Modern human life is driven by technology . We are gradually taken over by gadgets .Heart is not an exception . Implantable cardiovertor defibrillator (ICD ) is major innovation where in , an electrically wayward heart is brought under control by series of automatic shocks . One of my patients with old MI and significant LV dysfunction for whom ICD was an option taught me a lesson in physics . During counseling , he was asking me about the quality of life issues etc .

First, he wanted to know how stressful the sexual acts are ? . . .Then he surprised me with this question . He wanted to know , the risk of developing a VT/VF during the act and will the ICD shock his spouse as well ? That was a real cracker of a question I thought . I had to do a mini research and found that these are low energy shocks (30 Joules) and transmitted electrical injury is a non issue .
I realised then . . . we live in a era where physicians often get educated from their patients !
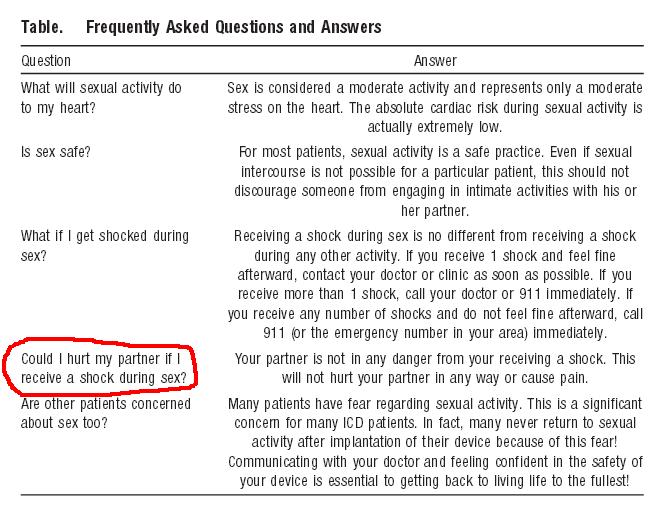
Here is the FAQs on ICD from the patient pages of circulation . With due courtesy I reproduce it here.
Final message
ICD shocks are low energy shocks delivered Intra cardiac , and rarely reach the surface , hence has little risk for electrical injury for those in contact.
References
1. Vazquez LD, Sears SF, Shea JB, Vazquez PM. Sexual health for patients with an implantable cardioverter defibrillator.

2.Steinke EE. Sexual concerns of patients and partners after an implantable cardioverter defibrillator.
Dimens Crit Care Nurs. 2003;22:89–96
3. A review article on the broad issue.