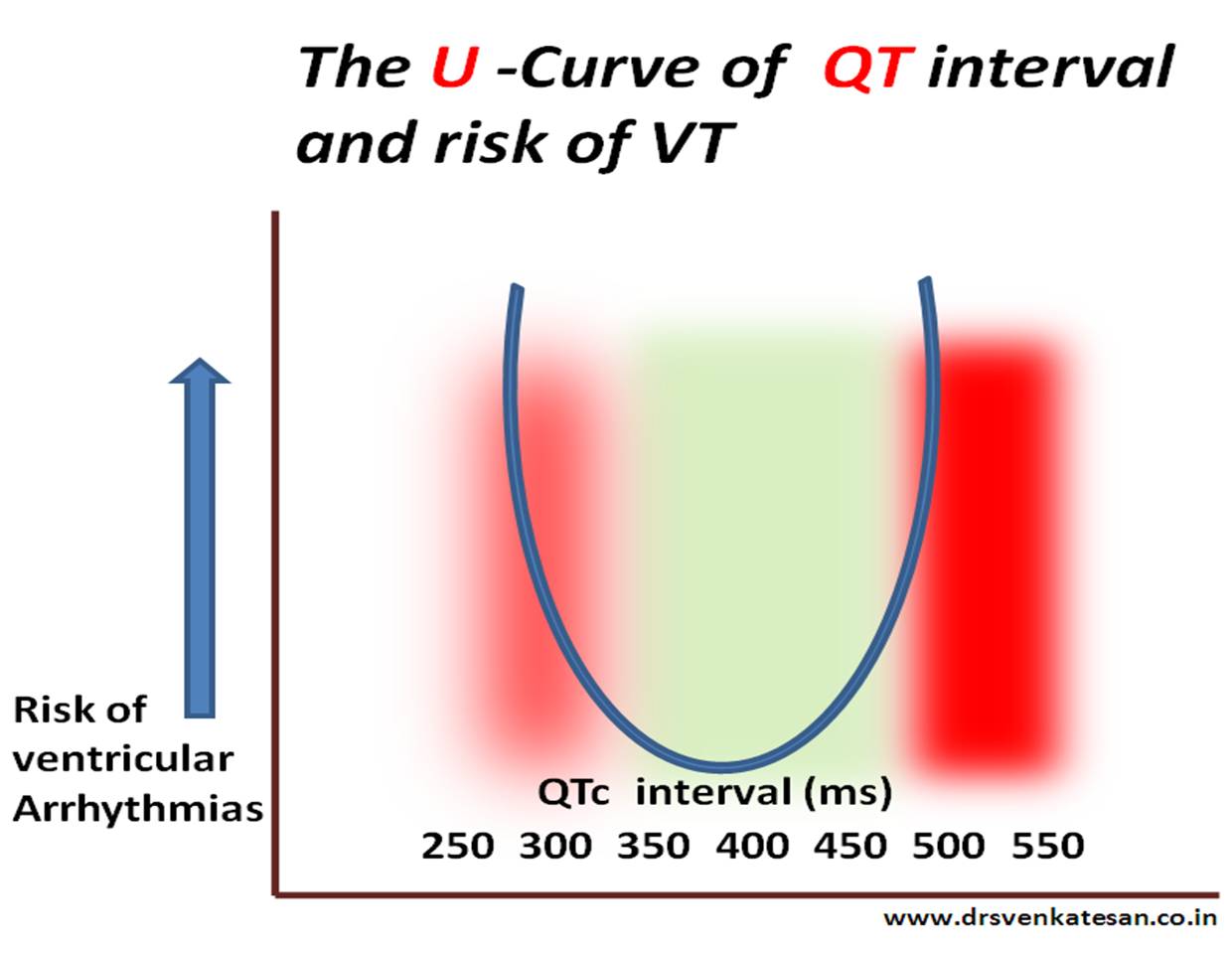
The stretch and strain experienced by the action potential’s left shoulder region is almost similar* in both long and short QT syndromes that trigger a VT.(* Hope this explanation makes some electrical sense !)
*Click over the image for high resolution
What is short QT interval ?
It is a range . Any thing less than 380 ms can be considered short.Generally It becomes important only at < 320ms.
In this mean world ,most truths exist without evidence . . . and often falsehoods masquerade as truths with overwhelming evidence !
Human biology has always been a mystery and can express in dramatic ways . While , many disorders combine to play havoc on the body , few tend to protect each other. HT and DM can join a deadly coalition to attack the heart .Smoking causes extensive peripheral vascular disease , still thrombo angitis of coronary arteries ( due to smoking ) is virtually unknown. Tuberculosis does not have the courage to attack the heart valves , while it can inflict serious injuries all over the body . Similarly , systemic hypertension and Rheumatic heart disease does not combine well . So , it can be assumed some unique and hidden protective factors are at play among different pathological entities and their target organs.
A brief account of how COPD could be related to CAD ! (* Mostly Imaginary !)
We know , COPD , stresses the right ventricle by pressure overload and in extreme situation affects the LV function because of hypoxia. It rarely impacts the coronary artery disease . This has been our consistent observation. While COPD patients often land up with LV dysfunction , investigations reveal they are more of a dilated cardiomyopathy and their coronary arteries are entirely normal. Diffuse atherosclerotic CAD is a rarity in patients with history of bronchial asthma. Coronary micro circulation is also observed to be largely intact in most people with COPD .
We haven’t got a call from our pulmonology wards in many decades , for a true emergency coronary consult . Mind you ours is a 200 year old Institution , with 3000 beds , largest east of Suez canal !
It’ s very rare for bronchial asthma patients to die of a cardiac event. Thousands of elderly patients throng our ER with acute severe asthma every winter , still extremely rare to precipitate an acute coronary event !
We are yet to see critical triple vessel disease in a patients with documented bronchial asthma and COPD . Even non-critical CAD is far less frequent in COPD vis a vis general population . It is indeed a strange observation , considering both entities are rampant in the community .
What could be mechanism for the perceived disconnect between COPD and CAD ?
Is it a myth ? Does it happen in all geographical zones ? If hypoxia is the sine qua non of COPD , one would rather expect a close association with CAD , isn’t ?
One suggestion that keeps erupting from my cortex . It is the wide swinging intra thoracic pressures in COPD or asthmatic individuals . . . somehow responsible . These wide swings of pressure are transmitted to aortic root . They transform into good coronary perfusion pressure , keep the vessels clean by pressure vacuuming effect .
We have asked our epidemiological unit to analyse the 25 year data from our coronary care unit to decode the mystery .
Counterpoint
Meanwhile, a diagonally opposite question was asked in UK and found a partial proof as well . Our experience do not agree with this study conclusions .
How can a opinion (rather an Imaginary essay !) based on personal observation projected as a scientific fact ? We need to observe , analyse and publish the data . This is what the scientific world expects us to do . Unfortunately , the journey form observation into publication has been kept purposefully difficult . In my opinion bulk of the international peer reviewed medical journals with high impact factor can convert any junk data into a scientifically palatable recipe !
The doctrine of modern medicine goes something like this . . .
For most medical problems , there would be a solution. Keep trying . . . till you get it !
*But , just make sure that problem on hand deserves a solution in the first place !
Modern medicine continues to remind us every day , the much hyped solutions often end up in new problems and many times worse than the original problem !
Oh ! what a great a quote ! When I was boasting myself . . . My wife reminded me , this is just plagiarized version of a 2000 year old Hippocratic thought !
Scientific studies can be fun .In our spare time we often Indulge in rapid fire sessions. We tested 30 wide qrs ECGs from our archives (All proven VTs) and asked our cardiology fellows to apply Brugada criteria . They could correctly diagnose VT in 18* patients.The same ECGs were shown to the staff nurses of coronary care unit . 24 VTs were correctly identified it.They did it by their clinical sense and Instinct. (*12 vs 6 VTs missed)
And now , four clinical data was provided. (Age , sex , Blood pressure , and past H/o MI were given ) The Nurses were able to predict it 28/30 VTs correctly.(97 % accuracy ) and the cardiologists were able to equal the score now. So obviously clinical sense was far superior .
Cardiology fellows were more likely to mistake VT as SVT. This is far more common than SVT mistaken as VT. It is a strange academic irony ,even the junior most nurses never missed a VT !
Summary
Simple sequence of history and clinical presentation is still far more powerful than ECG data in predicting wide qrs arrhythmias . Nurses guess work is far superior than cardiologists in predicting a wide QRS tachycardia as VT.
In fact , the cardiology fellows are preconditioned to get confused whenever they get a wide qrs tachycardia . Why not aberrancy ? In my experience I have seen this question keeps erupting inappropriately .Even shrewd fellows suffer from an oscillatory mind between VT and SVT .This is primarily because , every wide qrs ECG is likely to have at least two criteria that fulfill both VT and SVT.
The implications are genuine and far reaching . While nurses show a patient centric thinking cardiology fellows thought process revolves around ECG . Many modern-day cardiac physicians are disconnected from clinical reality and are obsessed with complex EP concepts and end up with a miserable face in the bed side !
This is not a new revelation in 2013 . Masood Akthar told this three decades ago.
Caution
Never try to glorify guess-work . EP is a great science .The pioneering concepts have made us understand how a VT emanates, travels , and exit from myocardium . We are able to localise it and ablate it .All credit goes to science . But , when it comes to bedside recognition of VT , clinical sense is a clear winner .With a consistently > 90 % predictive value it can no longer be called as a guesswork and becomes a hard scientific fact. Especially so , when the intellectual analysis of surface ECG could predict it with paltry 70 % accuracy (Read Reference 1)
This analysis startlingly reveal a fact .The over all accuracy rate of predicting the wide qrs criteria by popular algorithms is between 66-77% , just 16 numerals more than gross guess work of 50 : 50 ( This . . . or . . . that )
“Feb 20, 2013 – … in the New England Journal of Medicine Show Dabigatran Etexilate ... daily was non-inferior to warfarin (p=0.01) in preventing recurrent VTE, …”
What is the logic behind these Non inferiority trials ?
Why it came into vogue ?
Do you agree with the concept of NIT ?
I have taken the privilege of putting my answer in the title. Believers of NIT please excuse me.
Cannon waves occur when Atria contracts against a closing tricuspid valve of right ventricle .( There would be a equivalent left atrial cannon which goes into pulmonary vein as well , it is discussed elsewhere !)
Cannon waves happen only when P waves fall within QT interval in ECG as QT represents the electro-mechanical systole of ventricles. (Since P wave represents atrial systole , it is simple to understand when it falls within QT both atria and ventricular contractions collide to produce a cannon wave into the neck or pulmonary veins.)
The following two images of cannon waves taken from the legend Dr Paul woods own tracing .
Regular cannon waves
Occur during SVT with 1:1 VA conduction.*
1 : 1 VA conduction can be considered as absence of AV dissociation (Rather disciplined VA association with every beat ) This is essential to create a hemodynamic milieu for regular cannon waves.
* In AVNRT , VA conduction in strict sense is a misnomer .It is simply a retrograde conduction thorough the AV node .
Irregular cannon waves
Complete heart block .
Multiple random VPDs
Some patients with VT.*(Who are those patients ? Those with AV dissociation when retrograde “P” wave falls within QT interval cannon occurs. As expected this occurs in random fashion which makes the cannon fire irregular.
Can we get regular cannon in VT ?
Yes , but rare . As explained earlier this can happen only if AV association occur on a retrograde fashion.
Rheumatic fever and RHD is still a major cause for cardio vascular morbidity and mortality in India .It seems , improving quality of life has little impact on the incidence .(We could realise this as we sit in the cardiology OPD of a 200 year old hospital !) There is no country wide data on the true prevalence . Our understanding of rheumatic heart disease is based on isolated studies on localized populations .
Of late , cardiology resources in our country is diverted towards much glamorous CAD the poor continue to suffer with RHD.
Just Imagine many hospitals indulge in 1000s of PTCA every year but hardly do a hand full of PTMCs.
How our cath lab resources are used across the breadth and length of country needs some introspection (Currently , I believe we have about 750 labs ) .I think there should be a binding legislation in every cath lab .For every 10 PTCAs done at least one PTMC must be done to heal the poor .( Like the Air-craft license .You can’t fly only the lucrative metro sector is given only if IT services less developed areas )
In this scenario , it is a pleasant surprise to find a wonderful review article on RHD from the two pioneers , in lesser known medical journal IJMR .
Especially heartening is the fact , it is a collective effort from two distant regions of India ( Kochi from down south and New Delhi In the north) . While politicians keep the divide , it is a great work of the authors , which would help youngsters who would like to go on a national mission on eradication of RHD. .
Hypertension is probably the most important clinical entity for physicians
for decades .With the advent of modern interventional cardiology management of HT with drugs have become a less glamarous job for us. Still , the quantum of the problem and it’s impact on the risk of CAD and progression remain a major issue.
There many different bodies periodically coughing up guidelines to manage HT.
JNC from USA
British Hypertension society from UK
European society of cardiology
World hypertension league
Finally WHO guidelines* ( It is not a regular exercise ,WHO releases it as and when it feels like !)
The stakes are high for the drug industry .Anti hypertensive drugs are the major source of revenue to them . Any dip in per capita consumption will have direct impact on their health ! ( WHO bothers about public health ? )
The so called scientific guidelines, are generally made balancing patients health vis a vis drug companies health .I have found more often than not it was tilted towards the industry .
The fact that there are multiple guideline with varying impact factors makes sure the confusion among the global physician intact . This is one of the aims of the pharma companies as they influence heavily when to initiate the treatment , and what we are supposed to prescribe.
Some of the guideline are notorious for insinuations . One example was about the definition of pre hypertension few years ago .It has since been removed from the literature after a critical debate .
* One may wonder why I’m focusing always on non scientific issues more than academics .(I some how feel non scientific factors are going to impact our health more than any other factor in the coming generations )
Now is the beginning of a balance .
Among these guidelines I would think ESC is close to reality and fairness.
Even it was carrying dubious advices till recently .Now they have come out with new one in 2013.Most changes are welcome.
It is essentially about cleansing the contaminated guidelines
Removing unnecessary medications
Unified definition.
More efforts to identify true secondary HT
The salient points
There are 18 point update in the ESC 2013 . All of them are great . Essentially they are about the basics we have been taught as we learnt in our final year MBBS. (The rest of our life we have to unlearn the junk we have accrued over the years from various CMEs )
I can modify it and short list
Do not start too early .Have universal definition (Now 140mmhg)
Respect non drug treatment ,( However attractive the gold tipped pen the representative leaves in your consulting suit !)
Avoid using multiple drugs
Never miss a secondary HT .( If diastolic BP> 110mmh almost always a renal component would be there .Remember Conn syndrome (Primary aldosteronism ) is 10 times more common than much hyped pheochromocytoma ! Just do K+ levels to detect this )
In CAD patients never treat HT in isolation .( Measure blood pressure with sugar and lipid 120 /70 mg of LDL )
ESC 2013 is a commendable Initiative . It has tried to remove most errors of the past .obviously the pharma industry will be unhappy as it will definitely bring down total drug consumption the population.
Final message
HT is an important target for prevention and management of CAD
Thanks to the much maligned pharma industry .
We have good drugs.Use it judiciously . Try to reduce the number of drugs .
If possible make them drug free.
If a patients taking beta blocker for associated cardiac condition do not add another anti HT drug . (Recall from your distant memory , beta blocker is a anti HT drug too !)
Simply follow common sense . (* If you think you lack it , get it from your learnt patients .Many of them have in plenty . I often do that . One question they keep asking “Should I take this drug life long doctor ?” is a definite common sense booster! )
A Cardiologist will never accept the diagnosis , if a technician reports a ECG as normal in a patient with chest pain . . .
While , the same cardiologist gleefully accepts an echocardiogram done by a technician and treats the patient without verifying the veracity of the finding !
Why ?
Some where along the cardiology training , we have been made to believe Interpreting Echo Images does not require serious medical knowledge . . . but we strongly believe ECG cannot be read by technicians however well they are trained .(In-spite of the fact , Echo images are highly dependent on the person who does it , while ECG wave forms are totally independent of the person who record it ! )
ECG, still has a prestigious place in cardiologist’s mind , while Echo is often considered an inferior Investigation. Many of us consider ECG interpretation as a brainy work while Echo image acquisition and interpretation is perceived a dumb job* !
Lastly , probably most importantly , performing Echo is a time intensive process for the present day cardiologist who’s hands are tied with catheters and guide-wires .He has little time for the meanly echo . . . hence ready to compromise on the quality .
* With due respects to all non invasive cardiologists (That includes the author !)
Final message
I would think it is fundamentally inappropriate for technician to report Echocardiogram (Of-course they may record it ) . Unfortunately , for some reason this practice is continued in many parts of world .
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.