*The post is not meant for those who understood GLS (Global longitudinal strain) in a proper perspective. I am writing this, after a surprising answer from many students of Echocardiography, when I asked them what is GLS? Most answered, GLS currently is the best global LV functional index available. What a misunderstanding? The fact is, EF % will always be the best global parameter*, while GLS remains a regional function index.(*The limitation of EF% is in the methods of measuring it and not in EF itself.)
We are trying hard to ditch LV EF% by Teichholz’s / even 2D Simpson method, as they are considered a crude way to measure global LV function. Unfortunately, we are doing this without a credible alternative. GLS is being promoted as the next best. The normal GLS is around(-20 ± 2) . Nothing is perfect. Best global LV function probably can be achieved by 3D Voxel Echo/MRI)
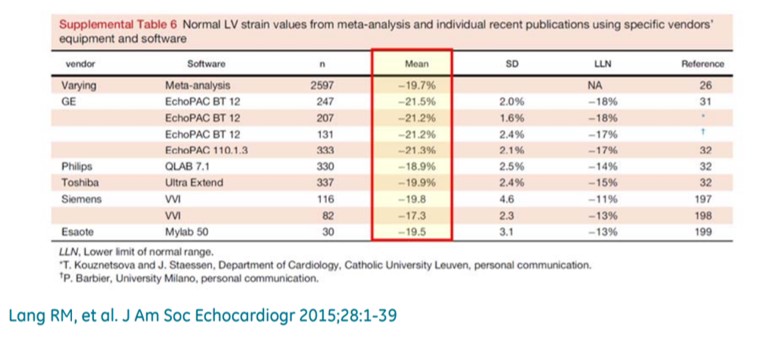
Normal GLS with various machines
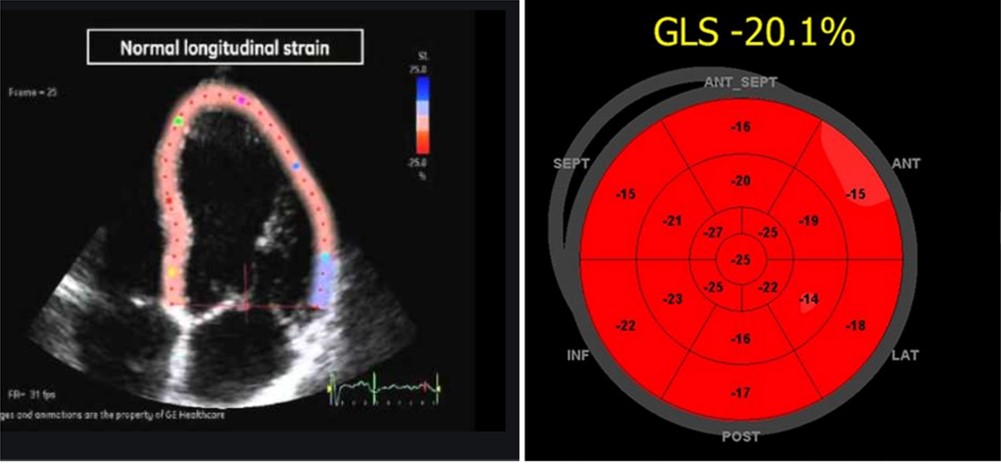
Please note, the bullseye 17 segment model though brings an illusion of a radial perspective of cardiac contraction, its purely longitudinal stain represented in short axis format.
The much popular GLS (Global longitudinal stain ) is a poor surrogate for global function. The word global is apparently misguiding and conveys a false message. When we refer to GLS, it is an adjective for longitudinal function and nothing to do with overall global LV function. (Though we have many studies to show it has good correlation with global LV function).
The longitudinal function is presumed to contribute 60 % of LV function. This means GLS is at best 60 % accurate in determining global LV function. Mind you, the heart doesn’t work in a longitudinal plane alone. The muscle fibers of heart are arranged in three distinct fashion (LOC) subendocardial- longitudinal, Mid-oblique, & Sub epicardial -concentric (Remember LOC ) Each fiber either lengthens or shortens.
The left ventricle not only shortens longitudinally, It also contracts radially, shrinks circumferentially, rotates clockwise at the base (5-10º) , counter rotates at apex (Up to 60º) twist, & un-twists. It’s worth reminding ourselves, we are ignoring all these components and happy to fall for GLS.
What can be done to improve the accuracy of true global strain?
The simplest way is, to look LV in short-axis by 2D and confirm everything is okay with radial contractile forces and deformation. Mind you, the most accurate tool to measure stain is the good old M mode with undisputed temporal (time) resolution ad frame rate the M mode thickening best deformation parameter to measure radial stain ( at a particular plane though).
Is the measurement of true global strain possible? (GLS+ GRS)
Probably yes. What about GLS plus GRS (Global radial strain) GLS measured by speckle + RS (Radial thickening by 2D/aided by M Mode) We are working on a project where the radial strain component is added to GLS. Roughly, it should pull the negative GLS beyond + 20 (If we assume GRS is + 30 to 60 ) This should be correlated with 3D voxel Echo /MRI .
Final message
Beware,The “G in GLS” is a perfect miscommunicator. * GLS can never reflect global LV function. If EF% by M-mode was criticized, for measuring only one aspect of cardiac function ie radial, the same would apply for GLS, in that it measures only longitudinal function. Never discard M mode/2D. It still, pours unadulterated ultrasonic data from myocardial contractile units in the highest resolution. We should continue to use it. In the name of modernity, we make it look outdated.
Reference
M S Amzulescu, M De Craene, H Langet, A Pasquet, D Vancraeynest, A C Pouleur, J L Vanoverschelde, B L Gerber, Myocardial strain imaging: review of general principles, validation, and sources of discrepancies, European Heart Journal – Cardiovascular Imaging, Volume 20, Issue 6, June 2019, Pages 605–619, https://doi.org/10.1093/ehjci/jez041
*