Answer :
In cardiogenic shock it is A . In all others it is probably C.
While D may be considered as an essential target criteria for completing the rescue PCI
Read also
Why-we-often-follow-a-reckless-time-window-for-rescue-angioplasty ?
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, Cardiology-Coronary artery disese, tagged rescue angioplasty, rescue pci, time window for rescue angioplasty, waht is the time window for rescue angioplasty on March 31, 2013| Leave a Comment »
Answer :
In cardiogenic shock it is A . In all others it is probably C.
While D may be considered as an essential target criteria for completing the rescue PCI
Read also
Why-we-often-follow-a-reckless-time-window-for-rescue-angioplasty ?
Posted in cardiology -Therapeutics, Cardiology hypertension, cardiology- coronary care, Cardiology-Coronary artery disese, tagged after load -preload mismatch, afterload mismatch, lvedp and ef in lvf, mechansim of lvf in hypertension, waht happens to ejection fraction in hypertensive lvf ? on March 31, 2013| Leave a Comment »
Answer
The tie is between “B” and “D ”
We know in hypertensive hearts LV primarily fails in diastole . Lungs get congested due to raised LVEDP .Here is a catch . . . if diastole is terribly dysfunctional how can be systole be near normal ? (After all . . . systole is not a distant cousin of diastole !)
How is that high blood pressure maintained in spite of LV failure* ?
Is it due to well-preserved EF and cardiac Index ? or Is it due to extreme levels of peripheral sympathetic activity mediated by catecholamine surge triggered by LVF.
We have attempted to measure LVEF in patients with flash pulmonary edema and acute severe hypertension .It was a real messy echocardiography . We could not conclude much but one thing is clear in acute hypertensive LVF the LV was vigorously contracting in , probably making the option D more correct .
* The other way of reasoning is . . . it is because of high blood pressure the LVF has occurred . LV contractility has no contribution in maintaining the high BP ( Not in line with the age old concept of LV contractility a major determinant of systolic blood pressure !)
(Having said that . . . we also see patients with severe LV dysfunction with severely stunned , ventricles in association with hypertension and LVF . In fact many of the reversible DCMs are due to sudden surge in blood pressure )
Other mechansims of LVF and lung congestion is
Postamble
If this article has confused you a little , It has achieved one of it’s objective . ! I expect more from young cardiology fellows to address the issue !
Reference
This NEJM article authored by Sanjay Gandhi has almost answered the hemodynamics of acute LVF and HT .

Posted in cardiology -ECG, Cardiology -unresolved questions, Cardiology-Arrhythmias, Cardiology-Coronary artery disese, tagged intermittent lbbb vs intermittent normal ecg, lbbb, new onset lbbb normal ecg, transient lbbb on February 28, 2013| 4 Comments »
We know new onset LBBB creates considerable anxiety . We experienced a reverse situation recently . A 72 year old man who is known to have chronic LBBB for over 5 years came to CCU with vague chest discomfort .
His ECG was perfectly normal . . . every one was curious !
![]()
![]()
My ECG always looked like this doctor ! Now you say it has normalised and you say it concerns you ! I am really worried doctor !
What does it mean doctor ?
Cardiologist : I do not know . Any sudden change in rhythm even if it is from abnormal to normal is to be given importance .
Patient : Is the going bad ?
Cardiologist : I do not know
Patient : Should I get admitted ?
Cardiologist : I think so but you need to undergo few blood tests and repeat an ECG .
Patient : Oh what ? you are not sure either ! Are you not an expert in heart disease doctor ?
Cardiologist : I think I am . I wish I have an answer to your question .
Follow up
This patient was admitted in intermediate care ward and observed for 12 hours .
His enzymes and Troponin were negative . Echo showed normal LV function .
He was discharged later and adviced a stress test .
What is the the mechanism of normal ECG here ?
Intermittent LBBB due to rate dependency is common .But this man had persistent chronic LBBB for > 5 years which got normalized .That mystified us !
Can transient ischemia of left bundle accelerate the conduction ?
Posted in Cardiology -Interventional -PCI, Cardiology-Coronary artery disese, cath lab tips and tricks, cto chronic total occlusion, PCI PTCA Hardware, tagged chronic total occlusion, cto, tips and tricks on February 28, 2013| Leave a Comment »
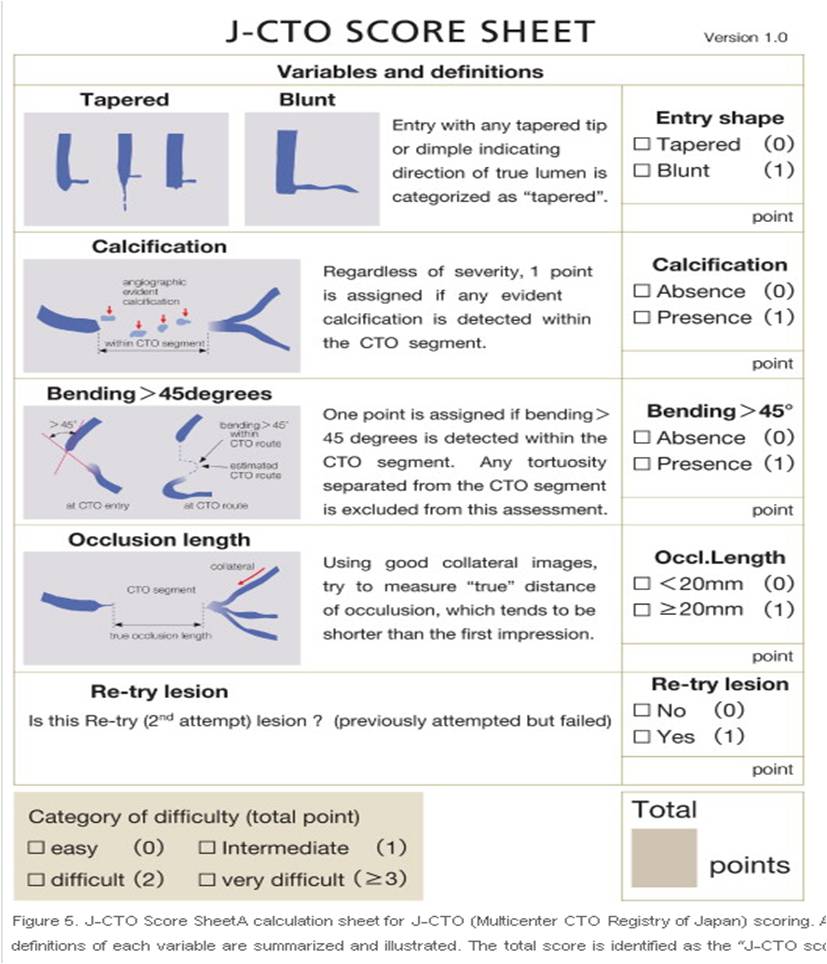
Japanese are the pioneers in CTO reopening .(I understand they do less CABG surgeries for religious reasons ) CTO is the ultimate test for cardiologist patience . it may take hours to open up a CTO (or even to abandon it .) Here is a success prediction tool from Japan .
Source courtesy : JACC: Cardiovascular Interventions Volume 4, Issue 2, February 2011
Reference
http://www.sciencedirect.com/science/article/pii/S193687981000912X
Posted in cardiology- coronary care, Cardiology-Coronary artery disese, cath lab tips and tricks, cto chronic total occlusion, Hardware techniques tips, tagged chronic total occlusion, cto, fielder xt, pci for cto, retrograde cto crossing, success in cto pci, tips and tricks on February 27, 2013| Leave a Comment »
Answer :
While each one of the above factor appears very much important morphology of the lesion is the clear winner ( Which includes , the content of the lesion , hardness , micro channels , thickness of the proximal and distal caps, the length and tortuosity of the CTO ( which is invisible ) the collateral status will ultimately determine the success)
It is becoming increasingly clear cardiologist expertise is getting less and less important .
Finally , it must be told to our younger generation of cardiologists , crossing a CTO and deploying a stent is not synonymous with success .It should result in long term sustained distal flow and make a significant impact on the patients symptoms (If at all any !) and survival.
Posted in cardiology -ECG, cardiology -Therapeutics, Cardiology -unresolved questions, Cardiology-Coronary artery disese, tagged inferior mi differential diagnosis, non infarct q waves on January 31, 2013| Leave a Comment »
We know q waves are not synonymous with Infarct . It just represents electrical activity going away from the electrode.This is why it can occur even in physiologically in many leads.
Non infarct Q wave can be recorded with
When a chamber enlarges (Any chamber ) it is brought near the chest wall the electrode may pick up the intra cavity potential that is recorded as q waves .
(The q wave in V5-V6 in severe volume overload of LV may represent LV cavity potential )
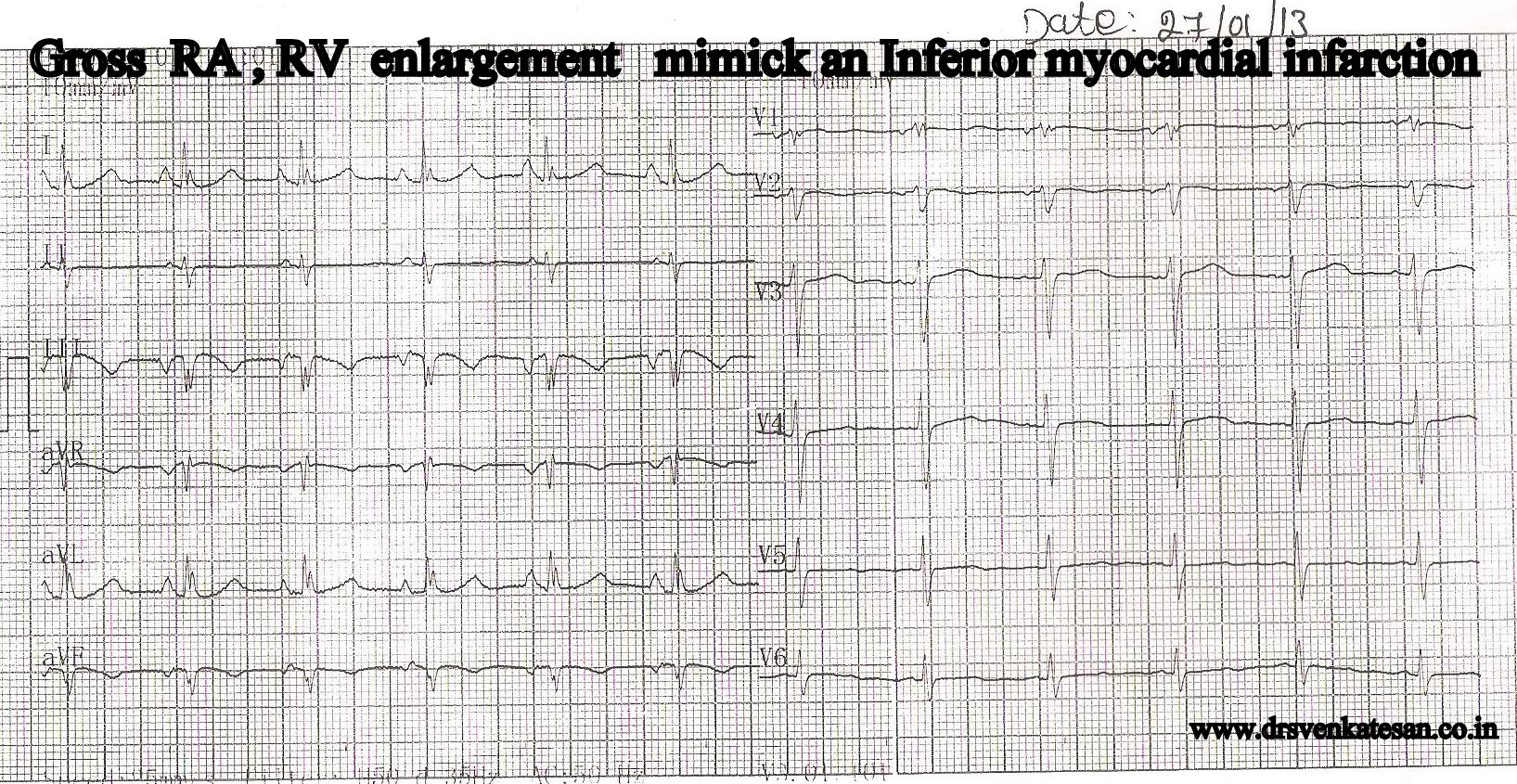
Similarly qR complex in severe RV enlargement in V1 represent RA cavity potential.Right ventricle is anatomically a difficult chamber to understand. It is located anterior below the sternum the inferior and posterior aspect of the RV is facing the diapharagmatic surface
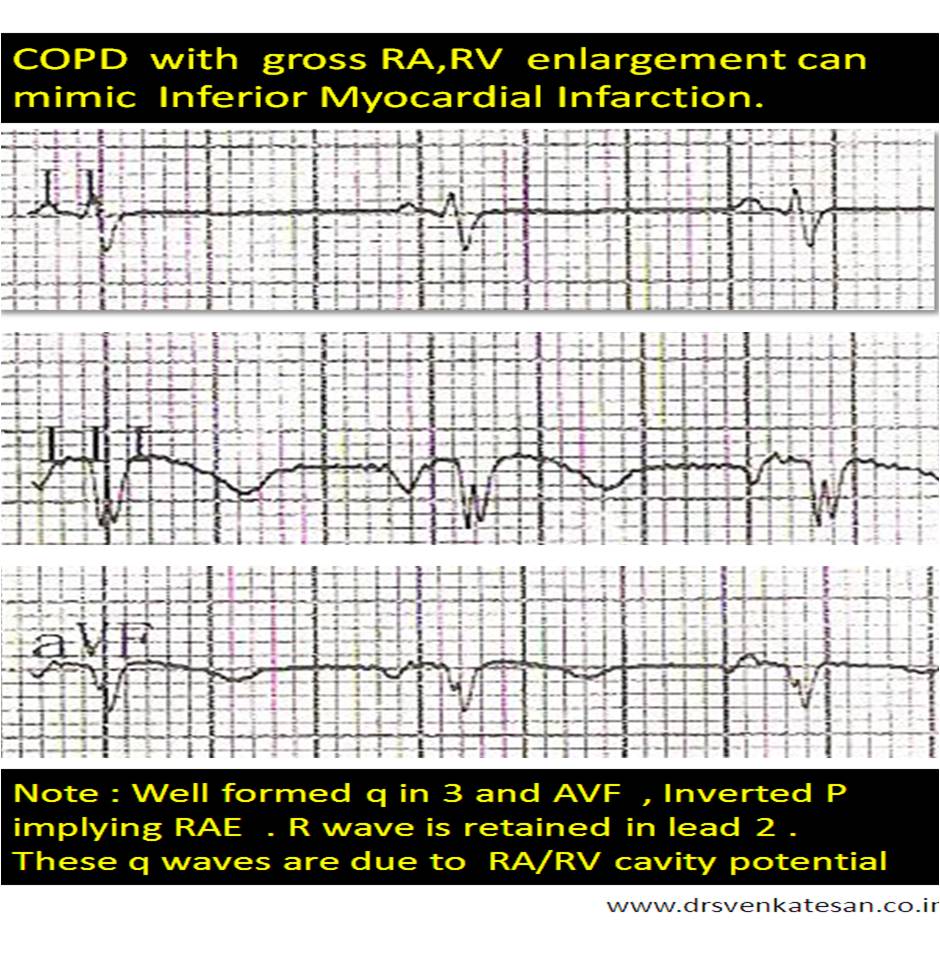
In huge RV enlargement , RV cavity potential or( even RA ) can be picked up by limb leads . While cavity potential is well picked up by unipolar pre-cadial leads , it is uncommon for limb lead record intracavitory potential. However this patient , who was diagnosed as inferior MI by a resident , turned out to be a clear case of severe pulmonary hypertension due to COPD .
Final message
One more differential diagnosis for inferior MI in ECG exists. A grossly dilated RA, RV due to COPD with severe pulmonary hypertension.
Posted in Cardiology -Interventional -PCI, cardiology- coronary care, cardiology-Anatomy, Cardiology-Coronary artery disese, Echo library and gallery, echocardiography, great illustrations in cardiology, tagged left main by echo tte, left main coroanry artery, left main ostium, rare echocardiogram images on January 23, 2013| Leave a Comment »
If only . . . we get an image like this , echo can help rule out most left main disease with conviction .
Have a close look at it ! One can get a good image of coronary ostia in short axis view . But , here it is well visualized in long axis .

I tried to put color flow within left main .
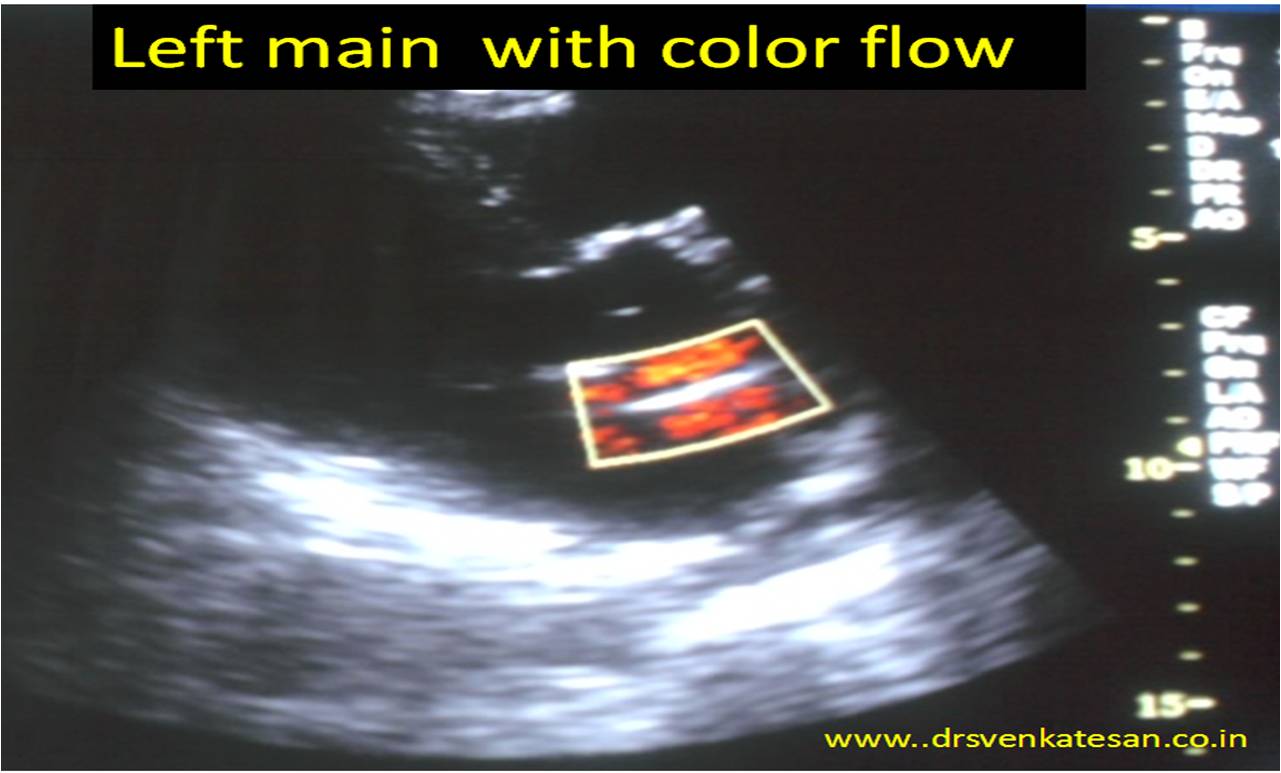
What about pulsed Doppler across left main ?
After all it needs 2mm sample volume and this left main was near 4.5mm . So keep trying !
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Cardiology -unresolved questions, cardiology-Anatomy, Cardiology-Coronary artery disese, Clinical cardiology, echocardiography, tagged discrepancies in wall motion defects, ECG, ecg echo correlation of wall motion defect, eelctrical myopia, inferior leads, inferior stemi, inferior vs anterior stemi, lvh q waves in inferior leads, mechanism of wave in inferior leads in horizontal hearts, myocardial segmental geography, rotation of heart and q waves, stemi nstemi combnations, wall motion defect in echocardiography, wall motion defectmindex on January 14, 2013| Leave a Comment »
Surprises are hall-marks of medical science . The cardiologists do get it , in enough doses from echo labs on a regular basis ! . One such thing is the total ECG-ECHO myocardial territorial mismatch following a STEMI . Human myocardial segments are divided by cardiologists by 17 segments by echocardiogram . Long before echo came into vogue , electro-cardiologists divided the heart electrically into three zones to localise MI . (Anterior , inferior and the poorly defined entity lateral walls* ) .Inferior and posterior segments are almost used interchangeably. So , when we have 17 echo segments to be fit into these three electrical category ! were bound to have some overlap . The issues of fitting in septal segments is really complex as septum is a three dimensionally engulfs all three electrical surface of the heart .
* By the way , anatomists never agreed about existence of walls in heart.They simply said , heart has smooth surfaces that blends with one another. We cardiologist have built imaginary walls and struggling to come out it !
We will try to answer the question that’s been asked here . “Inferior MI” by ECG . . . “Anterior MI” by echocardiography . How common is that ?
Possible causes for this wrong call
Technical errors in acquiring echo imaging plane or it’s interpretation is the commonest . Many times , obliquely obtained long axis view wrongly and strongly suggests a septal MI instead of inferior posterior MI. This is because in apical 4 chamber view bulk of septum (Basal and mid third ) lies in the infero-posterior region .

Perhaps , misunderstanding this septal geography is the commonest cause for erroneously calling inferior MI as anterior in echocardiography . (A simple clue is the presence of MR . (It fixes the infarct in infero-posterior zone with 90% accuracy )
Rotation and posture of heart
Alignment of the septum to the rest of the chambers can influence , how three inferior leads is going to look at the septum (There can be considerable errors -Electrical myopia ? as these leads are located distantly ) . The plane of the septum is such that in horizontal hearts septal electrical activity will be directed infero posteriorly inscribing a q waves in inferior leads rather than anterior leads . One can expect such ECG /Echo discrepancy in the following subset as well
There are three more situations , which mystified me with definite ECG/ECHO mismatch
Final message
By general rule , ECG correlates well with ECHO for localising myocardial segments . At times , it can really be tricky , and we get into above situation in echo labs.
While , it is common to observe ECGs to mimic inferior MI at the first look and subsequently echo revealing anterior infarct , the reverse is also very much possible .
The mechanisms are varied and technical issues are for more frequent than true clinical discrepancy .The issue has important management implications.
Of course , coronary angiogram will pin point the anatomy , still it also has strong limitations in localizing myocardial segments (to which it supplies ) especially with multi-vessel CAD and collateral dependent circulation .
Posted in cardiology -ECG, Cardiology -Interventional -PCI, cardiology- coronary care, Cardiology-Coronary artery disese, Infrequently asked questions in cardiology (iFAQs), STEMI-Primary PCI, tagged brugada syndrome, Early reploarisation syndrome, Hyperkalemia, Left bundle branch block/ Left ventricular hypertrophy, pericarditis, sgarbossa criteria, STEMI differential diagnosis on November 11, 2012| 4 Comments »
Top 5 conditions that closely mimic and often mistaken for STEMI !
ERS
The repolarisation is due to K + efflux . The K channel porosity is subjected to high degree of genetic variations .If the repolarisation starts even by 10 milli- second earlier, it would have early take off from descending limb of R wave and the J point ST segment appear elevated.
* STEMI in ERS : The issue becomes too delicate , if a patient with ERS develops a true ACS . ERS being a common ECG pattern in general population , it is not wise to label every chest pain in ERS patient as benign . Suspicious ones demand observation in step down units , at least !
LBBB
“Any patient with LBBB & chest pain . . . suspect MI” .
Unfortunately, this rule is too reverently followed by physician community. In fact , ACC/AHA guidelines reinforced this behavior , as it added a key word in their STEMI guidelines “New onset” or “presumably new onset ” LBBB is an indication for PCI/Thrombolysis .( Physician presumption is a too delicate thread to hang our concepts ! )
Every LBBB is new onset unless you have a documented proof otherwise . . . it seems to suggest !
Probably , this is the reason many of the LBBBs are thrombolysed when they present to ER in an acute fashion . Of course , we can apply criteria of Sgarbossa to differentiate ! however flimsy it may appear . It help us to exclude few benign LBBBs. Still , Sgarbossa will struggle to differentiate an acute STEMI in Chronic LBBB from an acute LBBB in old AWMI .
Simply put . . . even old MIs are at risk of acute intervention if they have LBBB and vague chest pain !
How to overcome this ? Always rely on clinical features . If STEMI is causing the LBBB , it should be a large extensive one and you can not expect the patient to be comfortable .(Logic would suggest necrosis of large parts of IVS is necessary to cause LBBB ) Chronic LBBBs are relatively comfortable .
Of course , there is one another issue to comprehend ie transient ischemic LBBB .We do not know the true incidence and long-term significance of this entity . Here , LBBB is not due to necrosis of the bundle but due to ischemia . (Almost impossible to differentiate it from rate dependent LBBB with aberrancy )
Role of enzymes and Echocardiogram in LBBB and suspected STEMI .
You can always ask for Troponin T / CPK MB .(They are helpful only if 3 hours have elapsed , can we afford to wait ? ) . LBBB due to STEMI will purge a large quantum of cardiac enzymes from the infarcted zone . (So a marginal elevation is not going to help!)
Unfortunately, LBBB can induce wall motion defect in septum that may awkwardly simulate an ischemic wall motion. Even experts have erred in this . One clue is, the motion defects can not extend into anterior wall . It is confined to septum ,the second clue is a little delayed post QRS thickening of IVS (Septal beaking sign will vouch for benign LBBB with fair degree of success )
LVH
Hyperkalemia.
With aging population and rampant acute and chronic renal disorders it is becoming a daily affair to get calls from medical units for ECG changes .We know the rapidity of efflux potassium is responsible for ventricular re-polarisation .Phase 2, and 3 are K + exit zones. This is the same phase ST segment and T wave are inscribed.In hyperkalemia K + accumulates inside the cell and keep ST/T segment elevated .T wave also becomes tall . It can mimic both as hyper acute STEMI .
Read a related article (Dialyisable current of Injury )
Pericarditis
Link to Read regional pericarditis
Brugada syndrome
Brugada syndrome is an ECG -Clinical complex in which ST elevation in pre-cardial leads is associated with ventricular arrhythmia. The defect lies in sodium channel . It reflects a mis -match between RV and LV epicardial repolarisation forces .It keeps the RV epi-cardial current afloat and the pre-cardial leads facing the RV records ST elevation that mimics STEMI. It often shows a RBBB pattern and varying patterns of ST morphology . The ST segment is also subjected to dynamism , due to change in autonomic tone and myocardial temperature .(Febrile VTs)
After thoughts
Other close contenders for the top 5 slots
Myocarditis
Acute pulmonary embolism
Dissection of aorta
More
(Cocaine hearts / Coronary arterial spasm / LV dyskinetic segments and LV aneurysms were not nominees ! )
Posted in Cardiology - Clinical, Cardiology -unresolved questions, Cardiology-Coronary artery disese, tagged dyspnea, dyspnea during ischemia, mechanism of angina equivalent on October 31, 2012| Leave a Comment »
Anginal equivalents are distinct (often vague ) symptoms that occur in response to myocardial Ischemia , instead of angina. Dyspnea or shortness of breath is the commonest anginal equivalent . The incidence and exact mechanism is not clear. Both angina and dyspnea are sensory events . Both are perceived at the level of cortex. Angina occurs when ischemic muscle triggers pain signals from the nerve twigs engulfing the myocytes membranes and the vasavasorum.
Dyspnea during myocardial ischemia is multi-factorial
Out of the above eight factors which is most important ?
The most popular and easy to comprehend mechanism is number 5 : Ischemic diastolic dysfunction .
(Fellows will be appreciated if they know this ! )



