Corona has triggered the scare of the century, even among the scientifically savvy brave men & women. The scale of the panic was unprecedented. However, one positive outcome of this pandemic was, this 20 nm RNA particle forced many of us, to ponder over the true purpose of life. It demanded a course correction in those who found one. Now, after 9 months Corona, in its second wave seems to be somewhat kind to humanity. The case fatality rate is dropping to nearly one-tenth of its peak in the first wave.
Where is the evidence coming from?
Apart from our own personal experience from 1500 bedded corona hospital, this paper reports data from 53 countries.
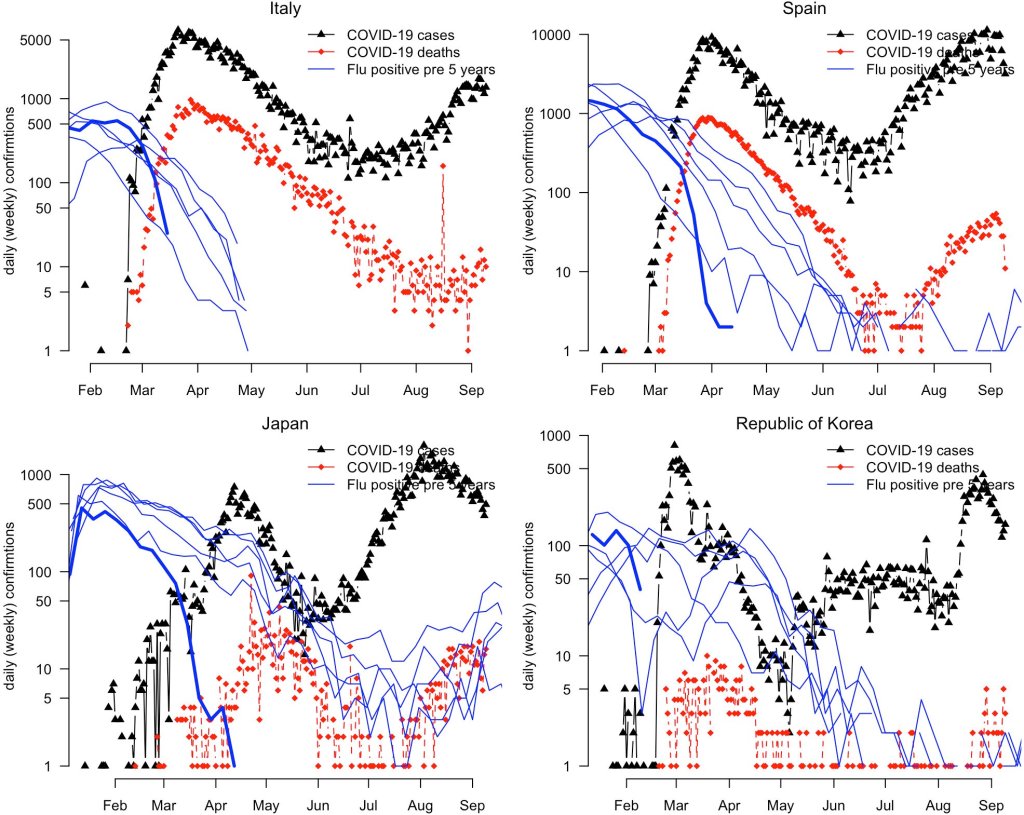
Note, the red covid mortality curves are not matching the black positive waves (Both Europe and Asia)
Link to the original article https://doi.org/10.1111/tbed.13819
The possible reasons for the low case fatality rate.(Personal observation)
- Viral apologetic behavior*
- Second wave affecting more healthy younger who fight it better.
- Less panic in the health care delivery system
- Though there is no specific therapy, at least some basic treatment strategies are in place.(Timely steroids & mindful oxygen did the trick)
- Initial aggression out of Ignorance (ie ventilator deaths) has largely ceased.
- RT-PCR(which helped In diagnosing /isolating ), CT scans,(helped in grading) the Remdesvirs(gave peace of mind ) the Tocilizumab(did nothing great ) has at best played a minuscule role at a huge cost.
Among all these factors, which do you think is the most important contributor to a declining fatality?
The single important factor could be, “The virus has decided unilaterally to forgive the frightened human beings, and become less virile“.(At least in those people who sincerely respected the viral might by wearing masks and other paraphernalia) Sorry, for uttering this forbidden stuff in science, still it could well be the truth.
If corona is losing its sting & steam what would be the realistic role of the vaccine? What is the likelihood of vaccine getting false credit*?If we are allowed to be optimistic, Corona in all likelihood is waiting to say goodbye after a feeble third or fourth wave. All these are speculative, still, one thing looks positive. Unlike the much-quoted fact about the Spanish flu of 1920, which resulted in more damage in the second wave, which is unlikely to happen with corona.
Disclaimer
* This article never intends to undermine the importance of preventive measures and vaccines for this worst pandemic in recent human history.
Counterpoint
The decline in case fatality is may not be uniform as fresh data from Europe suggest. It’s hyperbole to expect corona’s second wave to bring good news. It is largely left to the people’s behavior to contain the pandemic than to get a pardon from the virus.