Background
A 52-year-old diabetic woman who had undergone recent PCI with a DES developed a febrile illness which was diagnosed as Dengue fever. She has been taking DAPT (Dual antiplatelet) meticulously to maintain her stent. Now, her platelet count has dropped from 1.5 and subsequently to 1 lakh. She is asking now, whether to stop DAPT or not? What is the risk of stent occlusion if she stops?
The D³ cube syndrome
Infectious diseases rarely bother a cardiologist (maybe a few IE, myocarditis, etc). Now, a unique situation is emerging.
*Dengue affects 50-100 million people worldwide every year and one billion are at risk. CAD affects 5 % of the population that amounts to 350 million. As we fight CAD, 2 million coronary stents are implanted annually and at least one-third of them may be on DAPT at any time.
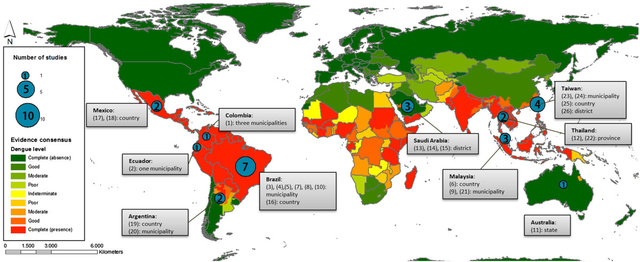
When a global population is at risk of an infection that targets human platelets and another chunk of the same population in whom platelets are targeted with drugs, what is the Incident risk of overlap between these two groups?
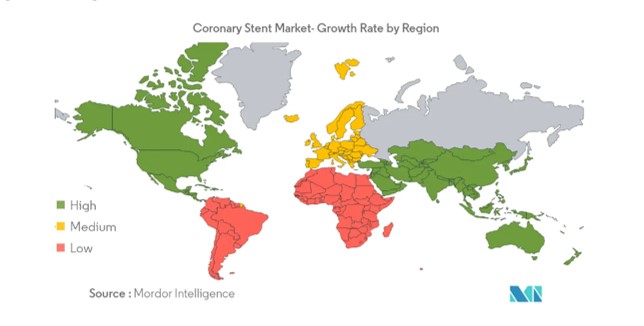
If you look at these two maps, I think we will not hesitate to call both Dengue and DES a global epidemic affecting the platelet function. The top one depicts the world stent market and the bottom Dengue prone countries
Mechanism of thrombocytopenia in dengue
The mechanism of thrombocytopenia in dengue is not clear. Both production at the marrow level and destruction in the periphery is attributed. The antibody-mediated NS (nonstructural protein) is the original antigenic sin (Click to know more)
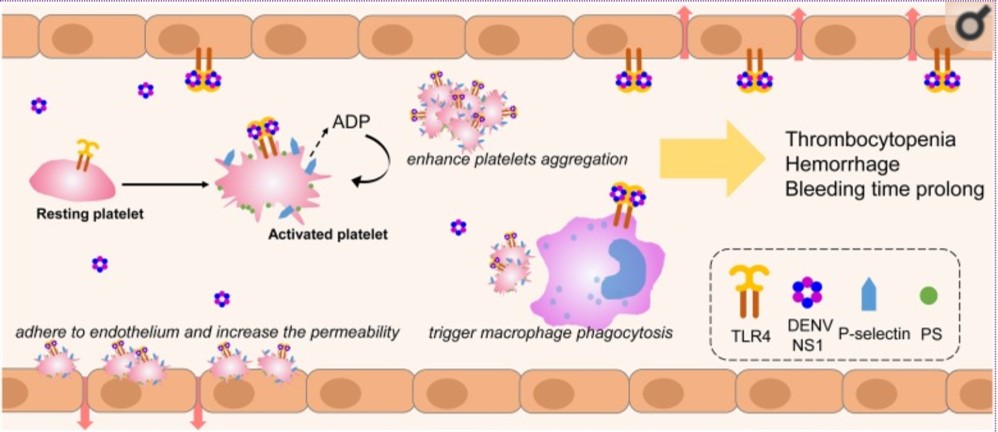
Chiao-Hsuan Chao PLoS Pathog. 2019 Apr; 15(4): e1007625. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6497319/
Meanwhile, DAPT paralyzes the platelet by blocking P2Y12 and COX. It is obvious Dengue virus amplifies the antiplatelet action and increases the bleeding risk at any point during the illness.M
Risky period
Bleeding periods is highly unpredictable. The late recovery phase seems to be critical for hemorrhagic risk.it can go up to 2 to 3 weeks or even a month. (When we don’t have data, only experience becomes data. )
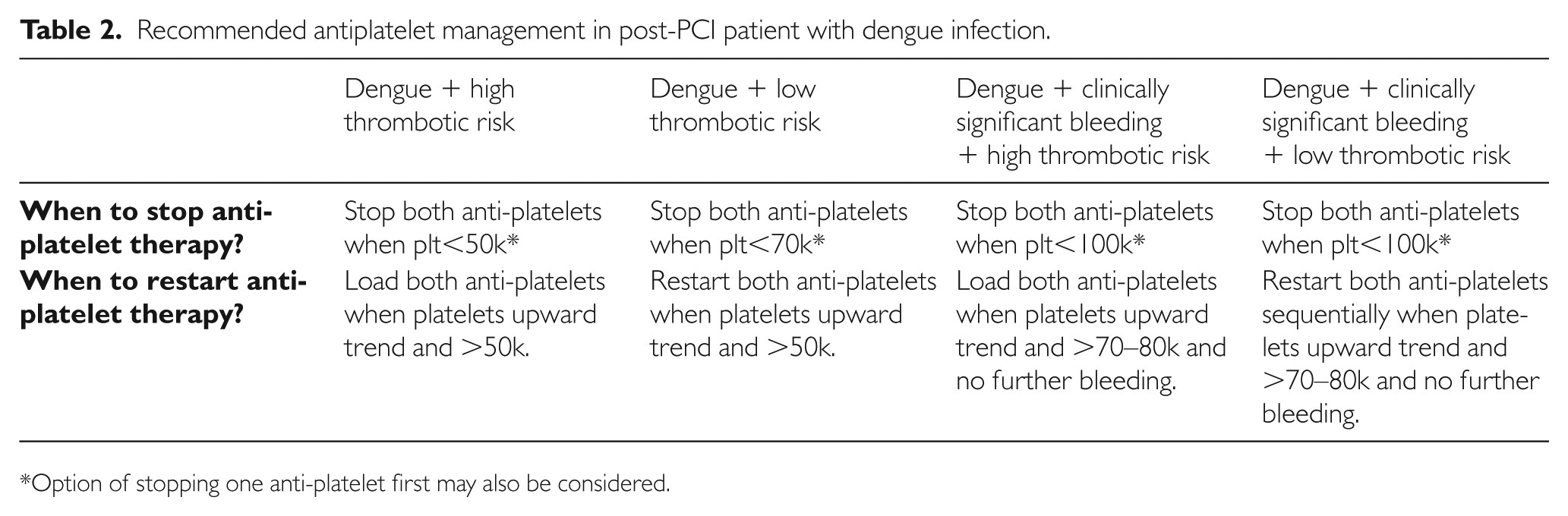
How to manage Antiplatelet agents in post PCI patients with dengue?
While we have guidelines to stop DAPT during the need for emergency surgeries, the same can not be adopted in Dengue.(Curiously, we can stop DAPT without much fear, after all, dengue antigenic responses take up the role of antiplatelet agent )
Presario from Brasil proposed a practical suggestion.Pesaro AE (Dengue: cardiac manifestations and implications in antithrombotic treatment. Arq Bras Cardiol. 2007 Aug;89(2):e12-5)
Switching to other drugs like eptifibatide or NSAIDs is not an option.
Post dengue prolonged platelet dysfunction
Though the platelet count returns to normal soon after recovery, long-term platelet defects are also reported. This has implications in resumption of DAPT. Surprisingly, dengue recovery phase thrombocytosis also happens for some unknown reason. Ref: Rebound thrombocytosis causing MI following dengue fever? (Roy A, et al Indian Heart J. 2007 Jan-Feb;59(1):94)
Final message
When both Dengue & post PCI epidemics are trying to match in numbers, I guess D³ syndrome (Dengue-DES-DAPT) would soon become a significant clinical issue.
Now going back to the title question, Should I stop DAPT or not?
- Never easy to answer this question. It is a fine balance between the risk of bleeding vs the risk of stent thrombosis.No amount of algorithm and guideline may clarify it.
- On any given day, the risk of bleeding in vital spots is more dangerous than thrombus.
- It is wise to withhold antiplatelet drugs in all febrile illnesses when the platelet count is actively falling below 1 lakh. It may not be quixotic thinking to expect dengue viremia to help the DES with its DAPT equivalent action ! in the intervening period.
Reference
2.Wishnu Aditya et all Proceedings of Singapore Healthcare 2019
Further queries
What about Heparin, Oral anticoagulation (OAC), usage in suspected Dengue?
Go back to basics. Heparin and OAC don’t affect platelet function. It is 100 % safe to continue.
Really? do you think so? No, coagulation physiology is not that simple. Thrombin and antithrombin interactions happen right on the platelet surface. Any antithrombin drugs do have some antiplatelet action as well. Extreme caution is required again. Withhold them unless absolutely indicated.