Pulse deficit is a clinical sign wherein , one is able to find a difference in count between heart beat (Apical beat or Heart sounds ) and peripheral pulse .This occurs even as the heart is contracting , the pulse is not reaching the periphery.This can occur in few clinical situations .
1 . Atrial fibrillation.
2. Very early diastolic ventricular ectopic beats
3. Some patients with Pacemaker.
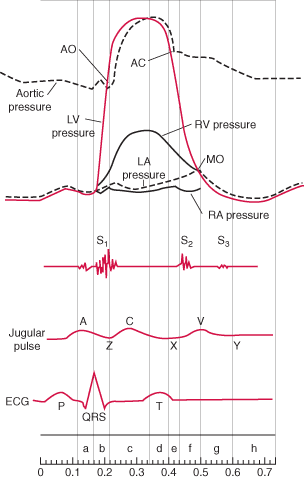
The mechanism is , the ventricular contractions are too weak and unable to open the aortic valve (Or opens feebly*) , but at the same time they are good enough to close the mitral valve. To open the aortic valve it has to generate atleast 60-80 mmhg pressure , while mitral valve closes even as LV generates 8-14mmhg .(LV/LA pressure cross over). So intermitently the second heart sound is missed while S1 is retained, producing more heart sounds and less pulse count in the periphery. The S1 is either felt or heard at the apex but the corresponding pulse is missing . Further , this intermittent absence of S2 results in totally irregular S1 /S 2 relation.
Why some of the contractions of LV is too weak to open the aortic valve ?
Because the RR interval varies , the ventricular filling also varies , diastole duration is constantly changing some of the diastole are too short and LV hardly gets filled , as the LV force of contraction is directly decided by the LVEDV and LV fibre length these contractions are too weak.
Other published studies
There has been some doppler observations ,where there is a midventricular LV blood flow reversal in atrial fibrillation that could explain the pulse deficit . Mechanism of production of pulse deficit in atrial fibrillation: assessment by blood flow dynamics
Second Department of Internal Medicine, Kagoshima University School of Medicine.
http://www.ncbi.nlm.nih.gov/pubmed/3221309
What is the clinical significance of pulse deficit ?
Currently there is no great clinical significance of this phenomenon. But an astute clinician will pick up this sign and it may indicate underlying LV dysfunction. In patients with PPM, pulse deficit suggests pacemaker malfunction .Some patients with cardiac tamponade & pulsus paradoxus systolic blood pressure falls too low to make the pulse feeble or not palpable in the periphery .This situation may mimic a pulse deficit if not recognised.
Dr.S.Venkatesan ,Madras Medical College , Chennai, India
* What is the evidence for intermittent absence or feeble Aortic valve opening in Atrial fibrillation ? I could find this from the book written by Harvey Feigenbaum. whom we consider Father of Echocardiography





How do you assses rate control in atrial fibrillation following digoxin or beta blockers?
one should ideally rely on heart rate or the ECG rather than the pulse rate.
what is the significance of palpable heart sounds in an atrial fibrillation patient ?
Palpable heart sounds in Atrial fibrillation is usually due to the first heart sound with varying intensity,
the loudest component is palpable. This indicate often an underlying diagnosis of mitral stenosis.
however , any long – short cycle sequence can result in a palpable first heart sound.
I am interested in reading reports of this nature such as you have produced.How do I get them. I have the said problem. Thanks for prompt acknowledgement.