’t know.While this may seem applicable even with structural heart disease , one may be vigilant while interpreting the nocturnal pauses in this population .
Caution
** Please note, all these rhythm monitoring extravaganza is meant for people with equivocal symptoms .Patients with well documented syncope with ECG features suggestive of cardiac rhythm disorders would never require these tests and go for pacemaker straightaway.
Reference

Posted in Uncategorized on November 12, 2015| Leave a Comment »
Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart Disease are just out in NEJM.
The results are as expected !
“Let us get more Courage , to say no when we want to say no !”
Reference
http://www.nejm.org/doi/full/10.1056/NEJMoa1505532?query=TOC
Posted in Uncategorized, tagged classification of pvt polymorphic vt, polymorphic vt on October 16, 2015| Leave a Comment »
A classification of Polymorphic VT .
It can be classified according the etiology, morphology or hemodynamic stability . However , for some reason classifying PVT with reference to the preceding QT interval and the manner in which tachycardia twists its axis along the qrs axis has been the most popular theme . ( Obviously ,the classification process should evolve further , and management strategies should be linked with it )

Read a related article :Different Avatars of polymorphic VT
Posted in Aortic regurgitation, Hemodynamics, Infrequently asked questions in cardiology (iFAQs), Uncategorized, tagged austin flint and diastolic mitral regurgitation, diastolic mitral regurgitation, diastolic murmur in complete heart block, reverse diastolic av gradient on October 11, 2015| Leave a Comment »
Mitral regurgitation is expected to occur only in systole during left ventricular contraction. In rare pathological states , if LV pressure exceeds the mean LA pressure at any point in diastole , small puffs of regurgitation into LA can occur.The genesis of this MR and its hemodynamic significance has generated much interest .
Causes
Mechanism
No single mechanism is responsible.
 Timing of diastolic MR
Timing of diastolic MR
It occurs in later part of diastole as it takes a time lapse for raising LV diastolic pressure to cross the LAP and generate a reversed ventricular gradient.
Will there be a clinical evidence for this MR ?
Its silent in most cases .Some patients with complete heart block may generate mid diastolic murmur . (Rytand AHJ 1946) .Retrospectively this could be due to diastolic MR
Is there a link between Austin flint murmur and diastolic MR ?
Many researchers believe the generation of diastolic murmur in severe AR is attributable to premature closure of mitral valve and the poorly compliant LV is not able to accommodate the leaking blood and it tends to regurgitate into LA through partially closed mitral valve in diastole (Ochaya S, Am Heart J. 74 1967:161-169)
Echo features
Cath correlation
Wong has demonstrated this phenomenon by direct hemodynamic recording in 4 patients
Further research
While the field of diastology is growing , still we are not clear how significant this MR in clinical diastolic dysfunction and acute LV failure that results in flash edema.
Reference
Posted in Uncategorized on October 2, 2015| 1 Comment »
“Oh , it’s a well recannalised IRA and its flowing TIMI 3 as well. Now, what shall we do sir” ?, An apparently worried senior resident queried after a second look at the images from a 8 hour old STMEI .Why you sound unhappy man ? As if recanalisation is an untoward event” ! I teased my resident !
and went on to ask . . .
What we mean by recannalised IRA ? (Recan-IRA)
The term recanlised IRA generally convey a hemodynamic meaning for a successful early (natural plus or minus pharmacological ) reperfusion .If every parameter is fine , and the lesion is not significantly obstructing better to pause any further procedure , as consequences of deploying stent in a well recannalised segment is not yet clear with a stro ng trend towards harm .The decision is to be taken on individual basis with reference to symptoms, stability , residual ischemia and quantum of incomplete salvage and lesion morphology .
If you believe ,a spontaneously recannalised IRA has provided a TIMI 3 flow , it is equivalent to well done job of natural thrombus aspiration by a hidden hand and catheter . Consciously respect that .Most cardiologists would have realised atleaset once , that any aggression on a God handled IRA can be counterproductive !
Is there a non academic angle to this issue ?
Undoubtedly yes , strangely inspite of a positive phenomenon for the patient , recannalised IRA leads to a difficult debate in cath lab .Suddenly , the entire collective scientific wisdom of the cardiologist is put into a stress test. There is direct fight between reality , expectations .True patient benefits , obligations to hospitals , the parasitic relations with device industry , do have a big say !
Final message
Practicing cardiology is simple , but when scientific and non scientific realities of life are in direct confrontation with patient welfare it becomes a huge struggle and only a determined few can win over this infinite fight against conscience !




{kind=link}