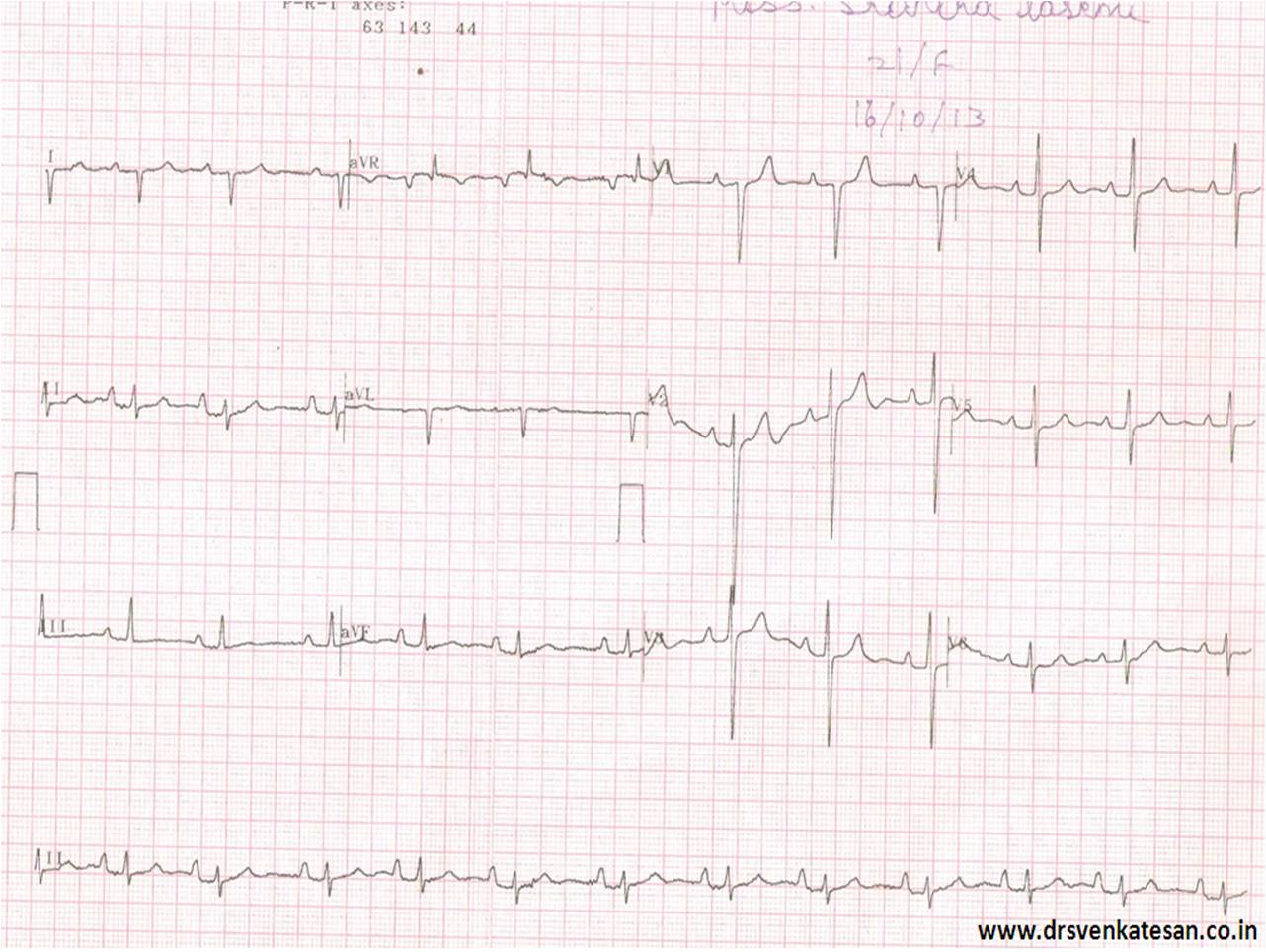
In one of my classes , this ECG was presented . Controversy erupted.It was about the basics .
What is the QRS axis of this ECG ?
Not surprisingly there were handful of answers .
- North west Axis
- Indeterminate QRS
- +150
- +180
- 0 degrees
- Extreme Right axis
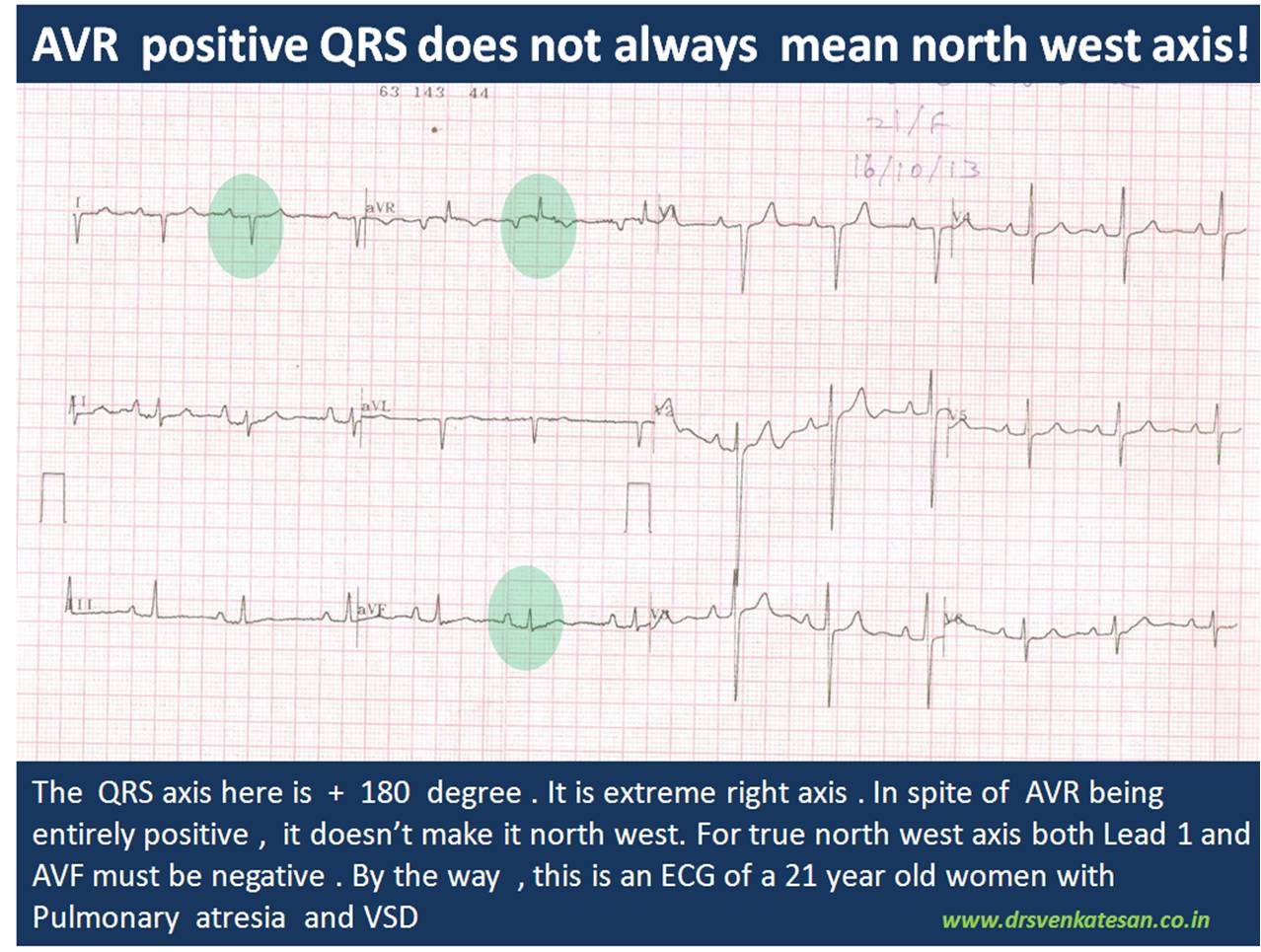
Which is correct ? My guess is , it should be closer to + 180 . Lead 2 is equiphasic and perpendicular lead is negative limb of AVL ie + 150 .If you plot Lead 1 and AVF in graph and calculate we get + 135 . (In the strict sense , we are not supposed to take one standard lead and an augmented lead for plotting ). Finally, the strongest argument was , since AVR shows only positive forces it would make north west axis more likely .
Causes of North west QRS axis
- Denova North west axis
- Extreme Left becoming NWA*
- Extreme Right becoming NWA
*Left becoming NWA is much more common than other types.
Chamber enlargement alone is not sufficient to shift the axis to NW corridor. There must be anatomical distortion of his bundle and it’s branches to shift the axis dramatically .This usually occur in complex congenital heart disease. In acquired heart disease the an apical VT is probably an important cause for NWA.
One word about indeterminate qrs axis .
By the way , Indeterminate QRS axis is not synonymous with north west axis. This term should ideally be used if qrs complex is equiphasic in all limb leads , when qrs axis can not be truly determined .This situation commonly occurs when we encounter very very low voltage qrs as in cardiac tamponade and severe hypothyroidism , constrictive pericardits, etc
If the QRS is in north west corrodor , How to differentiate , whether it came from extreme left axis or right axis ?
I am yet to find a correct answer for this.
- Pre-cardial pattern will help.
- A q in V5/V6 would suggest extreme left axis.
- May be we have to look the initial qrs vector in AVR lead for more clues
Traditionally , we talk about net qrs axis . We should realise net qrs axis is a combination of initial and late vectors .It can be dramatically different in different leads . QRS axis is a two dimensional representation of three or more (omni) dimensional electrical forces .That is the source for confusion. So, do not unduly worry about the complexity .Blame it on the limitations of surface ECG !
Expecting some comments .