Why didn’t you do it … for this patient?
“I thought, he was not the right patient for the procedure. I believe, what I did was the correct decision. Why all this fuzz? after all, the patient is doing so well without that procedure,.. are you worried about that?
“No, I need an explanation, we have a fully functional cath lab in our center. The patient came in the right window period. Still, you haven’t offered the best mode of treatment”.
“I can reiterate it again sir. Just because a lab is available 24/7, it doesn’t make all patients eligible for a PCI. I think I didn’t commit a professional misdemeanor when I decided in favor of fibrinolysis. In fact, I would be guilty had I rushed him to the cath lab, just to satisfy the misplaced scientific position we have decided to adopt. If you think, I am culpable for successfully treating a patient without taking the patient to the cath lab, you may proceed with the penal action.
Before that, I would request you to please read the current edition of this book we all revere. (Which continues to mentor physicians all over the globe for the past 50 years)

The current edition of Harrison 2022 is just out. I thought, there is something great learning point in Cardiology chapter, specifically about the reperfusion strategies in STEMI
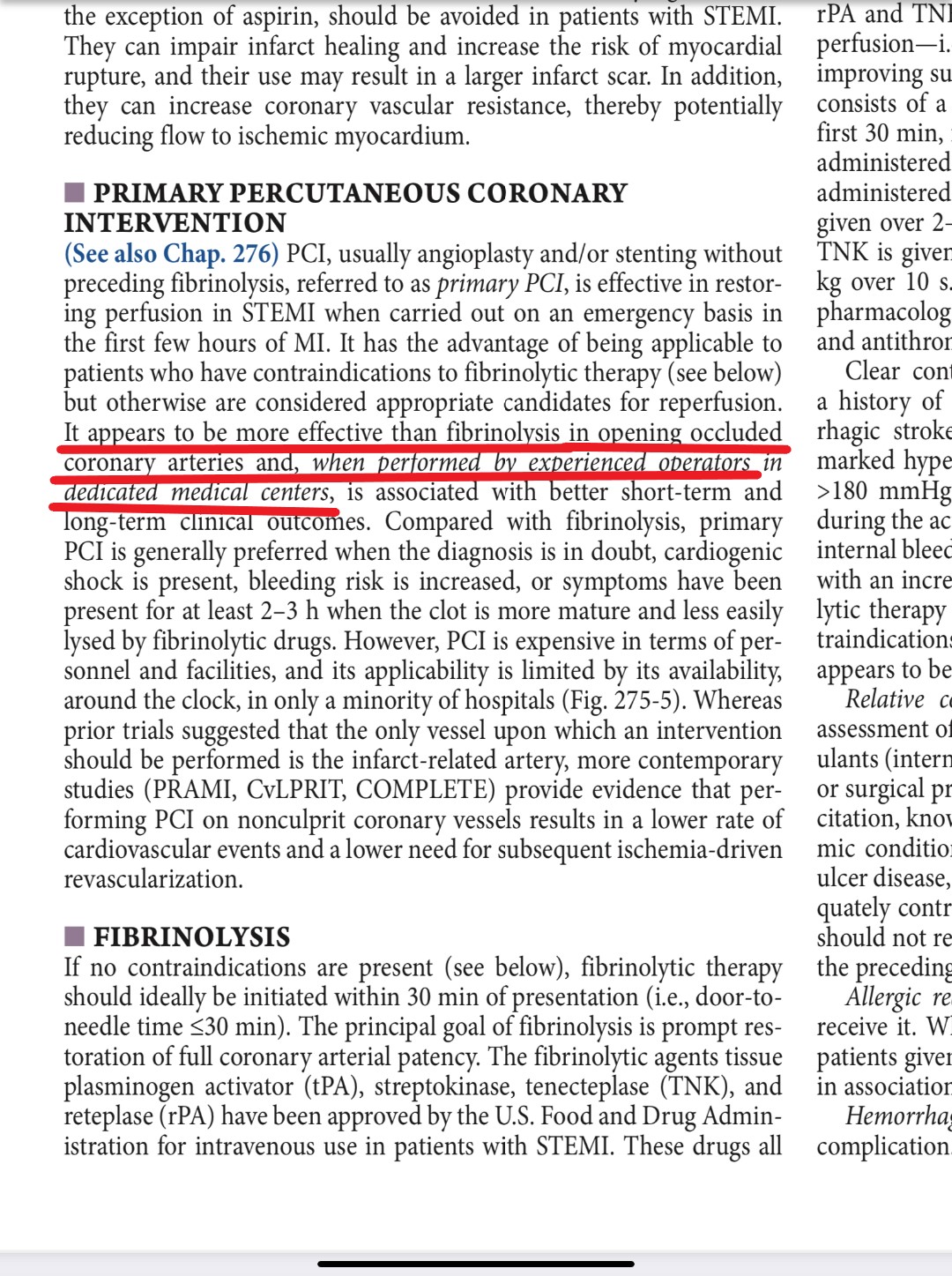
My hearty thanks to the editors of the chapter for the crystal clear expression about this much-debated procedure* and specifically choosing the word “PCI appears* to be more effective ” (even) if it is done in experienced persons in dedicated centers. The choice of the word used by the authors is Intentional and must be applauded. This message must be propagated to all our fellow physicians. What a way to convey an important truth pertaining to the management of the most common cardiac emergency, while many in the elite specialty are so dogmatic in their assertion without verifying the reality.
* The verdict is still under the jury even after 3 decades, since the PAMI days of the early 1990s. Thank you, Harrison. What a gentle, but a righteous way to express an opinion about a procedure that is apparently enjoying a larger-than-life image based on a handful of studies and a flawed meta-analysis.
Final message
Primary PCI is just an alternate form of treatment to fibrinolysis in STEMI. Both are equipoise in the majority of patients. Extreme care and diligence are required to harvest the small benefit the PCI seems to provide. There are lots of ” if and buts” that decide the success of this procedure. Get trained, and do it selectively for those who really need it.
Postamble
You may call yourself a super-specialist. But, please realize, If you have any doubt about key management strategies, never feel shy to take a cue from Internal medicine books. The greatness of these warrior books is that, it comes devoid of all those scientific clutters backed by premature evidence.