Reporting a coronary angiogram may look like child’s play for most cardiologists. Many do it in less than a minute. (It goes something like this 90 % LAD , 30 % ostial OM1, 50 % mid RCA etc etc ) The famous and meticulous classification of Ellis and Ambrose proposed two decades ago appear largely redundant.
In this review we shall briefly debate an eccentric plaque or lesion .
Pathological definition
Pathologically an eccentric lesion will have a disease free arc within an atherosclerotic lesion.If we apply this criteria most of the plaques appear to be eccentric.
Angiographic definition
In simple terms eccentricity is said to be present when the plaque volume is three times more on one side when compared to opposite side .
The incidence of eccentric lesion is largely under estimated. It can be up to 40 % of all lesions.
It has histological as well as hemodynamic significance.
How to measure eccentricity index ?
Ratio between maximum plaque thickness and minimum plaque thickness (Including the media )

Image courtesy modified from Circulation. 1996;93:924-931
In the above figure : The eccentricity index is measured as the ratio of the maximum to minimum plaque plus media thicknesses. In the eccentric lesion the maximum wall thickness measures 2.6 mm, minimum wall thickness measures 0.2 mm, and eccentricity index is calculated to be 5.2. In the concentric lesion the maximum wall thickness measures 2.2 mm, minimum wall thickness measures 1.6 mm, and eccentricity index is calculated to be 1.4.
What are the associations of eccentric plaque ?
Calcification and hard plaques are more common in eccentrically placed plaques.The most vulnerable point for plaque rupture or disruption is the shoulder region between normal and plaque segment.

A long eccentric lesion with over hanging plaque
Clinical implications
- Acute recoil
- Coronary spasm
- Mechanical effects : Asymmetric expansion of stent
- Drug eluting stents
An arc of normal plaque circumference predispose to acute recoil and spasm.this is logical as the normal arc will have a fully functional medial smooth muscle which are prone for spasm.
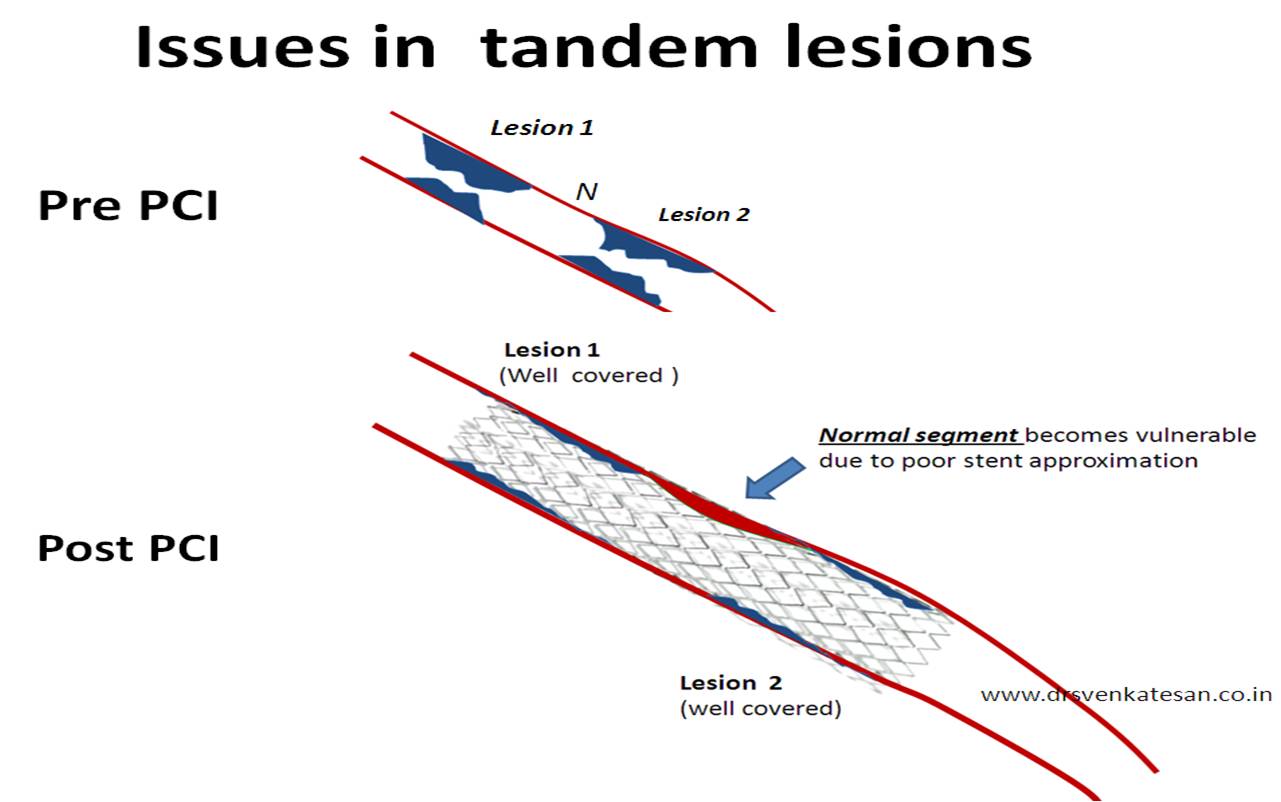
Does stenting reverse the eccentricity of plaque ?
It may not . The drag effect of major plaque mass may either result in plaque prolapse or asymmetric stent approximation or even stent crushing effect.
How does the the stents elute in an eccentric lesion ?
Stents are not intelligent enough to differentiate the plaque surface and normal surface. We also know these drugs are toxic to normal endothelium and hence are not welcome in the normal arcs of an eccentric lesion.
Since the drug secretion is uniform throughout the circumference it makes the DES a perfect misfit in eccentric lesions As we realise most of the lesions are pathologically eccentric one can guess the long term consequences .
Final message
The more we think we know . . . the less is understood .
The images we see daily in cath labs are too simplistic to make vital decisions .There are constant innovations coming up but none seems succeed in imparting common sense to majority us.(Namely direct plaque intervention can never succeed over a diffuse medical disease called atherosclerosis )
A good reference article

















{kind=link}
{kind=link}