This is a 15-year-old post about LVH, written in 2008. Few of my colleagues, now agree with this, but still hesitate to oblige in the open, suggesting it is too good to be true! Re-posting it for your own assessment. Surprised, why cardiology community didn’t consider this observation worthy to pursue.
Advantages of Left ventricular hypertrophy (LVH)
Left ventricular hypertrophy is one of the most common clinical cardiac entity.It is recognised either by ECG or echocardiography.LVH has a unique place in cardiology as it can imply a grossly pathological state or a marker of healthy heart as in physiological hypertrophy in athletes.
Logic would suggest, in this era of stem cells and nano medicine , every muscle fibre in ventricle is worth in gold !. So when the nature provides an extra reserve of myocardium in the form of LVH one should welcome it, if otherwise not harmful.
Is LVH due to systemic hypertension benign ?
Not really, LVH has been shown to be an independent cardiac risk factor. (The famous Framingham study)Further LVH can result in diastolic dysfunction and the risk of cardiac failure increases.
But in spite of these observations, an astute clinician with considerable experience will appreciate , patients with LVH fare better during an acute coronary syndrome !
This has been a consistent clinical observation . (Shall we call it as class C . ACC /AHA evidence? )
Is LVH an asset during ACS ?
A hypertrophied heart takes ischemic injury very easy , it doesn’t really hurt much . Another possibility is that in LVH myocytes are relatively resistant to hypoxia .
Patients with LVH rarely show significant wall motion defect following an STEMI.This is probably because the full thickness transmural necrosis is almost never possible even if extensive MI occurs.
This is also reflected in ECG as these patients rarely develop q waves in following STEMI .
Persistent ST elevation and failed thrombolysis is very uncommon in pateints with LVH.
LVH provides a relative immunity against development of cardiogenic shock . It requires 40% of LV mass destruction to produce cardiogenic shock.This can rarely happen in LVH. In a long term analysis we have found none of the patient with LVH developed cardiogenic shock following STEMI.
LVH patients are also protected against development of free wall rupture.
Concluding message
“Lack of published evidence is the weakest evidence to dismiss a true myth”LVH , either pathological or physiological, has a hitherto unreported beneficial effect.It acts as a myocardial reserve and helps limit the impact of STEMI.
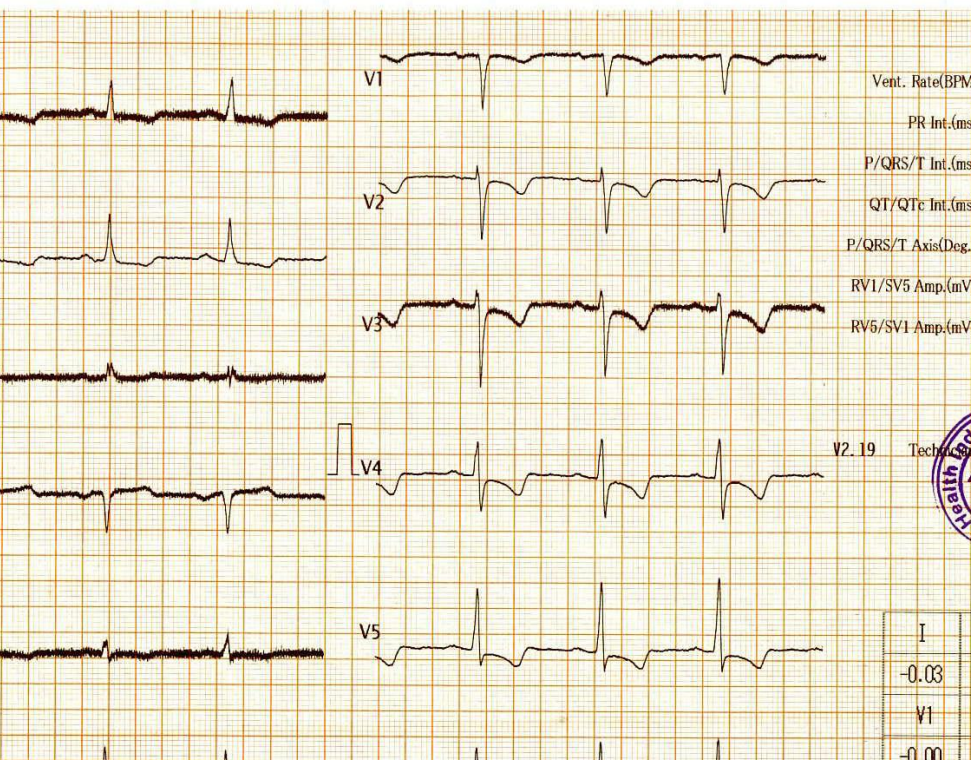
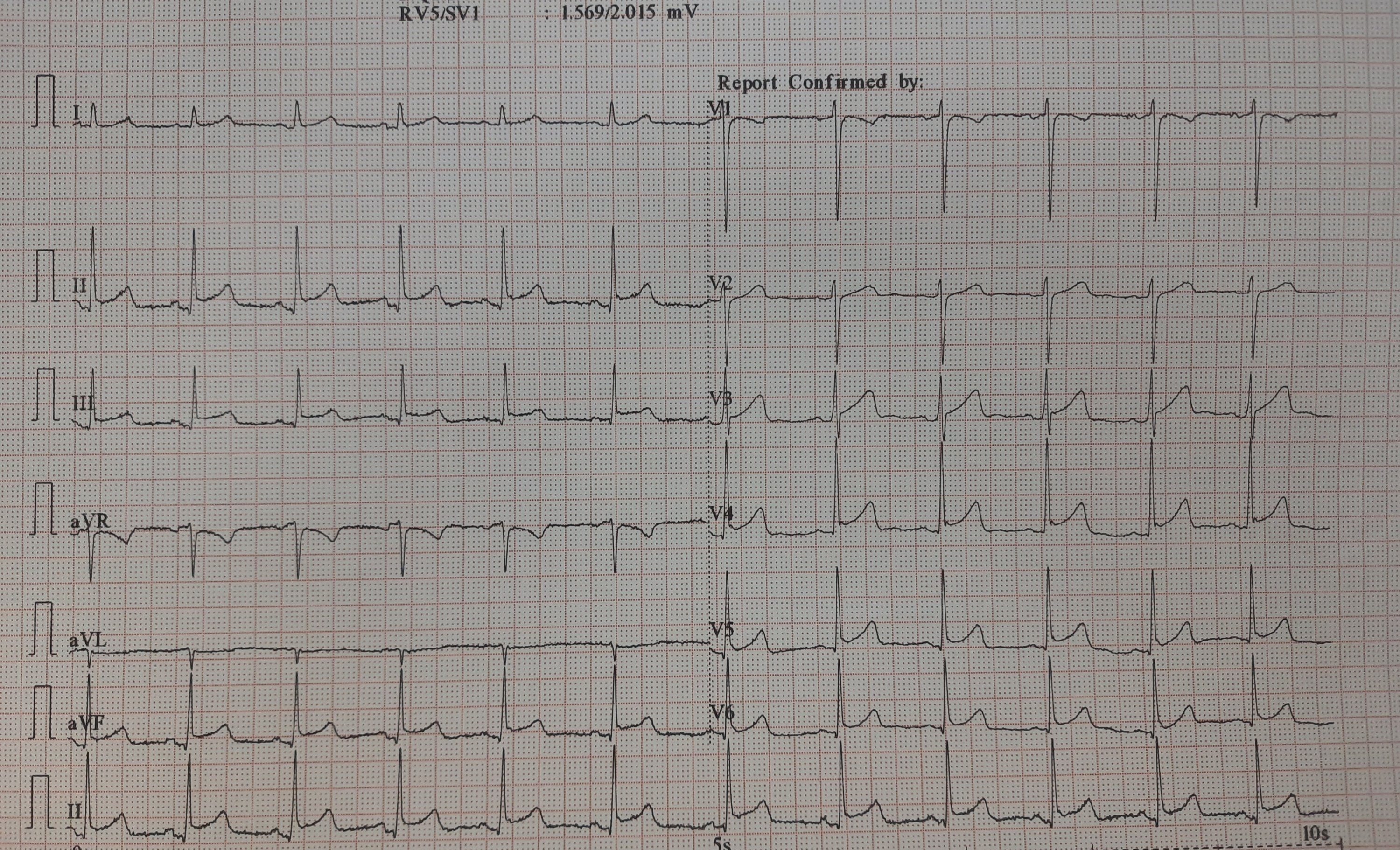
This is the Incidental ECG of an apparently healthy 50-year-old businessman, recorded while applying for health insurance
How will you describe this ECG?
Let me magnify it for you
Why this big fuss about this ECG?
Such ECGs are so common. Looking at the ST segment, we are supposed to think of significant CAD,, LVH,Aortic stenosis or variants of cardiomyopathy, and sometimes electrolytic shifts. The fact that it is recorded at rest, and the patient is absolutely asymptomatic, it is very unlikely there is ongoing ischemia.It could be a myocardial origin or an unknown repolarisation pattern. But, one thing is clear, we can’t send this guy under the label of non-specific ST/T changes.
The Echo was done it was normal. No WMA, LVH. The aortic valve was perfect.
Is CAG indicated here?
Three responses came from three different cardiologists. Everyone agreed, the stress test is not going to be useful, as baseline is unstable
Absolutely not Indicated, since he is asymptomatic. I believe the history and Echo. Please follow him up
A definite yes for CAG. (Being a scientific cardiologist, without excluding CAD, I can’t be at peace. Will do at least a CT angiogram)
A third cardiologist said a CTangiogram is waste of time and wanted to do a radial CAG in 10 minutes in his newly opened hi-fi radial lounge.
What happened then?
Don’t know, whether he underwent CAG or not. But, I can confidently say he will have a normal coronary angiogram. How can you be so confident? Confidence doesn’t mean I am correct. Look at the ST segment again. It is not true ischemic depression. It is neither non-sustained nor horizontal or downsloping*, This could be referred to as, primary T inversion with secondary ST segment dragging. Regarding the management, the first response is ideal,
*Classical slope should begin at J point. Late downsloping has little predictive value as in this ECG.
Is Echo good enough to rule out structural heart disease?
Even after the echo was reported normal, few questioned the quality of the echocardiogramand asked to look specifically for apical wall motion with speckle track and GLS. ( I know, MRI is a must nowadays to rule out structural heart disease as Echo can’t rule out intrinsic myocardial disarray, infiltration, etc)
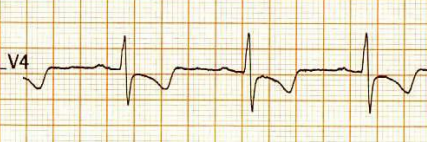
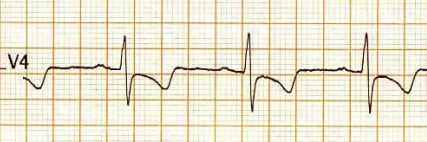
How is ST dragging different from ST depression?
Classical horizontal ST depression
ST dragging due to T wave pulling
For ST depression to happen, the junction point needs to be depressed. Note here junction is held high, only the distal half of the ST segment dips rather dragged by the phase 3 repolarization process which corresponds to the proximal limb of T waves. Our observation is, this type of ST drag is less sinister and usually indicates a myocardial ST defect, rather than an ischemic one. (Examples: concealed LVH or forme fruste of HCM or Infilitrative cardiomyopathy-related entities.)
Final message
The purpose of posting this ECG is, some ST segments create disproportionate panic than it deserves. The concept of T waves pulling down the distal part of the ST segment which can be called ST segment dragging is being proposed here.
Some provocation for advanced readers
Re-exploring the foundations of electro-cardiology is always welcome. Worth diving deep into mysterious terminology non-specific ST/T changes. ST segment in the ECG corresponds to the most stressful period since it represents the active part of mechanical contraction. Curiously, it Includes the entire electrical (Repolarisation) & most parts of mechanical relaxation. The true onset of LV myocardial mechanical relaxation we can’t be sure, It happens somewhere in late phase 2. I think it’s so difficult to decode that timing. But, what we can presume is ST segment behavior in its distal half is less specific for both ischemic as well as hemodynamic stress
The electro-mechanical continuity within the ST segment is so intimate, and the demarcation point between them is invisible in many clinical situations. No surprise, we are largely in the dark about the true influence of the ST segment over T wave morphology and vice versa. (ie distal ST depression pulling down the T wave ) Though chronologically T must follow the S in timing, it would seem impossible for “T” to go back in time and pull the ST down. (If QRS can precede P in a junctional rhythm, why not T do the same for ST? ) I am not sure whether there is any timing involved in antegrade vs retrograde repolarisation across endo-epicardial repolarisation dissociation.Further, we know very well, myocardial scars cause fragmented depolarisation in QRS. Can anyone guess effect of these scars in repolarisation vectors? (Fragmented ST segment ?) I think it is worth pursuing this phenomenon. Let the young new age Sodipellares’ look into this.
Though the traditional rule of thumb, makes ST segment shifts more sinister, T-wave changes are largely benign, It is not an easy job to segregate benign from more serious forms of T-wave changes. Isolated new onset T inversion, can be an equally troublesome marker, especially mid-chest leads in the male population.
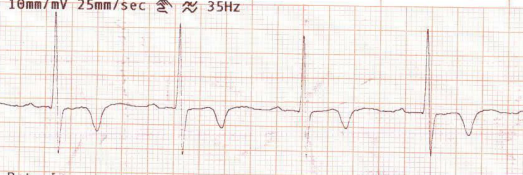
It is interesting to note, not every T wave Inversion is empowered to drag the ST segment down. We don’t know why. It is something to do with the curvature of the shoulder zone of phase 2 /3 of the action potential. In this context, ST dragging could be an important concept to explore.
. An example of isolated T inversion without influencing the ST segment. Try to compare this ECG with the one that is shown to drag the ST segment
Diastolic T wave stress
One more issue, which we are not yet clear is the timing of 2nd sound with reference to the T wave. It is a fact, a significant part of the T-wave will represent early diastolic hemodynamic stress* as well.
If some body is struggling with same problem, say for over three decades , there is something seriously wrong with the way we deal with the problem. How do you localise accessory pathway in WPW syndrome from 12 lead ECG ? is one such entity, This question is asked exclusively in cardiology board exams. Now a 2023 paper from EUROPACE claims, it has come out with a simple algorithm bettering all the previous ones. Please check it for yourself.
One thing we can say with conviction is most of these embryological remnant pathways are posteriorly or laterally dragged in peri AV annular region or the para septal region. Very few appear anteriorly, if anterior it is more often placed on the right side.
Why should we take this question easy ?
Try asking any experienced EP specialist* to localise a pathway in given 12 lead ECG . Don’t get surprised by a long silence before they commit, because they know the truth, and how delicate this question might sound on quiet a few occasion, because of various anatomical and physiological reasons.
*Never fail to appreciate their hard long hours in cath lab to spot, analyse and shoot these tracts.(EP stuff is not like angioplasties, which, many can do even in half sleep!)
Final message
Yes, localising WPW can be either a fascinating or frustrating exercise depending on our understanding about the attitudinal cardiac anatomy, variable autonomic tone dependent morphological behaviour of delta waves, PR intervals, QRS axis ,the transition zones etc. Shrewd fellows may go through this 12 lead stress test. ,
For others just try to localise right from left , & then posterior or lateral Forget the anterior ones. This is more than suffice. Unlike drug trials, where statistics are often battered , here the Incident numbers are the key measure of truth. (Even without seeing a ECG you are likely to be correct in 80 % times, if you localise the pathway to posterior, para-septal or left lateral zones. )
A 62-year-old man who is being scheduled for prostate surgery with no cardiac risk factors or comorbid status came for surgical clearance. I examined him and took an ECG, everything was fine and gave him clearance for surgery.
I was surprised to spot him the very next day, waiting in the lounge of my office. He said, his anesthetist was not happy with my pre-op-cardiac assessment report, suggested it was incomplete, and sent me back for echocardiography to know the LV ejection fraction.
I wanted to clarify with the patient, what exactly happened when he met his anesthesiologist.
“I am not sure doctor, the moment he saw your report, he called my urologist. I overheard his call, they were discussing the need for an echocardiogram and they were also wondering, how could a cardiologist give a surgical clearance without even an echocardiography”.
I wasn’t really surprised by the turn of events and told the patient.
“I am experienced enough to say, your heart is 100 % normal without an echocardiogram”.
“I understand doctor, but sorry to bother you. Can you please take it for the sake of my anesthetist and urologist, after all, right now I am worried about their peace of mind”
“You are absolutely right. This is a topsy-turvy world. Investigations are dictated to me in my own field of expertise. Anyway, I am not a fool, to expect a patient’s help to guard my principles of practice. Please check in, let me do the echocardiogram as they wish”
“Thank you so much, Doctor“.
I showed him, the vigorously contracting ventricle and taught the student trainee who was nearby, a simple clinical tip ie, a loud first heart sound on auscultation is good enough to tell you, the EF is beyond 60% in most situations. (A forceful AML movement is a direct auditory marker of EF %)
Final message
It is getting more & more clear, physicians will face huge hurdles in applying their clinical skills to practice. They may even be unauthorized to do so. It seems, in our misplaced quest for perfection, we have fallen into a scientific trap, that every clinical decision must be authenticated by some objective lab-made obsession. The word clinical acumen could soon become a laughing stock, as AI-powered medical zombies are waiting to join our consultation suits.
(Meanwhile, the guidelines are very clear. (Read below) Do echo only in high-risk surgery, if patients’ functional capacity is poor. But, let me confess, at least in our part of the world, we are happy to violate standard guidelines without any degree of guilt )
This is an ECG of a 25-year-old, recorded in master health check-up.
It would be mind-boggling to know the prevalence of such ERS patterns in the general population. One estimate suggests it could be anywhere between 3 to 13 % depending upon the criteria used. Let us assume the mean as 5 %. Then, it would be 30 crores of human beings in our habitat show this ECG pattern. If applied, in my city Chennai alone 5 lakh people could carry this tag.
While it is true, some forms of ERS and J wave syndrome can be markers of serious ventricular arrhythmias, either spontaneous or at times of Ischemia. Currently, It has become a fad, in cardiology academic circles*,to propagate the idea that ERS is no longer a benign condition. This is not acceptable at any degree of cognition. This happened mainly after few studies in powerful journals created some alarmist views. (*Maybe there is a bit of truth there. I still have doubts about whether we interpreted the Michel Haïssaguerre study properly)
Final message
ERS is a widely prevalent normal ECG variation with a minuscule risk. High-risk subsets need to be screened only if the J waves encroach and spill dangerously into the ST segment as well. Of course, this pattern is of serious concern if there is a family history of young SCDs has occurred.
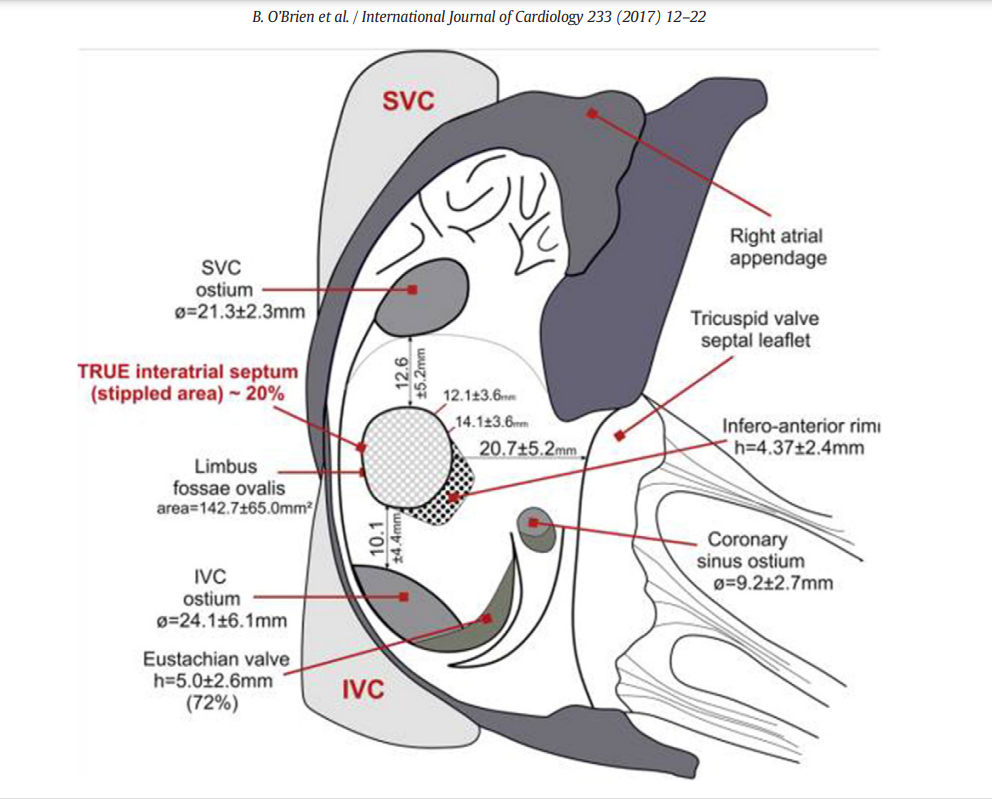
The main reason for all those jitters, we cardiologists, get every time we puncture the IAS is not due to a lack of expertise and experience perse. There are two more reasons. First and foremost, it is still largely a blind* procedure. (Even in this era, where drones with HD vision shoot one-meter targets from a 1000 KM range ) *TEE and ICE are there, but they rarely give enough confidence.
The second reason is more important and is rectifiable. It is the perception error in our anatomical cognition, that is fed to us from first-year medical school. We are made to believe (at least to people like me ) The right atrium is aligned like a perfect box on the right side, sharing a wall called IAS, and the left atrium is obediently placed left of the right atrium. Please realize the heart is such a complex twisted single tubular organ, the venous end, in a stunning backward loop brings the LA most superior and posterior to the right atrium overriding the left-right relationship.)
The right atrial terrain and IAS with multiple bumps and holes. Note the true IAS constitutes only 20% . This is where our punctures need to be.
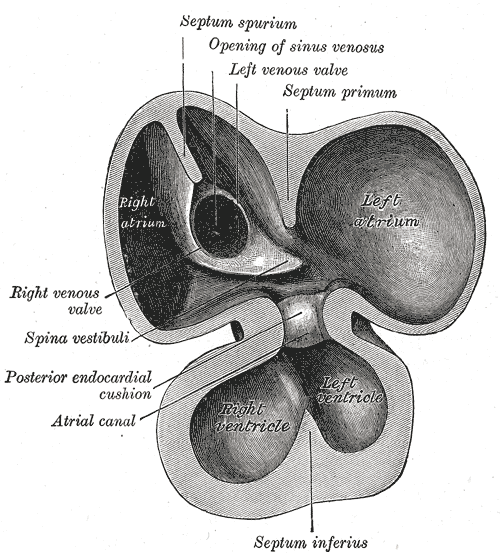
Development of IAS
IAS development and the number of layers it sandwiches, the tortuous tracts of PFOs, the fossas, and its variable limbus is a big topic. Further, It is worth recalling, the true IAS hardly forms 20 % of the area of the interatrial contact surface.
(the differential regression of sinus venous, along with infolding of the roof and along with curious septum spurium , the ubiquitous septum secundum make the texture, area & shape of IAS, a fascinating creation, though troublesome for the cardiologists ! ) Whoever named that part of vanishing IAS as spurious, (I think it is Henrry Grey ) has much fore-vision.
Forget about all this. Tell me how to cross this difficult terrain
Coming to the real world of interventions, we need to do targeted punctures in different spots of IAS in various interventions.(Mitra clips, LAA device, PTMC, PV abaltions, Mitral paravalvular leaks , TMVR etc) This has made this task even more tricky. Experts are always there to help us out. Like swimming, it can never be learned in books.
This 19-minute clip from. Seoul, South Korea is an excellent resource. Thanks to Dr. Sang Weon Park
Along with sound anatomical knowledge, improved hardware, and imaging like deflectable sheaths, TEEs, and ICE (intracardiac echo ), let us hope, it will soon become an easier task for everyone.
Final message
Understanding “attitudinal cardiac anatomy” with fluoroscopic overlay is the key. Again, it needs to be stressed, “Right is not right, and left is not left” when it comes to true atrial geo position. LA is equally posterior, superior, and of course to the left of RA. Some of my colleagues are blessed with a special 3-dimensional skillset (Inherited ?) I failed miserably to understand this, till very late. I am sure, Dr. Park’s video will help all our youngsters to cross the difficult gateway to the left side of the heart.
Fibrillation is a continuous, chaotic muscular activity. In AF, atrial muscle is expected to lose all coordinated contractions with fibrillatory waves replacing P waves. Have you ever spotted a suspicious P wave in a strip of otherwise explicit AF? If not, this write-up is not for you.
An evolving rare theme in Atrial fibrillation
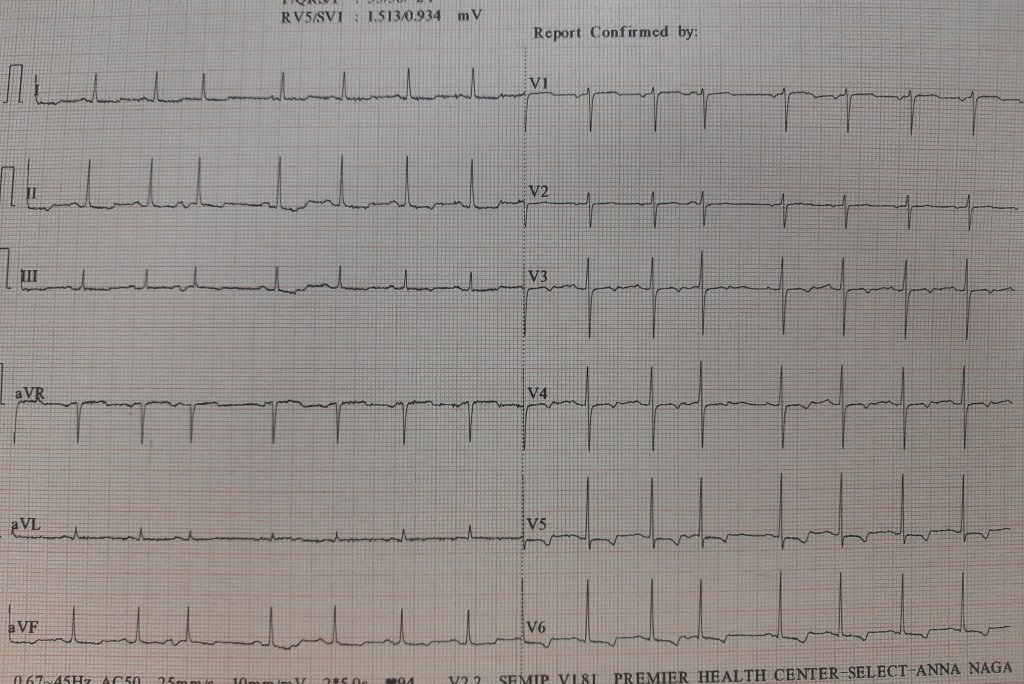
Have a look at this ECG
Here is an ECG, that was reported as AF, multiple APDs, or Possible AF, Pre AF. I suggested the term AF in transition. While few agreed, many said it is a straightforward SR with APDs, making it appear irregular RR.
But, the fact of the matter is, ECGs are insensitive to pick all fibrillatory wavelets. It can selectively pick a few coarse F waves and make them appear as P. I think, in this era, we should not diagnose AF by proxy, ie absent P waves. Rather, we need to look actively for fibrillatory wavelets. (Imagine all sinus arrests will qualify for f fine AF with a slow ventricular rate is it not ?)
The semantics of AF nomenclature is long. Intermittent AF, and paroxysmal AF, are well-known entities. It is now clear, AF can occur for a few seconds and vanish too. It seemswe need to play some more linguistics with the most common cardiac arrhythmia. (Non-sustained AF, evanescent AF, etc )
Some thoughts on this hide & seek P waves
Apart from the conventional list of absent P waves, one more example is repetitive APD can stun the atrial muscle for a few moments or minutes.
Then, we always have the issue( eluded to earlier) of sinus node paralysis, with irregular junctional escape mimicking AF.
Amiodarone can reduce fibrillatory rate, and (AF cycle length ?) Coarse F waves slow and stabilize it to mimic an organized P wave
P on Ta waves (Like R on T ) can trigger a nonsustained AF for a few moments in a functional manner without real pathology in atria.
A funny memory brings back an EP truth
During our student days, my Professor used to trap us with this question, Which atria would fibrillate in mitral stenosis? Many of us blinked, and few had no hesitation to say, it is the LA that fibrillates. Now, after 50 years we realize, how fascinating the secrets AF has unfolded. Some organized activities are often in the right atrium, even as LA begins the process of AF. It is possible it may take variable time for the left atrial chaos to spill over to RA*. During these electrical uncertain times, some of the right atrial P wave activity refuses to die down. Even more dramatic one Atrium alone can permanently fibrillate and others completely insulated by blocking the signal in the Interatrial pathways. (Ref 1 ) Ndrepepa’s paper in the JCE 2000)
Final message.
True scientists rarely bother about questioning a dictum. The concept of non-uniform AF was first thought of by (Schrmp et al Ref 2) 100 years ago in 1920, and Zipes(Ref 3) hypothesized this in 1973. now, in the Year 2000, Ndrepepa confirmed it with EP studies. The spotting of occasional P waves is not forbidden in AF if the contralateral atria decide to block the incoming AF signals and keep generating their own P waves
Young EP guys, now that you are equipped with the sophisticated intracardiac GPS, please pursue this provocation in AF. One more piece of evidence we observed in the echo lab. Try to look at Tricuspid doppler A velocity waves in full-blown AF patients. You can see the surprise for yourself.This is very good research work to do. This is one of the ideas I gave to my fellows at MMC. Now, it is free for all to pursue whoever wants to do this. The clinical implication* will follow.
* A lingering query, how common is RAA clot in mitral stenosis with AF and the possible threat of pulmonary embolism?
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.