How can we use AI as a tool of knowledge distillation ?
Here is a deep discussion with Grok 3, on the merits, limitations & validity of DANAMI 2 and PRAGUE 2 , the two old studies on pPCI. Curiously , we don’t have any other studies to quote. As on 2025 , superiority of pPCI hangs precariously on these two decade old studies, which has some serious omissions in the primary end point and its Interpretation. To get into the facts , please go through the following link.
Absolutely yes. The number of studies with such wrong aims is staggeringly higher than we could imagine. “Wrong aim” is probably not the right word to describe them. Rather, we can call them obsolete, duplicate, illogical, unproductive, intentionally fraudulent studies, or studies with a prefixed conclusion.
There is an estimate, that says 95% of papers in nearly 5,000 medical journals, is either junk or written for the sake of publication related to mandatory academic positions or promotions as a budding scholar or faculty. Science has to survive on the shoulders of those rare & genuine 5% souls.
Final message
What is the true “Aim for your study” , I want a very honest answer ?
Yes sir, I agree ,the primary aim is to publish my damn paper and get that promotion !
A related post
There was a brief post about this in the year 2008, 15 years ago. Is it still relevant? Find out for yourself.
“In one sense, meta-analysis would come closer to a milder form of ethical plagiarism”
Can meta-analysis really be called as original scientific research ?
No it is not,but some may say yes. It is very difficult to dispute either. But, the fact of the matter is, meta-analyses are not a true science of innovation. It is using some others’ work( sort of intellectual steal ?) done by a group of scientists interested in the same research topic, trying to squeeze more info from these studies. It is a glorified group journal club activity.
At best, meta-analysis can be referred to as knowledge and evidence aggregation. Surprisingly, mostof the academia seems to give more weight to meta-analysis, disproportionately more than the original researchers. This is because meta-analytic scientists backed by big journals claim, they can bring out more info out of the original. The assumed scientific superiority of meta-analysis is expected to be downgraded soon, as these sort of evidence aggregation can be done easily by any AI-powered engines. Network meta analysis, by dedicated medical scholastic AI networks can do this in a fraction of a second.
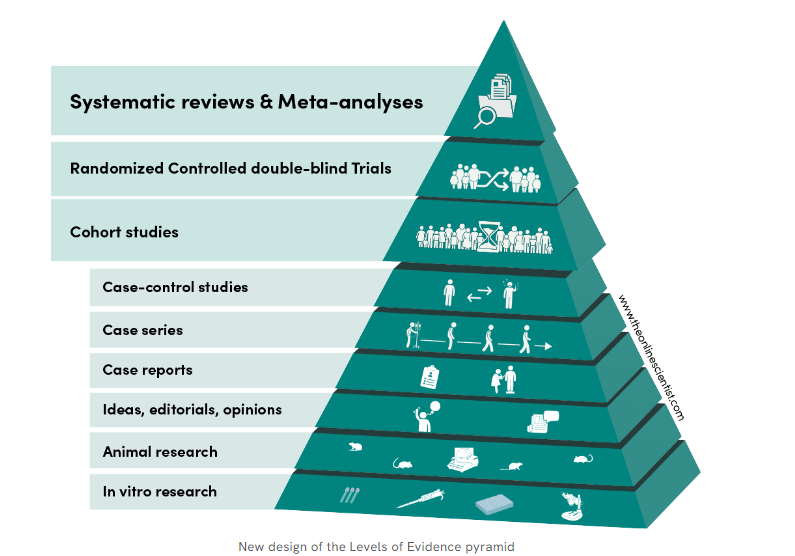
Meta analyses as of now is sitting proudly as crowning glory at the top of evidence pyramid. This is one of the reasons for the false glory surrounding anyone (or anything ) associated with meta-analyses. I doubt whether it really deserve the top slot. (An excellent debate between RCT vs metanalysis) Wish, the meta-analysis taste its own medicine at least once. We need to have a meta-analysis to show it is really superior to other forms of evidence. I cant find one as yet.
What about systematic review ? This looks better, as it has less statistical content , and the researcher is at least compelled to go deep and get enlightened on the topic as they spend months together on the topic.
How is meta analysis different from original research?
There is no new data collection ,no primary hypothesis testing . It primarily focus on summarizing existing evidence. To do it properly, there are certain standards.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)
Cochrane Handbook for Systematic Reviews of Interventions
MOOSE (Meta-analysis of Observational Studies in Epidemiology)
While meta-analyses aren’t original research, it’s a crucial tool for evidence synthesis, research translation informed decision-making.
Flaws of metanalysis
It is a academic business with done studies. So it is 100% retrospective. It might come with irreversible errors. Unless every error in the past studies is accounted for and curated the result of meta-analysis, it can never be foolproof.
Should we get permission from all the authors who did their original studies before doing a meta-analysis?
As long as fair use criteria applies there is no need , but a moral obligation is definitely there . Other wise metanalyses will come closer to a milder form of academic plagiarism of others’ work. (Of course legally and scientifically approved)
Final message
In the world of true scientific research, meta-analyses can not be considered as great scientific work. It is just evidence aggregation, which of course could be meaningful if and only if the studies taken were done properly.
However, meta-analysis has undisputed value in aggregating rare cases, scenarios, diseases, and problems where there are very few published studies. Collecting them together in an organized fashion serves a real good purpose.
A set of attitudes, habits, or possessions associated with a particular person or group. and such attitudes, etc, are regarded as fashionable or desirable.
Final message
Communicable disease need not be an Infectious disease like covid. The word “Communicable” shall soon convey a new meaning, to the enlightened. Adverse life styles ,disseminated into the community that vigorously propagate CVD, has every reason to be referred to as a ‘Neo non-infectious pandemic”
Postamble
In the strict sense, CVD is not a communicable disease ,rather the risk factors are …but technically it is.
Here is a pleasant surprise, a collectors issue of NEJM year book 2023, is made available free (even for non subscribers, in its website) .It is fascinating to know how fast the Internal medicine has grown. For the busy cardiologists, this will a be refreshing reminder, that there are other important organs and specialties do exist in medicine , with equal breakthroughs and Innovations.
It is indeed an amazing , whirlwind tour of medicine for all those who see medical science as single holistic specialty. It has articles, ranging from from simple clinical studies on postpartum hemorrhage (E-MOTIVE study) from deep inside Africa by Melinda Gate foundation, to Dupilumab for COPD, a stunning monoclonal antibody inhibitor of IL-4 for COPD exacerbations. Shortening tuberculosis treatment with a strategy involving initial treatment with an 8-week Bedaquiline-linezolid regimen (TRUNCATE-TB study) is also a revelation.
Of-course, the mandatory cardiac topics do find a prominent place including the currently omnipresent drug GLP agonist Semaglutide for HFpEF (STEP-HFpEF study). Baxdrostat, an Aldosterone synthase antagonist for treatment-resistant Hypertension, appears promising (BrigHTN).
Final message
However, the crowning glory among all articles appear towards the end of the document, titled Combating misinformation as a core Function of Public Health.
Let me share the link to this PDF document here. Hope it allows open access and there are no copyright issues. Notable articles of 2023 from NEJM .
Statins belong to a group of drugs, stolen and reengineered from the blueprint of natural Chinese red yeast rice (Monocoline K) in the late 1980s. The rest is the remarkable history in the pharma industry.
Statins directly interrupt the cholesterol synthesis by blocking HMG-CoA within the hepatocytes. It significantly lowers the LDL, fights human vascular atherosclerosis. It makes the plaque either regress, prevent progress, make it harder and in the process make them less vulnerable . There are innumerable studies that document the evidence. Statin has become a must-prescribe drug in any one with clinically established CAD or even in concealed CAD. Guidelines are available to prescribe statins various intensity, depending on the risk profile.
Which statin ?
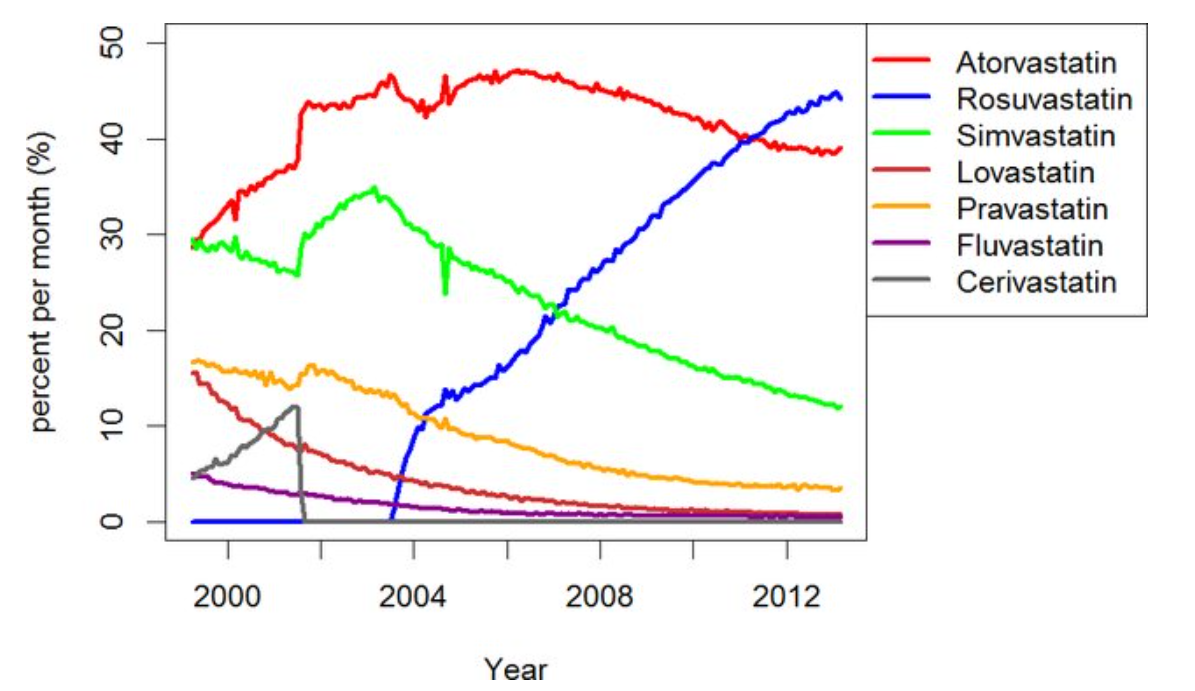
There has been a long list of statins. Many of them have retired from the ring .Currently, the fight is between Atorvastatin, a Rosuvastatin. Like Pepsi vs. Coke.
Note the graphic ,A meteoric rise of one drug since 2005 . (Can you guess the reason ?)
ATRORVA or ROSUVAWhich one should I choose ?
There is very little “one to one” comparison study between Rosuvastatin and Atorvastatin .The gap in the pros and cons are narrow. Following points are observed, without much dispute.
No one is dare enough to give strong verdict . Surprised to find one this month. BMJ has come out with a possible answer. It is called LODESTAR trial (Ref 1)
Mechanism of new onset diabetes with statins (REF 3)
It can be 7% with Rosuvastatin (less with Atorvastatin). We think, statins act primarily within the hepatocytes where cholesterol synthesis takes place, but they also have an eye on the pancreatic β-cells as well. It down-regulates GLUT-4 in adipocytes, and results in compromised insulin signalling. Furthermore, statins’ impact on epigenetics may also contribute to statin-induced T2DM via differential expression of microRNAs.
Mechanism of cataract with statins (Ref 2)
The cells lining that line the lens are dynamic and require cholesterol on a day-to-day basis. Statins inhibit proper epithelial cell development within the crystalline lens, where cholesterol biosynthesis is critical to maintain transparency and structure of the lens.
Final message
So, is it Atorvastatin or Rosuvastatin? It is left to you.
Mind you, “no statin at all” is the best option if circumstances and risk profile allows. Statins are never considered life-saving staple drugs in our fight with CAD and atherosclerosis. We, along with our scientists might may make you feel like that. Lipids can be controlled within desirable means exclusively with diet and exercise in most of the population* .
(*Forget about statins in the last 5000 years of known human existence, so many great people have lived a long and successful life in this world, without even knowing there is an organ called the heart that is responsible for the circulatory system)
World heart day is being celebrated every year on September 29th ,Initiated by the World heart federation with a genuine purpose, vision & goal. It has become big hit in recent times. In India, the theme has captured the imagination of the main stream media . Every one wants to propogate a message. I am not an exception. Please bear with this skewed message “One for the patients and the other for the self” !
This quote is being sent for the annual meet of “Right care movement” I know ,this can sound outrageous, permissble limits of abuse ? Up to 2% or 5% ? Let it be anything . Meanwhile try to enlighten yourself , the key differences between misuse & abuse.
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.