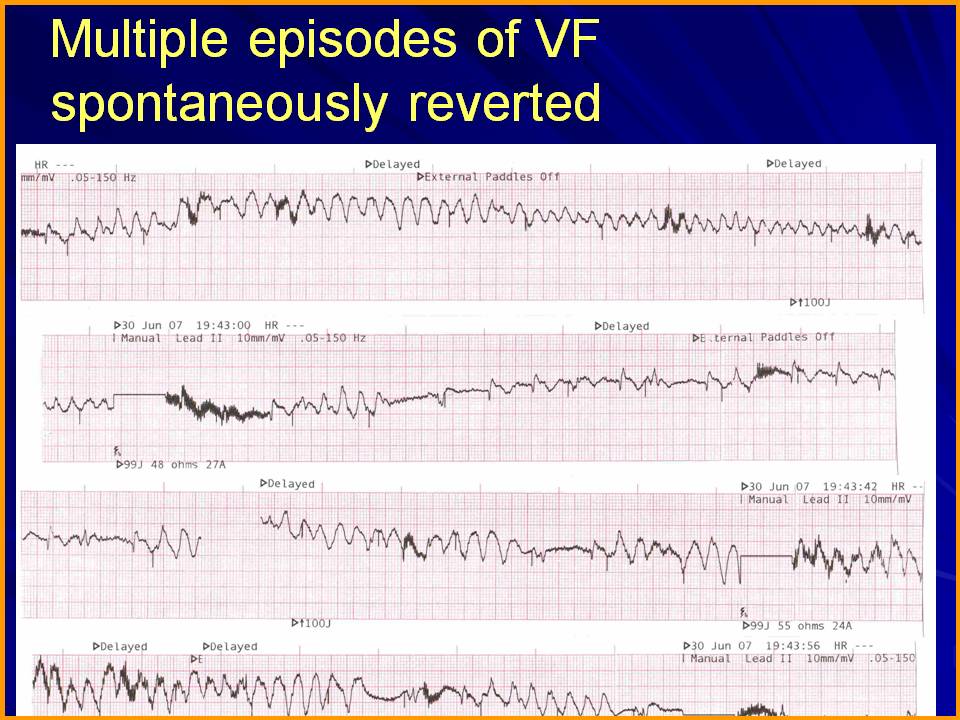
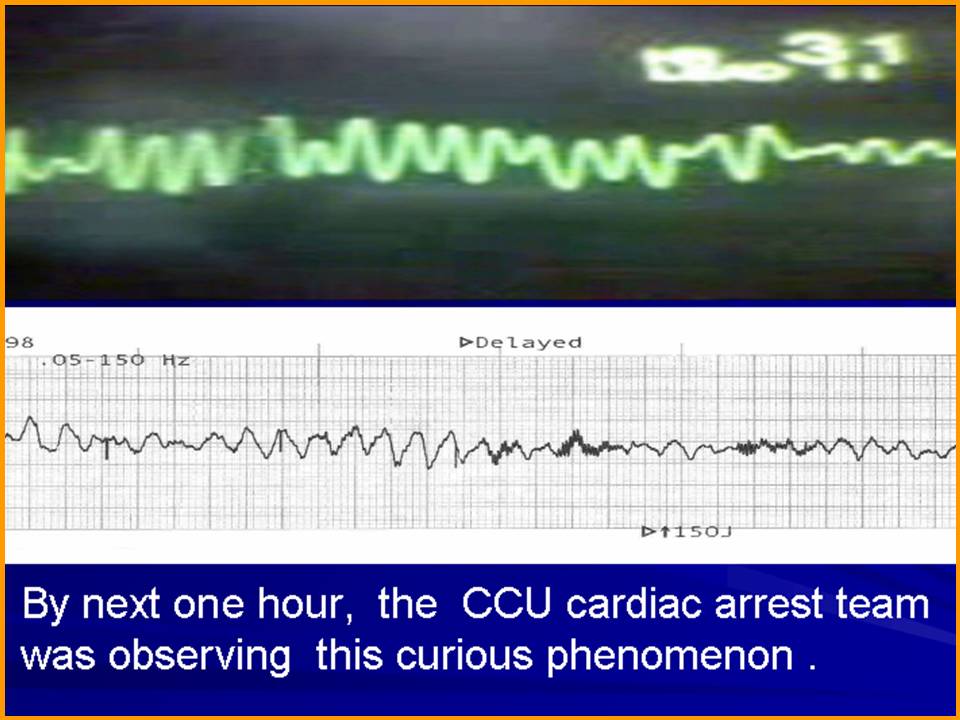
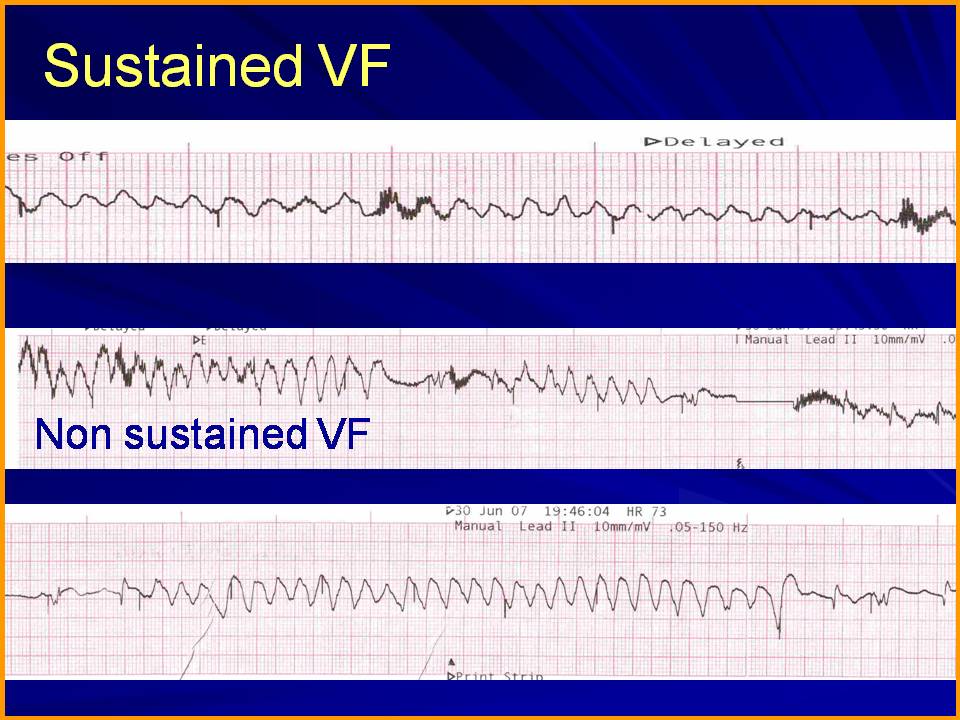
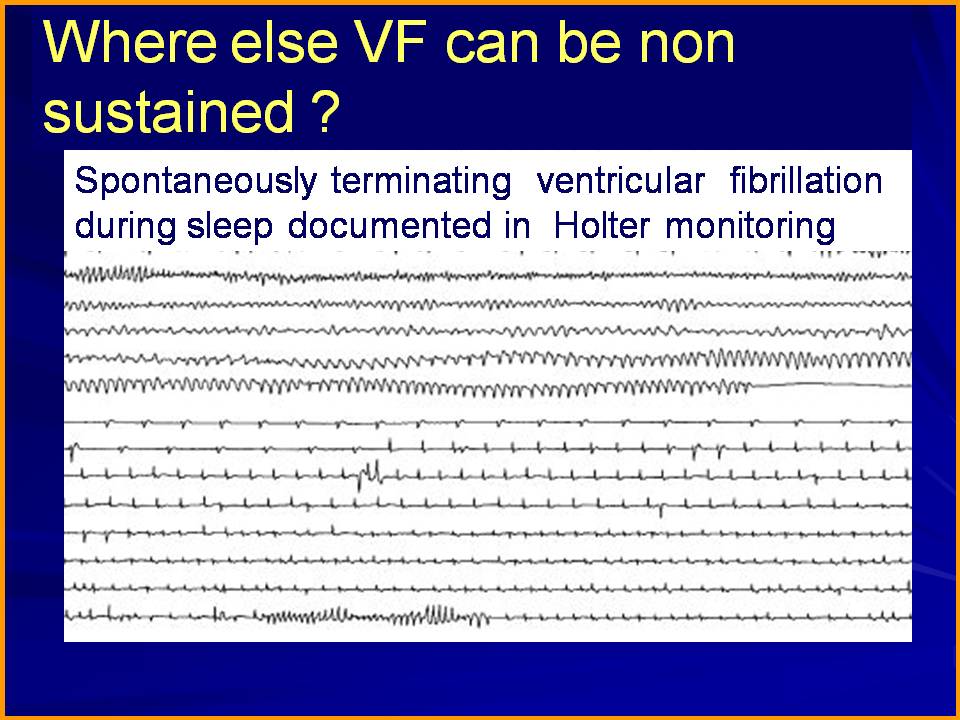
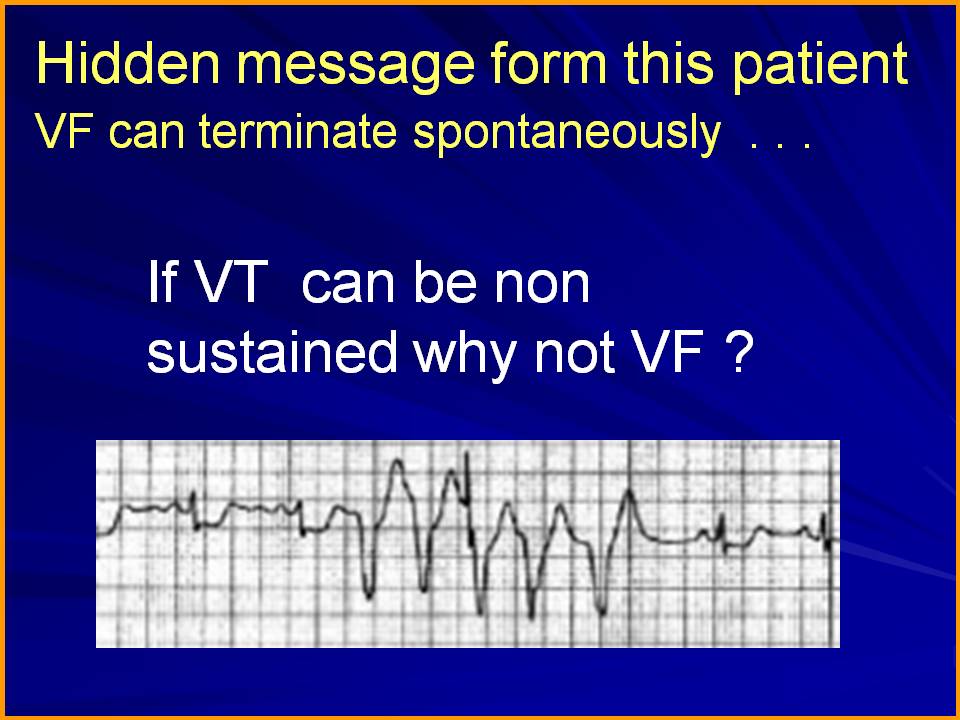
Can VF be a non sustained arrhythmia ? This question was raised and a single case report was presented
in the annual scientific sessions of Cardiological society of India Meet in year 2008 in Chennai.
I am just reposting it from my archives .

Posted in cardaic physiology, cardiac physiology, Cardiology - Electrophysiology -Pacemaker, Cardiology -unresolved questions, My presentations, tagged mechansim of ventricular fibrillation, non sustained ventricular fibrillation on March 28, 2013| Leave a Comment »
Can VF be a non sustained arrhythmia ? This question was raised and a single case report was presented
in the annual scientific sessions of Cardiological society of India Meet in year 2008 in Chennai.
I am just reposting it from my archives .
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, tagged abberrant conduction in apd jpd, apd, apd jpd vpd, escape caputre escape ectopic trigeminy, group beating ectopics, jpd, pause dependent vpds, premature ventricular beat, sinus arrrest and jpd vpd, sinus node dysfunction snd with escape and ectopic rhythm, VPD on February 28, 2013| Leave a Comment »
Sinus node is the electrical high command of our heart .When it gets injured seriously (or shot down as in sinus arrest ) there is utter chaos in the lower ranks !
This is what happened in this patient .
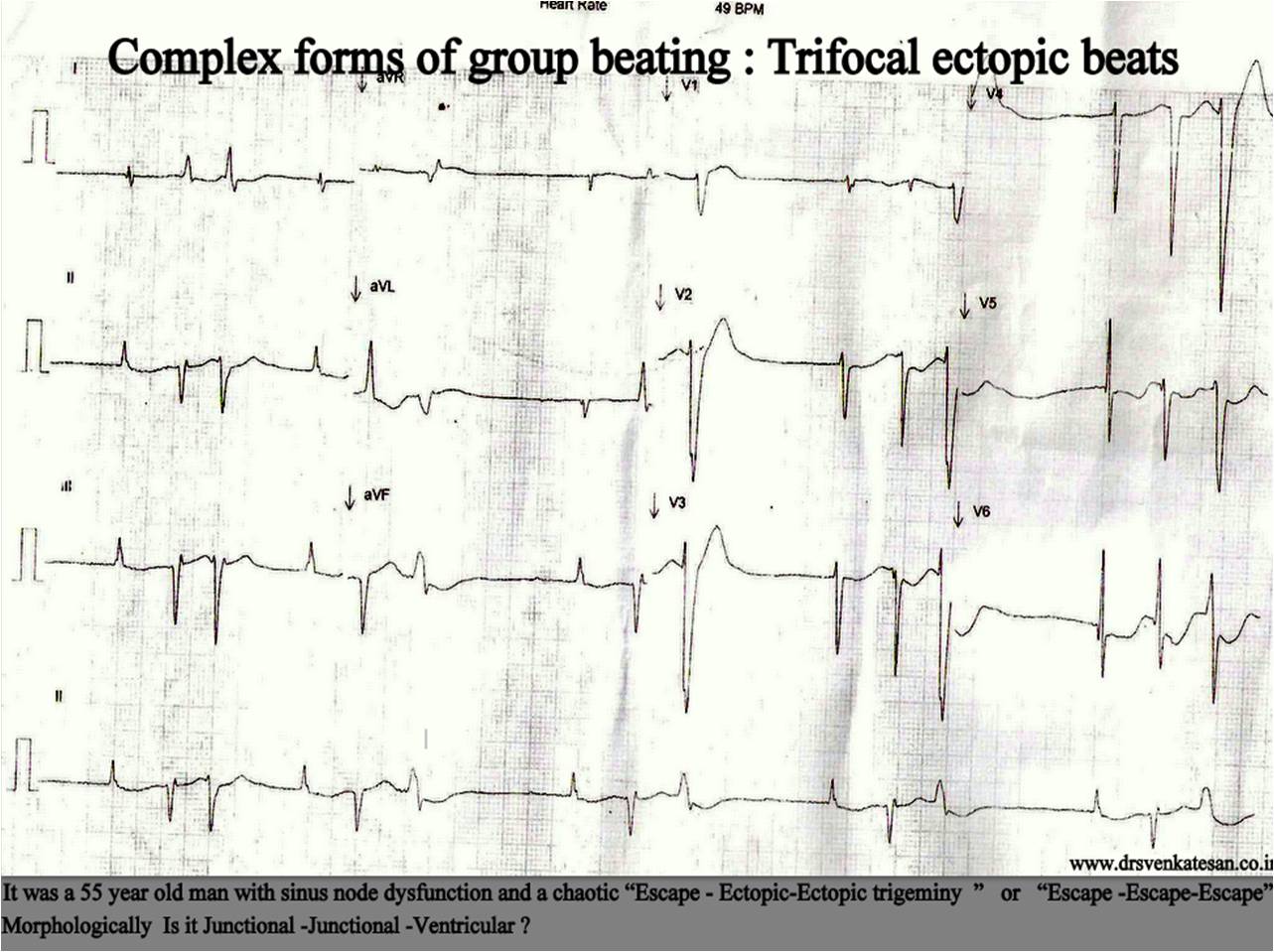
The lower pacemkers can either passively release themselves as escape rhythm or actively fire with a ectopic focus . Any combination of escape / ectopic beats can occur .If occasional sinus beats capture the ventricles things can become further complicated .
It is obvious , this random intra-cardiac shooting makes the life of the myocardium miserable . It is a perfect setting for syncope, tachcyardic cardio myopathy , extreme brady induced VT , VF even SCD.
*Meanwhile , It is heartening to note SND rarely lead to sudden death in spite of all the chaos .However extreme bradycardias that occur in complete heart block does not enjoy this immunity as fatal complications are common if not intervened .
Posted in Cardiology -guidelines, Cardiology -Interventional -PCI, cardiology-ethics, Uncategorized, tagged acts of commision is also a medical negligence, cardiology ethics, hippocrates, inappropriate medical care, medical ethics, medical negligence on February 28, 2013| Leave a Comment »
The irony of modern medical care is 9/10 times medical negligence is defined in terms of acts of omission in required level of care . In reality most medical negligence acts are related to knowingly overdoing a futile diagnostic or therapeutic modality.
This irony was never understood by the public, the professionals or even the judiciary .This remains the most dangerous issue facing modern medicine !
Finally some light is appearing in the horizon . A Missouri Cardiologist is suspended for overdoing things he knows best . . . namely coronary stenting !
This may bring chills over many cardiologist’s spine .
Posted in stroke, Uncategorized, tagged Antipaltelet agents drugs controversy, antipaltelt agents mainstay in tia, prasugrel for tia, prasugrel vs clopidogrel in TIA, strke in evolution on February 27, 2013| Leave a Comment »
Current prescribing information cautions clearly Prasugrel should not be used in TIA or recent stroke (Even in ischemic strokes -Embolic included !)
The warning is perplexing and illogical to me.
What is your take ?
I would imagine the following could be the reasons.
Prasugrel as an antiplatlet agent is many fold powerful and could convert all strokes into hemorrhagic one .
Does Prasugrel convert a TIA into stroke instead of curing it ?
Prasugrel may worsen the stroke in case the TIA is going to end up as stroke.
Is there any thing called hemorrhagic TIA ?
Since we do not have any mechanism to diagnose Ischemic TIA from hemorrhagic TIA , it is better to avoid Prasugrel . It is still a mystery , why clopidogrel which acts on the same receptor and can be safely given for TIA ( pro actively)
After thought
I think Neuro physicians must answer this question . ( Cardiologists better limit their extended geographical terrain ! )
Posted in cardaic physiology, cardiac physiology, Cardiology - Electrophysiology -Pacemaker, cardiology -Therapeutics, Cardiology -unresolved questions, tagged atrial synchrony, atrio ventricular synchrony, cardaic resynchrony, CRT, davi ctop pacemaker trials, inter atrial block, inter ventricular asynchrony, inter ventricular dysssynchrony, inter ventricular synchrony, intra atrial block, intra atrial dyssynchrony, intraventricular dyssynchrony, lbbb and pardoxical septal motion, miracle trial, non physiological pacing, patholgical pacemakers pacing, permanet pacemaker physiology, physiological pacing, resynchronisation therapy, septum vs lv free wall de synchrony, ventricular synchrony asynchrony, vv synchrony vs av synchrony, vvir dddr vdd pacing on February 10, 2013| Leave a Comment »
Answer
Each of the above can be important in diseased heart .The most important component seems to be Inter- ventricular synchrony .This is closely followed by AV synchrony .In dysfunctional ventricles Intra-ventricular synchrony also becomes important .In structurally normal hearts none seems to be important (This statement can be debated )
VVI pacemakers causes both AV and Inter-ventricular (VV ) dys-synchrony
DDD pacemaker may still induce Inter-ventricular ( VV ) dys-synchrony whenever RV is paced for any reason .This may happen up to 60 % of pace making time in real world.
Some more facts
*Chronic VVI pacing may induce adverse remodeling of both atria and may worsen LV dilatation. In contrast isolated chronic organic LBBB is well tolerated and with paradoxical septal motion rarely worsen the LV function.
**Please note the paradoxical septal motion , which is noted in all LBBBs is same as inter-ventricular dyssynchrony .
***Inter atrial synchrony is a less discussed issue .It becomes important in diseased atria which manifest gross intra atrial conduction blocks , atrial inhomogeneity and AF .Onset and offset of AF has a major impact in the way DDD pacing is going to fire .
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Infrequently asked questions in cardiology (iFAQs), tagged inter atrial block, inter nodal pathway, lae in ecg, lae vs inter atrial block, left atrial enlargement in ecg on February 8, 2013| Leave a Comment »
This is an ECG of a 42 year old man .He was reported as Left atrial enlargement (LAE) and was referred for echocardiography . His echo was normal . LA measured 2.5 X 3.1 cm .The consultant called back the echo lab , to verify the left atrial dimension .He thought he was very sure of LAE .It took considerable time to convince him about the credibility of the echocardiographer . He was right after all . . . still . . . ECG was also looked convincing for LAE !
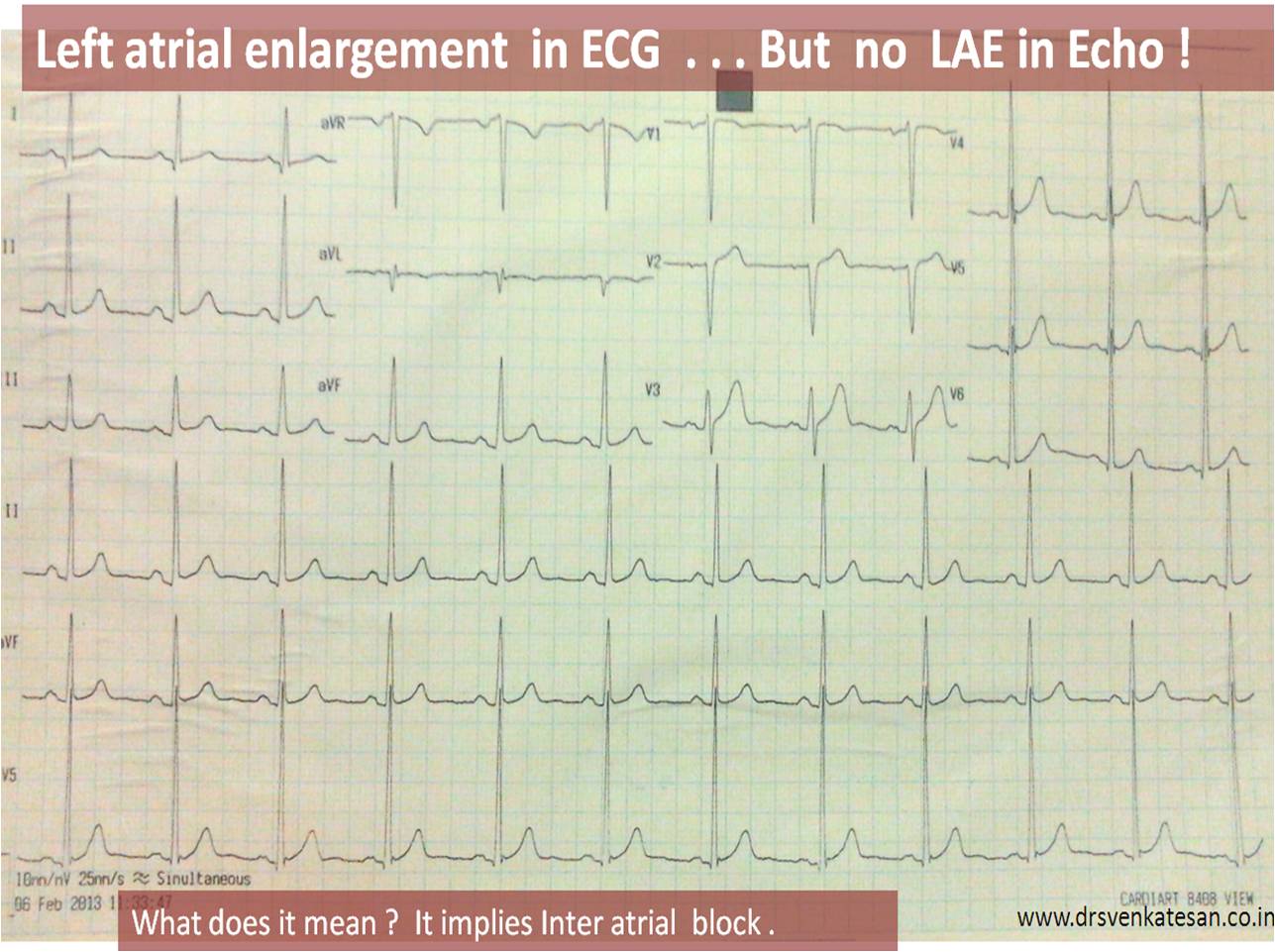

Is this phenomenon of wide P wave with normal atrial dimension common ?
Yes it is . It underscores poor sensitivity of ECG in the diagnosis of LAE .The P wave abnormality in the above patient is due to Inter atrial block (IAB ) . This widens the p wave .
What are the types of Inter atrial block ?

P wave widening is not synonymous with LAE .(Here P waves widened due to sluggish inter nodal pathway and inter atrial pathway .It is something like QRS widening in bundle branch blocks )
Final message
IAB is an important differential diagnosis for LAE . The significance of which is not entirely clear . It is possible IAB precede LA enlargement .It can even trigger AF due to inhomogeneity.
Even though IAB was reported in 1950s (Puech P* ) , it was rarely considered important With increasing incidence of atrial arrhythmia in aging population , IAB is expected to come into the lime- light again . The sophisticated electro anatomical mapping can unravel the mysteries surrounding this entity .
Reference

*Puech P. L’activite´ electrique auriculaire normale et pathologuique. Paris: Masson, 1956; 206.
http://www.jecgonline.com/article/S0022-0736%2812%2900227-0/abstract
Posted in echocardiography, Uncategorized, tagged definition of LVH, LVH with normal IVs on January 31, 2013| Leave a Comment »
We always look at the thickness of Inter ventricular septum for LVH . The Normal IVS thickness is up to 11 mm in diastole . LVH is definite if IVS measure > 11 mm .It is certain if it is > 12mm . But , we need to realise LVH by definition is not simply wall thickness .
It is increased LV mass .
LV mass can increase without wall thickening . This is referred to eccentric LVH . For example in chronic volume overload states (or even DCMs ) LV mass may increase without septal thickneing .
Final message
LVH is possible without IVS thickening .
Posted in Cardiology -guidelines, cardiology -Therapeutics, STEMI-Primary PCI, Tutorial in clinical cardiology, Uncategorized, tagged 2013 STEMI AHA ACC Guidelines, Current stemi guidelines, New stemi guidelines 2013 on January 28, 2013| Leave a Comment »
Guidelines are meant for simplifying cardiologist’s life as well as ameliorating patient suffering . It should also ensure improving overall outcome with efficient use of human resources and economy .
These guidelines are written from sophisticated centers mainly for consumption in developed countries .Though core concepts will be same , many recommendations are neither possible nor desirable at the exact point of delivery in less developed countries . Please remember these guidelines are not binding on you .Physician discretion is the ultimate principle in medicine.
So , let us read these guidelines apply our mind and try to indigenise . Get maximum out of it for the respective population .
Some of the highlights in this 2013 guidelines
1. Therapeutic hypothermia should be started as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest caused by ventricular fibrillation or pulseless ventricular tachycardia, including patients who undergo primary PCI.31–33
(Level of Evidence: B)
2 . Presumed or New onset LBBB is no longer a Indication for emergency reperfusion
3 . Indication of Primary PCI has the following modification

Reference
http://circ.ahajournals.org/content/early/2012/12/17/CIR.0b013e3182742cf6.full.pdf+html
Posted in Uncategorized, tagged coronary artery swing, digital subtraction angiography for coronary motion movement, lad inter ventricular groove movement, lcx legt av groove motion, longitudinal rv function, lv rv function assessment in cath lab, mapse, reading coronary angiogram, right av groove, rv ejection fraction, rv function assessment simple tool, tapse and coroanry av groove rca motion on January 27, 2013| Leave a Comment »
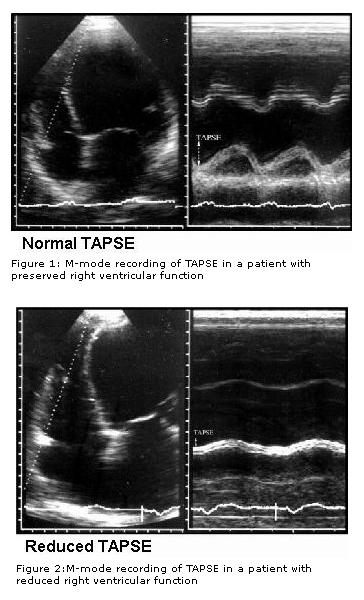
Right ventricular function assessment has always been difficult in view of it complex shape and limited imaging planes in echocardiography .
Recently , we learnt tricuspid annular motion can give a quick assessment of RV function . This was accomplished by M-mode echo of tricuspid annulus. (TAPSE) tricuspid annular plane systolic excursion . This simple parameter has brought the maligned M mode echocardiography into limelight again.
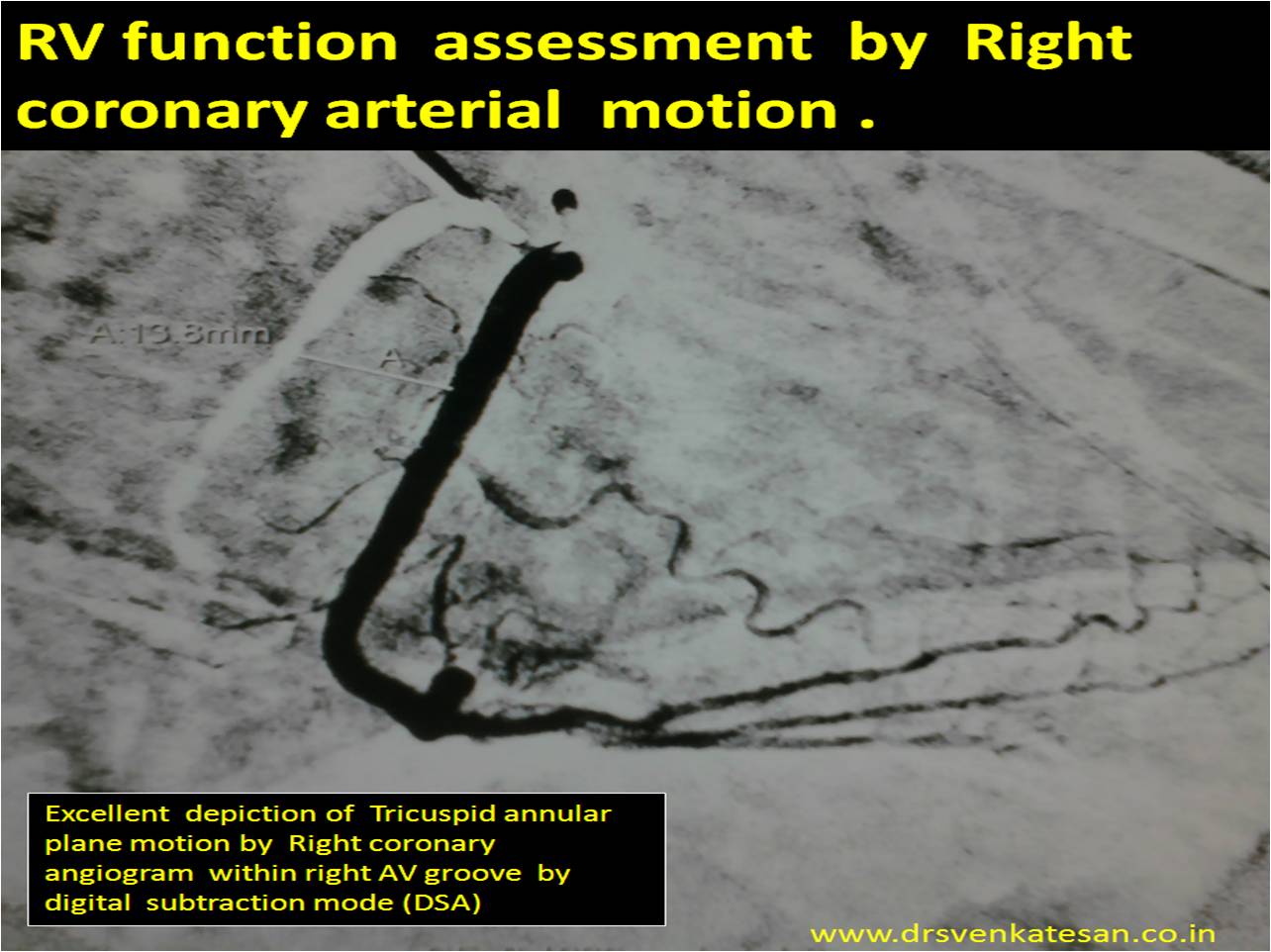
Currently coronary angiogram is done just like a non invasive echocardiogram across the nooks and corners of any country
Modern day cardiologist is expected to look beyond the coronary artery narrowing when reading coronary angiogram. If only we give little importance to how the coronary artery moves with reference to cardiac cycle we can get excellent information about mechanical properties of heart.
Every cath-lab work station has a DSA mode . With this one can measure the coronary artery swing and document it objectively .Right coronary artery swing faithfully reflect RV longitudinal function . This motion is more accurate than the TAPSE by echo . We have found the normal excursion to be 15-20mm (Slightly lower than TAPSE) . Similarly LCX motion give us an estimate of longitudinal LV function and LAD motion can tell us how IVS moves .
Final message
Coronary artery swing* is a new method ( rapid and accurate) to assess cardiac function in cath lab ! We should utilise this more often .I feel it may throw more valuable than the sophisticated but complex 3D reconstructed and post proceed imaging modalities to assess individual chamber function .
* There is no published reference available for modality .It is so simple concept i think , it does not require any major experiments for a proof !
Reference
RV function assessment ASE guidelines
http://www.echobasics.de/rv-en.html
Normal RV function Indices .
TAPSE (tricuspid annular plane systolic excursion) < 2 cm
TASV (tricuspid annular systolic velocity)< 15 cm/s
Tei-Index (myocardial performance index)> 0,50
TAPSE can be correlated with coronary swing
Further research potential
Now we require comparing the TAPSE with the quantum of RCA swing by angiography. I have asked my fellows to look into this aspect . I guess TAPSE by Echo over-estimates the true motion ( normal 2 cm ) seems on higher side. It includes translational motion of echo which is eliminated in angiographic annular movement .
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Uncategorized, tagged refractory rv shock, RVMI on January 27, 2013| 1 Comment »
Right ventricular infarction (RVMI ) is a common cardiac emergency in coronary care units. It can be termed as a mechanical complication of infero-posterior STEMI .However , around 10 % of anterior MI do develop this complication . Onset of refractory hypo-tension in spite of correcting hypovolemia suggests RVMI.RVMI generally comes under class 3 (Cidar Siani /Diamond -Forester classification of STEMI ) , ie silent lung with systemic hypotension. (RV shock requires an unique definition , as it can not be included in traditional definition of cardiogenic shock as the PCWP is likely to be normal.
How to manage a full blown RVMI who is not showing signs of improvement ?
Following is an extract from our coronary care unit experience
(do not ask for evidence for everything !)
Final message
RV shock carries a dismal outcome , almost reaching as that of an LV cardiogenic shock. Ironically ,the most important prognosticator in RVMI is the quantum of LV involvement !