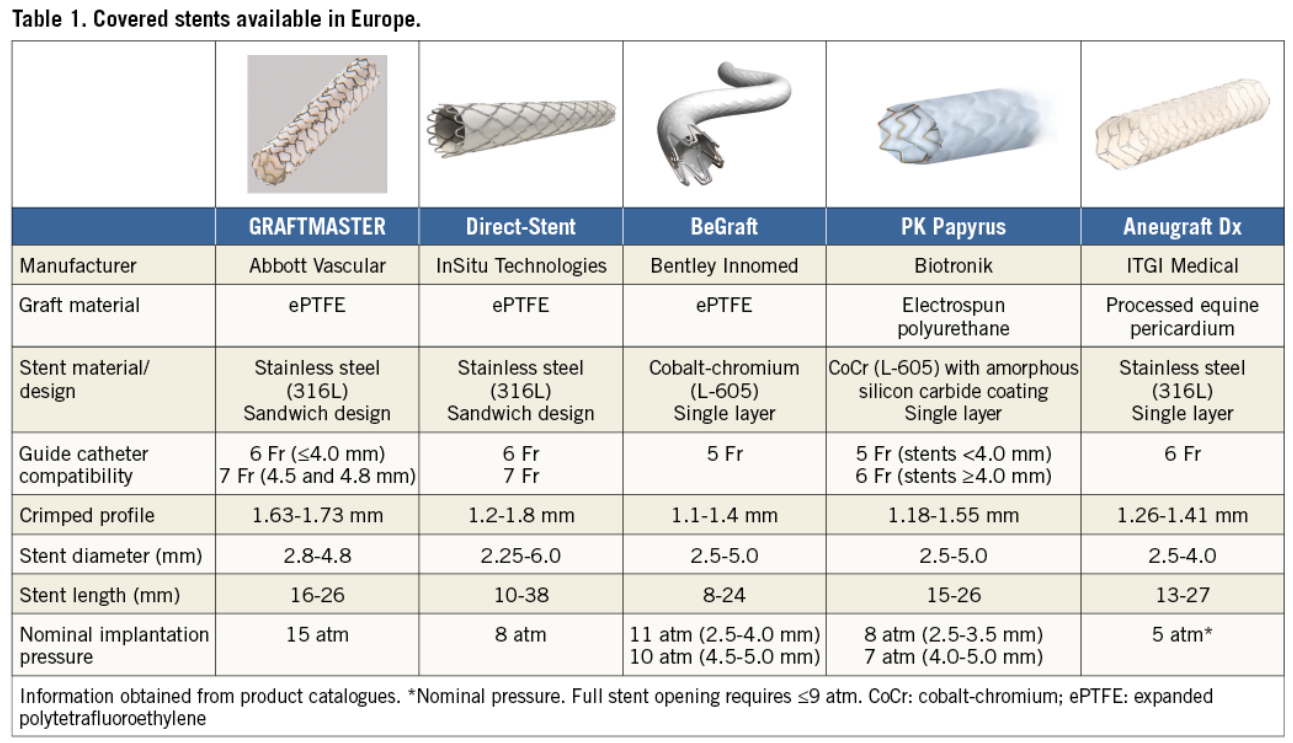
Covered stents are exclusively reserved for coronary artery perforations. Yes, that’s what we think. There has been limited exploration regarding the value of covering the complex lesions, which could prevent future coronary events .
It is possible, covered stents might play a extended role , other than perforations as in complex .friable thin capped lesions . As of June 2025 , haven’t found any such study in cardiology literature.
The recently released PREVENT study argued for PCI for patients with vulnerable high risk plaque. Ironically , it is found plaques with very thin cap ie <50microns are at risk of rupture by the radial stress of struts in the immediate or late follow up.
The thought of this study came when we witnessed high recurrent events, due to plaque prolapse, TCFA injury, new plaque ruptures, micro emboli. no reflow etc in patients with complex lesions.
Any past studies done on this aspect ?
There have been some attempts to use covered stents in degenerated venous grafts. Also, the M-Guard stent system was used in the past to seal thrombus during primary PCI. Both showed mixed results. (Gracida 2015)
Are we ready for a trial with a far fetched Imagination ?
What about jacketing and sandwiching the coronary lumen internally with a synthetic layer of tissue? That can potentially prevent recurring events indefinitely. (It is like making a native coronary artery into a Teflon-coated tube.) The proposal may look crazy until we find a inert layer of synthetic tissue to false roof the coronary lumen. But someone can make a start.
Final message
Covered stents are not just meant to arrest blood leaking outwards, in case of perforation , it can also be used seal high risk plaques, that ruptures and leaks its content into the lumen.
*In the following document, a brief outline and proposal is written about such a study. Whoever wants to do such a study, may use it. I wish I could be an external adviser, as I am no longer attached to a teaching hospital or research center.
Postamble
Before , we begin such a study, one may look at the long term outcome of patients who had already received covered stents for perforations. This is important because, PTFE’s pro-thrombotic potential and need for additional vigilance is yet to be defined.







ORBITA trial : First let us do some harm . . . second , we shall . . !?
Posted in Cardiology -Interventional -PCI, Cardiology -Technology, Cardiology -Therapeutic dilemma, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology journal club, cardiology wisdom, Medical education, Medical ethics, Uncategorized, tagged ABUSE OF STENTS, ACC AHA ESC ORBITA GUIDELIES, CHRONIC STABLE ANGINA GUIDELINES, drsvenkatesan, HOW ORBITA TRIAL WILL CHANGE MY PRACTICE, INAPPROPRIATE USE CRITERIA AUC STENTS, LANCET ORBITA STUDY, ORBITA COURAGE BARI2D FAME 2, ORBITA IMPERIAL COLLEGE, ORBITA study, ORBITA TRIAL LANCET, ORBITA trial review and comments, ORBITA VS COURAGE, reviewing ORBITA trial study critically, TCTMD 2017 ORBITA, WAHT WE LEARN FROM ORBITA STUDY on November 6, 2017| 2 Comments »
Cardiologists at confused cross roads !
Perils of limited Intellect & Infinite greed
When not so appropriately trained cardiologists do Inappropriate things “use becomes misuse” . . . then, it won’t take much time for science to become total abuse. That’s what happened with the murky world of coronary stents .No surprise, it’s time to firefight the healers instead of the disease !
Now ,Comes the ORBITA study . Yes , it looks like a God sent path breaking trial that spits some harsh truths not only in cardiology, but also in behavioral ethics .Let us not work over time and hunt for any non-existing loop holes in ORBITA. Even if it has few, it can be condoned for sure as we have essentially lived out of flawed science for too long Injuring many Innocent hearts !
Yes , its enforced premature funeral times for a wonderful technology !
GIF Image courtesy http://www.tenor.com
Meanwhile, let us pray for a selective resurrection of stenting in chronic coronary syndromes and stop behaving like lesser professionals !
Postamble
Extremely sorry . . . to all those discerning academic folks , who are looking for a true scientific review of ORBITA , please look elsewhere !
Rate this:
Read Full Post »