It appears,antiplatelet agents are waging a turf war on the CAD battlefield. It is no secret either, the fight often goes beyond academic reasons. Though NSTEMI connotes a true cardiac emergency, it consists of a highly heterogeneous population. A patient with UA can be treated even at home (Low-grade angina with little ECG changes, when it’s due to Increase demand situation). While, in the other extreme of NSTEMI, a patient with a GRACE score >200, in Ischemic LVF, might need an emergency multivessel angioplasty along with Mitra clip ± ECMO support.
Antiplatelet agents along with heparin will remain the cornerstone
* in the management of NSTEMI/NSTEACS, irrespective of our fine catheter skills within index lesion. They are administered right from the pre-hospital phase/ In ER, CCU/ or on way to the cath lab(upstream)/or within the cath lab/or after CAG /PCI. It is the right balance between the prevention of stent-related coronary thrombus vs systemic bleed we are worried about. Definitely, DAPT is warranted. (See the chart below) Prasugrel has been reinvented as the most powerful P2/Y12 blocking antiplatelet agent. It squarely beats its other colleague drugs like Aspirin, Clopidogrel, and Ticagrelor in terms of potency as well as its risk of a bleed.
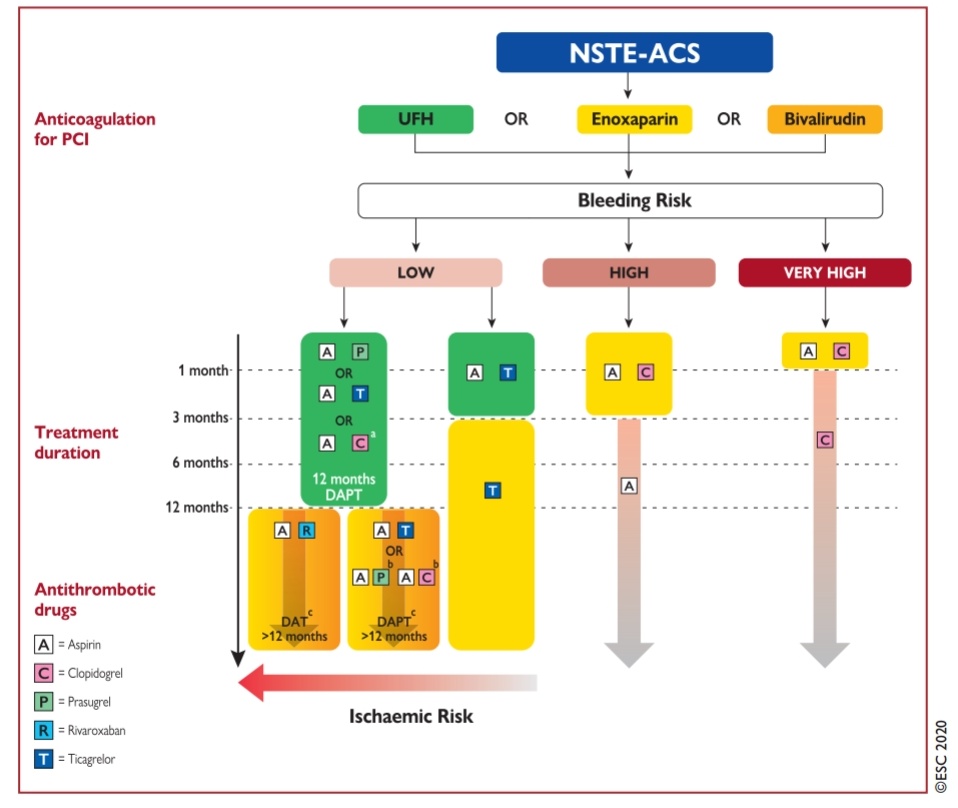
This is the current antiplatelet protocol in NSTEMI in a patient planned for PCI after visualizing the coronary anatomy. Note, Aspirin plus Prasugrel combination occupies the top slot among various options. The principle of DAPT strategy is all about Initial escalation to match the heightened risk of thrombosis/ cardiac events and later de-escalate once the risk period is over (Which can vary between 1 month to 12 months or even 2 years)
* The popular concept of attributing NSTEMI to platelet clot and STEMI to fibrin clot is no longer valid. The contribution of the individual component(white vs red) in a given load of coronary thrombus was never quantified accurately. That’s why antiplatelet agents alone are grossly inadequate in NSTEMI. This will be vouched by this NSTEMI algorithm, which begins with red clot busters heparin. So, how to handle sharp-edged drug-like Prasugrel?A powerful drug-like Prasugrel is at high risk of being misused. It has taught us some harsh lessons in stroke. So, we have to be wiser to extract the maximum out of this drug in the presence of a high thrombotic milieu (or at risk of developing it after a PCI.)
Since ECG and clinical features are not sufficient to predict the coronary thrombus. It is suggested to have a look at coronary anatomy and decide only if a PCI is contemplated.Some of the situations where Prasugrel is likely to be Indicated
- Any PCI with a stent in the culprit artery.
- High thrombus load
Prolonged procedure time
When to Avoid Prasugrel?
Just looking at coronary anatomy is not sufficient. Estimating the risk of bleeding is required. Attempting to use various scoring systems during a cardiac emergency is a self-inflicted mathematical burden. In my opinion, none of these scoring systems(CRUSADE , ACUITY, ARC-HBR) truly discriminate patients in a useful way. Mindfulness with an eye on co-morbid conditions is required.This has to be matched with coronary lesion /PCI complexity. Realistically, the confidence in our technical adequacy of stent deployment shall decide the need for aggressive post PCI DAPT or anticoagulation
Final messageJust because we know the coronary anatomy,
don’t expect prasugrel to be kind enough to lower the risk of stroke. The risk is the same whether we know anatomy or not. It is the funny evidence base we have created that makes us believe it so. Routine DAPT for all patients with ACS is not warranted without assessing the bleeding risk. Meanwhile, there can be an important subset of patients who can really benefit from prasugrel even within coronary care units who are unplanned for PCI. (Which the current guidelines seem to forbid without any valid reason)
PostambleWe know, stents love to befriend thrombus instantly, that demands aggressive antiplatelet/anticoagulants) which beget bleeding. So,
should we stent all lesions in a given patient with NSTEMI ? is a very valid question (rarely asked though) needs to be answered by the custodians of patients’ heart. When dealing with a complex PCI case scenario, simple mindfulness with an eye on comorbid conditions and downgrading ourselves to a good general physician mindset is welcome.
Reference1.The DUBIUS trial downstream vs upstream use of antiplatelet agents in NSTEACS- No difference
https://www.acc.org/latest-in-cardiology/clinical-trials/2020/08/31/21/44/dubius
2.