Posted in Uncategorized | Tagged evidence based medicine, future of medicine, inappropriate scientific growth, medical education, medical ethics | 2 Comments »
Dizzines , giddiness , light headedness , fear of fall or true fall (Syncope) are the most common symptoms beyond middle age .They usually end up with consulting physicians , neurologists and cardiologists .Cervical disc is commonly blamed for this.While all these symptoms can be a manifestation of cervical disc , true syncope seems to be rare with cervical spinal disorder.
 Why true is syncope rare with cervical spinal narrowing ?
Why true is syncope rare with cervical spinal narrowing ?
There is a fundamental ignorance here. We are not yet clear whether giddiness /dizziness is neural or vascular .(Or combinations of both ) in cervical spinal disease.
Many of the patients experience momentary unsteadiness and feel like falling but very rarely end up in a fall or syncope.By definition syncope requires global transient hypoperfusion of brain to trigger a fall .
Cervical canal carries only the vertebral artery .Both internal carotids are no where near the spine. So, however severe the vascular compromise within the cervical canal , syncope is unlikely as anterior cerebral circulation compensates at the level of circle of Willis. Is that the correct way of reasoning ? Unilateral vertebral compromise rarely matters as other side takes care.It is very unlikely both vertebral artery get compromised by cervical spinal spurs simultaneously.
How many seconds of vascular compromise is required to produce syncope ?
Brain seems to be a funny and sensitive organ .In erect posture it is very sensitive. It reacts in a fraction of time for any transient reduction of blood flow.The same cardiac events which can cause symptoms of impending syncope in erect posture is quiet comfortably tackled in recumbent posture .
In erect posture , blood pressure need to much higher to get it pumped above the heart against the gravity. Though , it seems absolute blood pressure and cerebral perfusion that matters, there is something more we are missing. The brain-stem -vestibular system perceives differently when a recumbent person develop cerebral ischemia than when he is erect . The reflex circuit that activates on/off switch for abrubt loss generalised muscular tone is not yet been identified .
It is a biologically heartening irony that syncope is a natural counter mechanism by which the organism assumes instant recumbent position to maintain perfusion of brain .A fall promptly does this.(Ofcourse with a risk of Injury )
We think more than 3 second pause will initiate a syncope circuit .But it is not a fixed number. Some can tolerate up to 5sec or even more especially in lying posture.
Final message
Syncope , as such in isolated cervical spondylosis is rare even though it can potentially interfere with the vertebro basilar system .Why the vascular compromise almost always fall short of syncope and end up with just momentry unsteadiness is not clear.
Further queries to be addressed
Is dizziness, giddiness , presyncope are vascular or neural event?
Can vertigo occur with cervival spine disease ?
Posted in Syncope | Tagged cervical vertigo, mechansim of syncope in cervical spondylosis, syncope evaluation, syncope in neck compression | Leave a Comment »
Every time , patients ask me what diet he or she should follow , Iam sort of amused , as my understanding of diet and cardio vascular disease is at best primitive.I used go with a standard single phrase advice “Anything in moderate should be okay “
What about going for a saturday night party doctor? One of my shrewd looking patient who was recently double stented with DES , asked.
Human body is a biological marvel.While medical professional divide it into various systems for our convenience. God doesn’t think that way .He has no systems in mind when the body was designed . There is no wonder , the alimentary system and hematological system has to interact on a daily basis with the help of circulatory system to keep the body alive. Platelets are unique blood cells that exist primarily to plug physiological bleeding if any or for self-healing at sites of tissue injury.

With human vascular system increasingly invaded by various metals and wires , platelet are a confused lot since their original biological functions are altered. They simply don’t know whether fight these foreign body , aggregate over it , flush or simply pass over these .Adding to this the powerful anti-platelet drugs targeting critical functional pathways .No wonder every other cardiovascular patient consumes at least one anti-platelet drug.
It seems diet can have direct influence of platelet function
With human beings desire to add style to food consumption and eating habits competing with top slot of purpose of living , we often forget it is same prevent us from living a good life.
There has been numerous anecdotal and study population and experience acute coronary events are more common after a heavy meal especially a fatty one .The immediate suspect has been high triglyceride and chilomicrons in blood stream shunted intestines .
It is logical to expect , these high TGLs some how act a s trigger for pro-coagulant trigger .With the core thrombus rich platelets it is assumed platelet stickiness is augmented and maintained by transient raise in triglyceride formation(Reference 1,4,5)
Glycerol component of TGL is know for its sickness and making the companions wet.
The million dolor question is , at what level of TGL and which forms of TGL make the platelet cry and attract each other ?
Diet, anti platelet drug efficacy ?
Now , patients with coronary stents has to live at the mercy of these anti-platelet drugs. The drug resistance(Clopidgrel) is threatening to be major issue.Like warfarin do we have real issue of dietary binge and acute neutralisation of anti-platelet drug efficacy that can trigger acute stent thrombosis . This is potentially important area of study .
Final message
So does a fatty meal a new trigger for ACS ? It may sound an alarmist statement .but as of now , its difficult to ignore this.So my advice for that the that smart young man with soluble stent was to avoid binge dinners that carries a definite risk of interfering with stent maintenance .
Reference
6.Fuhrman B, Brook JG, Aviram M. Increased platelet aggregation during alimentary hyperlipemia in normal and hypertriglyceridemic subjects. Ann Nutr Metab. 1986;30:250–60
8.Platelet lipoprotein interplay: trigger of foam cell formation and driver of atherosclerosis Siegel-Axel D1, Daub K, Seizer P, Lindemann S, Gawaz M.Cardiovasc Res. 2008 Apr 1;78(1):8-17. (Free full text link)
Posted in acute coronary syndrome, atherosclerosis, platelet function | Tagged platelet adhesion and aggrgation and fatty meal briyani, platelet stickyness and dietery fat, platlet anf fat ldl and triglycerides, tgl mediated platlet aggregation | Leave a Comment »
What are the mechanisms of cyanosis in cyanotic heart disease ?
Most of my fellows have difficulty in answering this question. (It is not the lack of knowledge though !) In my view ,cyanosis can occur , by six different modes
- Reduced pulmonary blood flow with some form of anatomical obstruction in RVOT with a communication between ventricles (TOF physiology ) , atria or both
- Reduced pulmonary flow with obstructive pulmonary vasculature (Eisenmenger physiology )
- Wrong way origin ( RV to Aorta/LV to Pulmonary artery ) : Transposition physiology
- Simple mixing of arterial and venous blood channels within the atria ,ventricle or great vessel without RVOT obstruction .This, in fact can causes increased pulmonary blood flow (Technically left to right shunt ) and still there is cyanosis (These are called as Admixture lesions ) It is also to be noted some of the admixture lesions (Truncus, DORV,etc ) the mixing takes place only during systole , while TAPVC,Common atrium, Tricuspid atresia* admixture is more complete as it happens during entire cardiac cycle.
- Isolated Right to left shunt are very rare ( Pulmonary AV fistula , SVC to LA )
- Complex combination of first 4 (Like bi-directional shunting , TGA combines , AV canal defect , with varying degree of pulmonary obstructive disease) Note : TOF and Eisenmenger are physiologically mimic each other , the only difference is site of resistance to pulmonary flow. RVOT vs Lung vasculature )
* Essentially Atrial admixture is more complete than when it happens at ventricular or great vessel level
For advanced readers only
Now, is it possible for “Net” left to right shunt to result in cyanosis ?
Yes*.Very much possible. The bulk of this group is referred to as admixture lesions with certain caveats.There should be an obligatory mixing without contribution from RVOT obstruction or raised PVR( *Please note theoretically admixture can either be right to left or left to right shunt )
All pure admixture lesions are in fact net left to right shunts. (TAPVC, Single ventricle , Common atrium , Common AV canal ,Truncus, ) This is the group we have been traditionally calling cyanosis with increased pulmonary flow.
Its may also to be noted with surprise some admixture lesions often has less intense cyanosis than other forms as long as pulmonary blood flow is normal and the lung does its job perfectly .
*Please note Isolated classical left to right shunts , ASD, VSD, PDA can never cause significant cyanosis unless there is reversal of flow .However ,many Eisenmenger physiology show net Left to right shunting only ( 1.2-1.5 : 1 or so ) but with a definite right to left component .What we call as typically bi-directional shunt .
How can cyanosis be minimal even in some cases of single ventricle ?
- Even though there is single ventricle , there can be preferential (favorable) streaming of right heart blood flow without gross mixing .
- As discussed before good uninterrupted pulmonary blood flow will make the cyanosis less intense .
Is single ventricle with PS admixture lesion or TOF physiology ?
Though single ventricle in isolation is an admixture lesion, when it has associated RVOT obstruction it ceases to be admixture by definition as mixing is augmented by the obstruction rather than by simple mixing.The complexity could be understood in certain situations where admixture lesions like common AV canal go for raised PVR .Here the various quantum of contribution to cyanosis is mind boggling. (Original admixture, augmented by RVOT resistance, differential mixing at atrial and ventricular level , hypoxia at lung level due micro pulmonary AV fistulas in grade 4 heath Edwards etc )
Role of streaming in Admixture lesions
Streaming is selective flow of venous blood into PA and arterial blood into Aorta even in the presence of large septal defects. Favorable streaming implies good systemic saturation. Unfavorable streaming would mean PA saturation more than aorta.(It should be noted streaming and good admixture don’t go together. If good admixture has happened there can’t be any streaming and vice versa)
Streaming is common in which situations?
Inspite of absence of IVS, streaming has been noted in some cases of single ventricle with minimal cyanosis with good saturation in Aorta.
Streaming in TAPVC has some unique features.
Fetal circulation has certain preformed pathways. IVC blood deflects to LA through ASD/PFO .SVC blood preferentially enter RV-PA. In Infradiaphragmatic TAPVC where it drains into IVC highly saturated PV blood may stream into LA thorough ASD and reach LV nd result in higher Aortic saturation.(This is in contrast the classical type of TAPVC draining into RA with little favorable streaming and hence O2 saturation equilibrates between PA/Aorta.)
In Supra cardiac TAPVC that drains into SVC or coronary sinus the streaming is unfavorable as it may preferentially cross tricuspid valve and enter PA making the saturation higher than Aorta.
Streaming is less common in which lesions ?
In common atrium and TAPVC draining into RA streaming is less common.In tricuspid atresia streaming is almost impossible as TV is non existent and this ensures complete mixing in the atria and hence cyanosis is likely to be severe.
Can TOF behave like an admixture lesions ?
Technically yes.If the RVOT obstruction is minimal ,(What was called then as pink Fallot ) We haven’t understood this entity properly for so long. Atleast I was baffled to read when J.K Perloff mentioned in his book during my DM fellowship days, that TOF can manifest with predominant left to right shunt with little or absent cyanosis.
The aortic override in TOF facilitated by large malaligned VSD make it a sort of admixture situation as RVOT resistance is too little to offer any resistance, (rather it welcomes more blood from left side ! ) So , should we call it simple VSD physiology , admixture physiology or just acyanotic forms of TOF ?)
Key points
Though admixure lesions are discussed separately , bulk of them actually represent cyanosis with increased pulmonary blood flow situations.
The net pulmonary blood flow is much more important than the quantum of admixture in determining the degree cyanosis
Finally , one should appreciate there can be combination admixture lesions with obstructive RVOT components . (Tricupid atresia+Pulmonary stenois )
Further reading
An excellent review article on this rare topic of admixture physiology
Posted in admixture lesions in cyanotic heart disease, cardiology -congenital heart disease, Tetrology of Fallot | Tagged admixture lesions in congenital heart disease, can left to right shunt cause cyanosis ?, mechansim of cyanosis, mechansim of cyanotic heart disease, what is admixture lesion | Leave a Comment »
On this special day , wishing all the readers and followers of this blog an energetic, creative , insightful and of-course a happy new year 2016 !
Just wanted to share the 2015 annual report of this site with the readers.
Posted in Uncategorized | Tagged 2015 annual report dr s venkatesan | 1 Comment »
Metformin is one of most commonly used oral hypoglycemic drug listed by WHO as an essential anti diabetic drug. .It is a biguanide which blocks the hepatic gluoneogenesis . Since lactate is the major substrate for the process of gluco-neogenesis , excess of which spills into blood .Lactate is swiftly cleared by the normally functioning kidneys .Metformin is completely excreted by the kidney. Hence in patients with compromised renal function (or when contrast agents compete with Metformin in renal excretion ) high levels would not only cause lactic acidosis (> 5meq), it can also aggravate contrast induced renal injury resulting in a downward hepato -reno-metabolic spiral.
Though the incidence of Metformin induced Lactic acidoss is low , the outcome can be bad , hence the concern. The European society of urogenital radiology has provided clear cut guidelines regarding Metformin usage when contrast agents are being used.
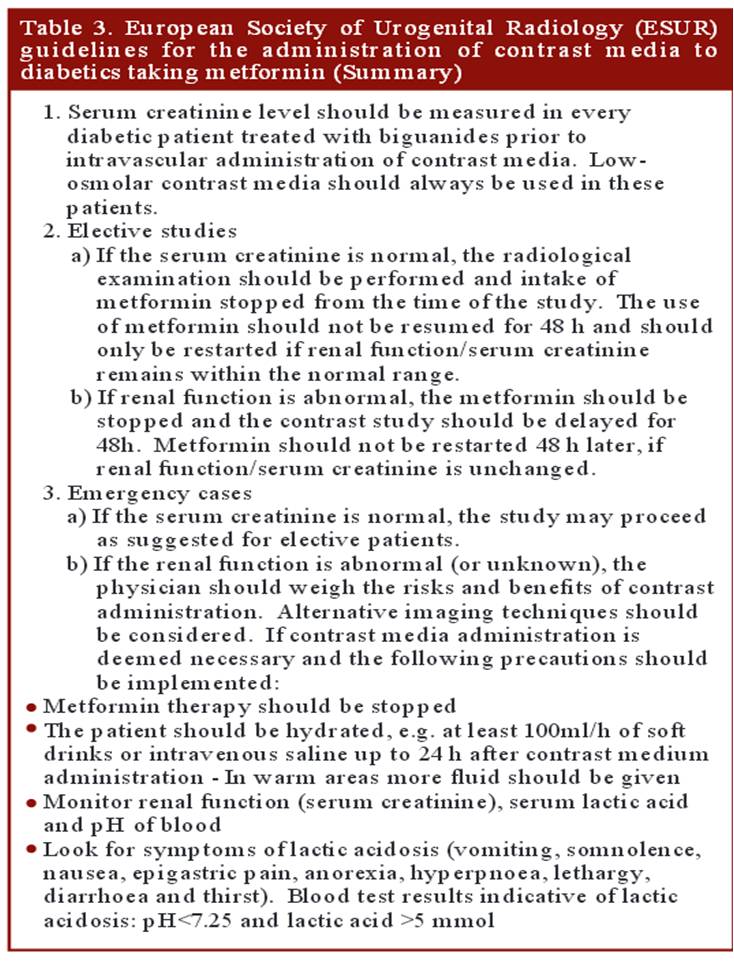
What can be done in emergency situations
- Since the risk of lactic acidosis is very low , in case of emergency situations Metformin need not be discontinued prior to contrast usage.However it need to be stopped for 48 hours from the index procedure. (Fortunately Metformin is a dialysible drug that can be removed in case of toxic accumulation.)
- Consider alternate mode of Imaging if renal function is really concerning
Reference
1.Pre admission metformin use and mortality among intensive care patients with diabetes: a cohort study.Christiansen C, Johansen M, Christensen S, Crit Care. 2013 Sep 9;17(5):R192. doi: 10.1186/cc12886
2. http://ccforum.com/content/pdf/cc12886.pdf
A good article from drug review Contrast induced nephropathy and metformin
Posted in contrast induced nephropathy | Tagged contrast induced nephropathy and metformin usage, eusr guidleines for contrast and metformin, metformin and coronary angiogram, should we stop metformin in all ? | Leave a Comment »
Wall motion defect , in patients after CABG is fairly common.These defects are difficult to interpret as the mechanisms can be multiple.Though the commonest wall motion defect appears to involve the interventricular septum. it can occur anywhere in antero-lateral zone.
The mechanism attributed is the effect of pericardiotomy , which surgeons as we understand leave it open after grafting .This can cause lack of localised ventricular interdependence and results in a a brisk septal movement (bounce )It is an indirect effect .
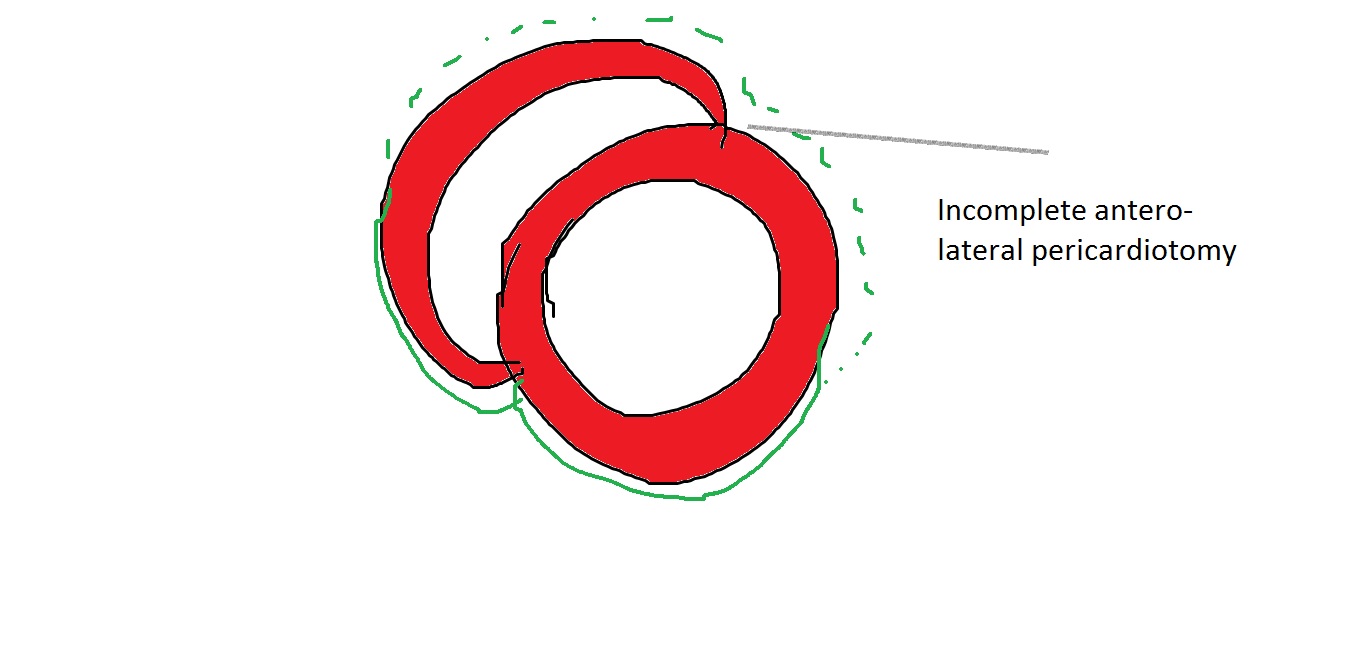
Note the, wall motion defects are confined to the exposed areas of the heart during cardiac surgery .In short axis echocardiography it correlates anywhere between 9 to 3 O clock position. Though interventricular septum is not covered by pericardium in the true sense , there is a indirect bounce effect over IVS due to interference with anterior ventricular interdependence .
More commonly a direct wall motion defect in the 12 to 3 O clock position in short axis is seen .This can closely mimic true wall motion defect as pericardial adhesions can tether these segments. Careful observation is warranted.Myocardial thickening is the key differentiating feature.
What is the physiological impact of these wall motion defects ?
It is generally considered benign (It is !) .Though in echo it looks awkward and suggest desynchrony. The real issue is , it can mislead the echocardiographer to errors in calculation of that universally sacred parameter called EF %
Importance of knowing pre existing wall motion defect.
This has to be reviewed with old reports as it can wrongly create a new wall motion defect de-crediting the surgeons.
New pathological wall motion defect.
Of course it can happen due to peri-operative ischemic insult or infarct . However , It need to emphasised transient wall motion defects are common post CABG due to apparent hypoxia.This seems to be more pronounced with on pump surgeries than off pump .(Expected though) In my opinion, 2-4 weeks cooling off period is required before a meaningful assessment of wall motion post CABG.
Late pericardial reactions and localised constrictive features has been reported.
Disappearance of wall motion defect : How common ?
Any disappearance of WMA is welcome . It happens rarely though . Some of the post ACS population (Both STEMI and UA/NSTEMI) can experience this , as they could harbor zones of myocardial segments afflicted by ischemic stunning rather than true necrosis , that might disappear.
Posted in CABG, Cardiology -unresolved questions, Echocardiography - LV dysfunction | Tagged echocardiography following cabg, paradoxical wall motion defect in ivs septum cabg, post cabg wall motion defect | Leave a Comment »
Inferior STEMI is as common as Anterior STEMI .Unlike the anterior STMI which auto localises to LAD , inferior STEMI has to be fixed either RCA or LCX.
Following ECG features help localize Inferior STEMI .
- ST elevation in lead 3 > lead 2 suggest RCA (Not always true )
- ST depression in lead V1,V2,V3 strongly suggest LCX. (More objectively the sum of ST depression in V1, 2 , 3 divided by sum ST elevation in 2,3, AVF , if less than 1 indicate LCX. Or simply ST depression V3 > Lead 3 indicate LCX.)
- ST depression in lead 1 indicate RCA
- ST elevation in lead V6 strongly suggest LCX
Finally , and most importantly RV infarction as documented by ST elevation in V4R almost always localises the lesion in proximal RCA.
Role of Echo
If ECG features are not clear , a rapid bed side echo has a very good localizing value. To fix RCA look specifically for wall motion defect between “6 to 8” O-clock position .It corresponds to infero basal septum that is invariably supplied by RCA. For LCX involvement concentrate on “3 to 6” o clock position.

Image source and courtesy http://www.aseuniversity.org
Which has better outcome RCA or LCX STEMI ?
- Though RV infarction does not occur with LCX , incidence of MR is more with LCX and can be truly troublesome. This probably negates the potential advantage of “protected RV” in LCX STEMI.
- Since LV lateral free wall involvement is extremely rare with RCA STEMI , it has a lesser impact on LV function while LCX STEMI can give a double blow to LV (MR and LV dysfunction)
- On the down side ,coronary artery spasm and thrombus load are more with RCA .
Interventions in RCA is fairly straightforward ,while acute LCX PCI has some issues . Apart from technicalities of intubating the posteriorly curving LCX ,realistically it involves fishing in troubled waters , as we need to cross the left main , likely physical contacts with LAD ostium , which is the sole supply chain for the injured and ischemic LV myocardium . Meanwhile , If RCA is the culprit , its a well cordoned crime scene where one can spend time liberally and fix the lesion.
Final message
It is easier to localisethe culprit artery in inferior STEMI ,but its a tricky to predict outcome .Both can be troublesome .It depends on dominance of the RCA/LCX ,proximal nature of lesion, the number and caliber of OMs, and PLVs and RV branch .However, it remains a fact LCX STEMI has a overall turbulent course.
Posted in echocardiography, Infrequently asked questions in cardiology (iFAQs) | Tagged echocardiographic segments in lcx vs rca, localising inferior stemi rca vs lcx | Leave a Comment »
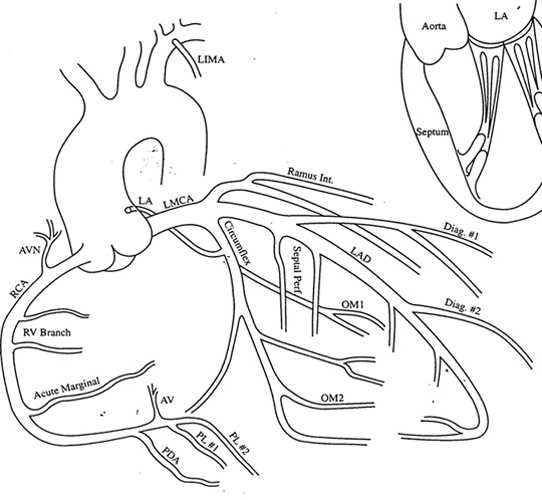
Co-dominant coronary circulation is defined as , when posterior crux of the heart receives twigs from both right and left system making this water shed area with advantage of twin innervation.They essentially supply inferior and posterior aspect of both left and right ventricle including the posterior aspect of interventricular septum.
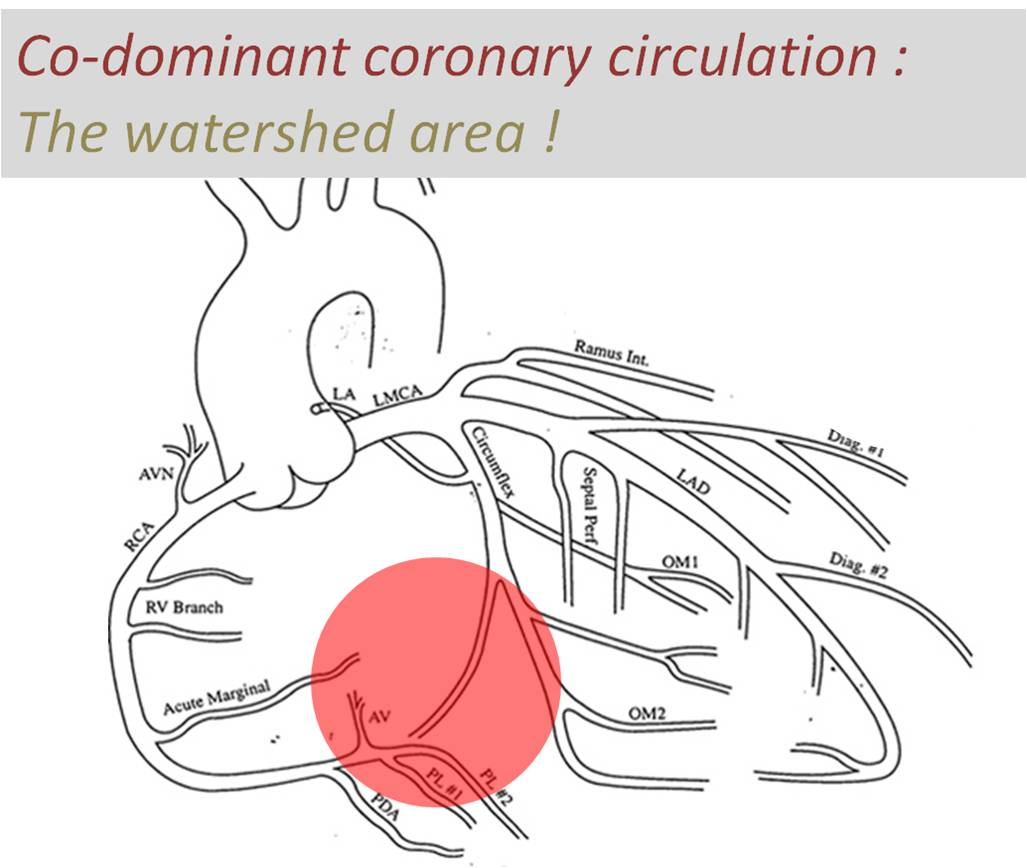
Image courtesy modified from :http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/image4.JPG
Traditionally inferior and basal aspects of heart are perceived (wrong tough !) as less important than anterior surface of heart.Infero posterior MI can be extensive and cause significant LV dysfunction and poor outcome. Longitudinal function (AV grooval velocity) and Mitral valve function is critically dependent on posterior circulation.
Is there an advantage for co-dominant circulation with reference to ischemic mitral regurgitation ?
Obviously ,one would expect there is some advantage in co-dominant circulation when ACS occurs either LCX or RCA.It could theoretically protect against development of MR as posterior papillary muscles could receive supportive twigs from its companion.
However , there is a caveat .The antero-lateral papillary muscle normally has twin blood supply from LAD(Diagonal ) and LCX (OM) . But in co-dominant circulation this pap muscle is at risk of becoming single blood supply as the dominant RCA has a trade off with OM with its large PLV branch. It is likely in co-dominant circulations if LAD is the culprit outcomes are likely to be worse.
Final message
A rare study involving more than 200,000 patients which specifically addressed this issue of dominance and outcome , threw some surprising findings. In concluded PCI outcomes with left or co-dominance has a worse outcome than Right dominant system.
Reference
2.Papillary Muscle Perfusion Pattern A Hypothesis for Ischemic Papillary Muscle DysfunctioPaolo Voci, Federico Bilotta, Quintilio Caretta,Circulation. 1995; 91: 1714-1718
Posted in Uncategorized | Leave a Comment »
Verdict ?
Only complicated or high risk STEMI, would require immediate anatomy based management. Please note, this population at worst is never beyond 20 % of all STEMI. Hence more than majority of patients can be managed effectively without CAG.
My reasoning tells me,though knowing the coronary anatomy appear vital , it is rather the physiological impact of those anatomical lesions that will determine the outcome. So,post STEMI, if at all , we need to investigate, it should be about the adequacy of the over all blood supply to left ventricle.This is done by a pre or post discharge sub maximal stress /nuclear test .If it’s negative with a good exercise tolerance CAG will never be required as any critical flow limiting lesion ( that would require intervention )is excluded with near 100% surety.
Postamble :Try asking any neurologist , how often they demand to know cerebral arterial anatomy for managing stroke ? You will get a real surprise answer !
Posted in Uncategorized | Tagged fibrinolysis vs priamry pci, indications for coronary angiogram following stemi, priamry pci vs thrombolysis, revascularisation for cad, stemi guidelines, stemi management controversy, timing of coroanry angiogram in stemi, when to do coronary angiogram stemi ? | 2 Comments »
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- March 2026 (7)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,637,860 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note


{kind=link}