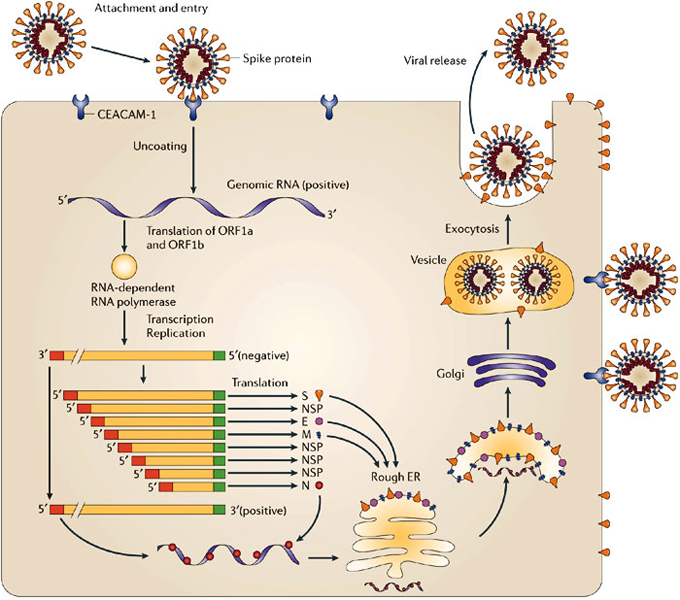
Viruses are essentially lifeless molecules (A nucleic acid RNA/DNA) .In the case of CoRoNA, it is the inbuilt RNA that acts as a commander in mischief. Ironically, it gets to life only when it attaches to the host cell. How a small bit of nucleic acid with a lipid cap infects a cell and becomes a deadly factory of new viruses and spread through the body remains a deep biological mystery.
Someone asked me , “Can we kill the Corona en masse”? The answer is frighteningly simple, we can’t kill them really, because they don’t have life in the first place. At best, we can deactivate or make it dormant and reduce its spread.
I just got contaminated with coronavirus . . .Is it a death sentence?
Even if you forcibly feed COvid 19 at random to 100 persons 80 % will be near normal or with a mild respiratory infection. You may wonder how can so many people are positive for Covid 19, and comfortable. We are still far away from understanding the complexity of how this virus will behave in a given human body.
This is because we are not clear what is the exact port of entry and how the first cell reacts to it.The way the body deals with it is entirely different if it attacks the respiratory tract through aerosol or it enters gastric tract (Imminent death with acidic PH ? we don’t know )
The mysterious interaction of genetic susceptibility, response to initial entry, epigenetic memory and subsequent immunological activation, will determine whether one is going to get simply infected and completely decimated.
Healthy humans enriched with good protein diet are expected to have good immunity. However, it can never be foolproof. It is obvious, there is something more than a host stress response readiness.(The fighting power and the fitness of your Immune cells T,B ,K,NK cells, infinite number of Interstitial scavenger cells and molecules)
When you are stressed the Immune system is activated or deactivated?
As expected the answer can be both. Then, how does the body will fight it over? Cells start synthesizing defense molecules. Unfortunately and paradoxically, cortisol is a major hormone released at times of emotional stress, that can severely compromise the immunity. Steroids are firefighters but cause collateral damage.
So its easy to conclude, positive emotions have positive immunity and negative emotions like fear, anger, distress can pull our immunity down.
Fear is a thought virus
Technically and biochemically, every human thought is a neurotransmitter. A neurotransmitter is nothing but a chain of amino acids synthesized in response to DNA/RNA codecs. So, straight away there is an obvious link between thoughts we harbor and the fighting power of the body. Why depression and anxiety affect the infection rate ?
The effect of various emotions on the Immune system is a big emerging topic. Fear-mongering about Corona and the manic digital dissemination of the virus of fear could turn out to be a great Immune system dampener.
One of my wonderfully healthy friends wanted to estimate the fighting power of his body’s immune system in case he is affected by Corona. He asked, whether his blood can be mapped and give a reassuring report?
I said no, it is not possible. Just take all the precautions. Reassure yourself that you have all the Immunity to fight. That’s it.
This following article elegantly explores the link between emotions and Immune response.
Final message
Can viruses befriend “fear” that reduces host Immunity and help self propagate? No one can be sure. But, I wish “unrestricted courage” acts as a vaccine to Corona, which can ooze from the brain free of cost.
Postample: What will happen to this pandemic?
It will (and should) settle down taking its toll. Preventive measures are gratifying. We need to learn from China, how they blunted the steep ascending curve of propagation.(Of course it started from there)
Who is responsible for such global pandemics?
I am sure, this is the toughest question, probably with no answer. Is it man-made or God made ? If you strongly believe, God will never punish human beings without a reason, then the answer is simple. Now, the world is under freeze. Its one way of arresting the mad growth of artificial,materialistic, biased economy. Corona could be a whipping force on mankind and let us use it to heal and unite fellow human beings.
Now, some positive news from CoVid 19 positive population
The false positive results are too high with currently done active screening tests.
This study from China says positive predictive value of a positive test is just 19% .It would mean 80% error rate. So, don’t really get unnerved with a positive test.
https://www.ncbi.nlm.nih.gov/m/pubmed/32133832/