An animated version

An animated version
Posted in cardiology congenital heart disese | Tagged left vertical vein, snowman tapvc, tapvc, tapvc animation, Total anomalous pulmonary venous connection supracardiac | 1 Comment »
Posted in Aortic stent grafing | Tagged aortic aneurysm, aortic stent graft, endovascular reconstruction of aortic aneurysm, mechanism of aortic stenting, stent graft | 2 Comments »
In HCM every myocyte is genetically made defective . Myofibrils are in disarray every where . Still , can we identify some vulnerable zones that acts as arrhythmic focus ? If that is possible , we have a opportunity to abate that focus .
In HOCM , which is the most stressed area ? LVOT ? Septum, ? When we say stress , it can mean either mechanical or electrical .

Does electrical instability involve the same zone as mechanical stress ?
How often VT originate from LVOT in HCM ? For this we have good clinical model _, the patients who underwent alcohol septal ablation.
What happens to the incidence of VT post septal ablation ?
“It is reported post septal ablation the incidence of SCD becomes equal to general population” (Read the paper below )
If that is true , it is obvious the arrhythmic focus is also ablated along with LVOT myocardium .

Though many studies claim so ! It fails to convince us . HOCM is a diffuse disease of myocardium. Even a cluster of myocyte disarray with fibrosis can be a future focus irrespective of it’s location .
However , it is always possible relieving the mechanical stress of the LV can definitely reduce the likelihood of an electrical event .(Even if the arrhythmic focus is intact elsewhere !)
* We know RVOT is developmentally arrhythmia prone zone . We also know HCM involves RVOT (After all , IVS is legally shared by both ventricles ! ) . Some of the monomorphic VTs with LBBB morphology may originate from RVOT in HCM .
Management of recurrent VT in HOCM
Reference
1.A case report for successful ablation of VT in HOCM http://www.ncbi.nlm.nih.gov/pubmed/9255687
2.http://www.ncbi.nlm.nih.gov/pubmed/23076968
//
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, Cardiology-Arrhythmias, Infrequently asked questions in cardiology (iFAQs) | Tagged hocm, hypertrophic obstructive cardiomyopathy, lvot vt in hocm, mechanism of vt in hocm, mechansim of vt in hcm, septal vt in hocm, vt in hcm, vt in hocm, vulnerable spots in hocm | 1 Comment »
Systemic hypertension (SHT ) is the commonest clinical entity encountered in cardiology consultations . 95 % of HT is considered primary. The remaining 5 % form the most important class of HT (Secondary to renal parenchymal, vascular , endocrine, etc)
How intelligent is this traditional classification of HT ?
The incidence of primary and secondary HT varies depending upon the level of investigation we do . One of my regular patient who gets to me for HT .He is 42 year old man works in financial institution with lots of work stress and he was marginally obese as well . He was investigated for all known cause of secondary HT and every parameter was found to be normal and was being treated as primary HT.
When he was about to leave my clinic he bowled this google !
Doctor , why do you call mine as primary HT ? . . . When you yourself say my stress and weight is responsible for high blood pressure ?

Valid question is it not ! . . . I told him “somehow” , we have not been taught in medical schools , to consider stress of life as a factor responsible for developing secondary HT !
Final message
Strange definitions in medicine continue . Not every one with high stress levels develop HT .There are some unknown factors operating .Till we know that we will keep calling them as primary HT .
( Who knows the man who raised this question may show up with adrenal hyperplasia or a renal parenchymal dysfunction 5 years down the lane !)
We live by perceived knowledge on a moment to moment basis ! . Ignorance tries to lock the doors of knowledge .
But we continue to open new doors . That is the only purpose of medical research !
Posted in Hypertension | Tagged essential hypertesnion, hypertension, priamry vs secodary hypertesnion, renal hypertension, secondary hypertension, stress and obesity related hypertension | Leave a Comment »
Q waves are neither sacred nor sinister waves . It represents either of the following .
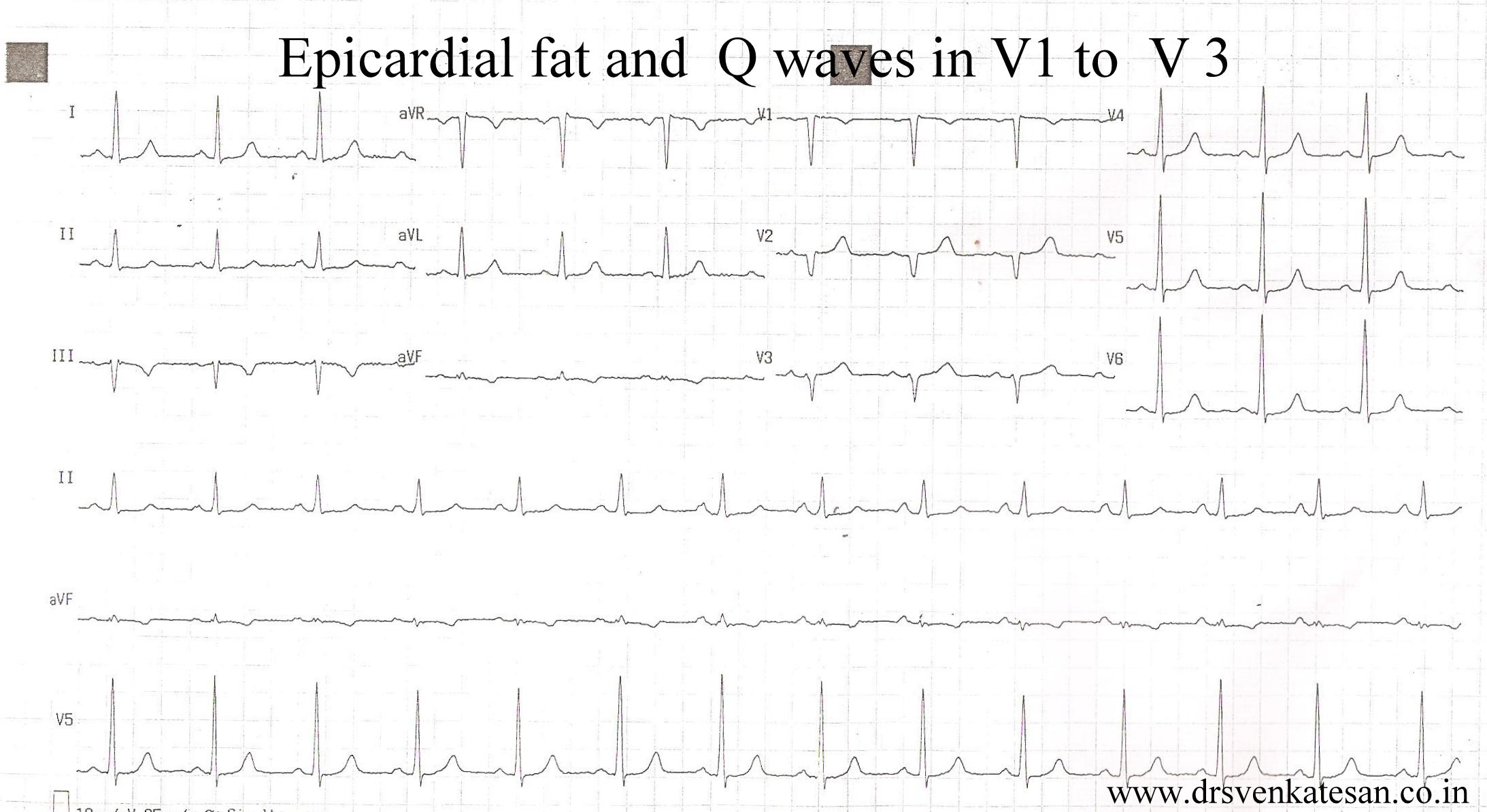
Here is young women of 42 years with a diagnosis of old anterior MI for over 5 years ( Getting a dedicated care from a cardiologist! The prescription included Imdur/Betaloc/ Statin/Clopidogrel and Aspirin )
This was the ECG . It was very convincing for old ASMI.
It happened , I did an echo for her .
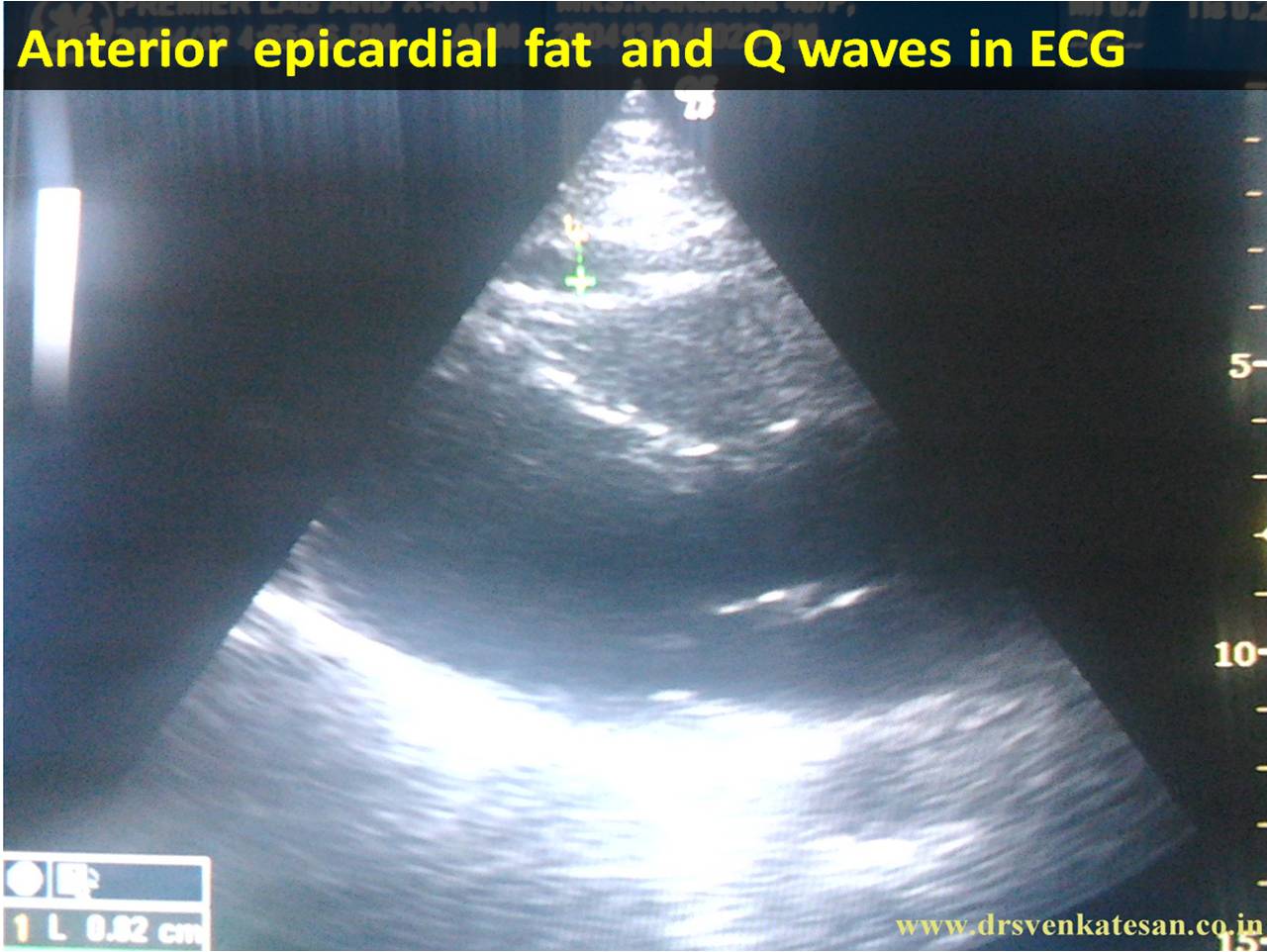
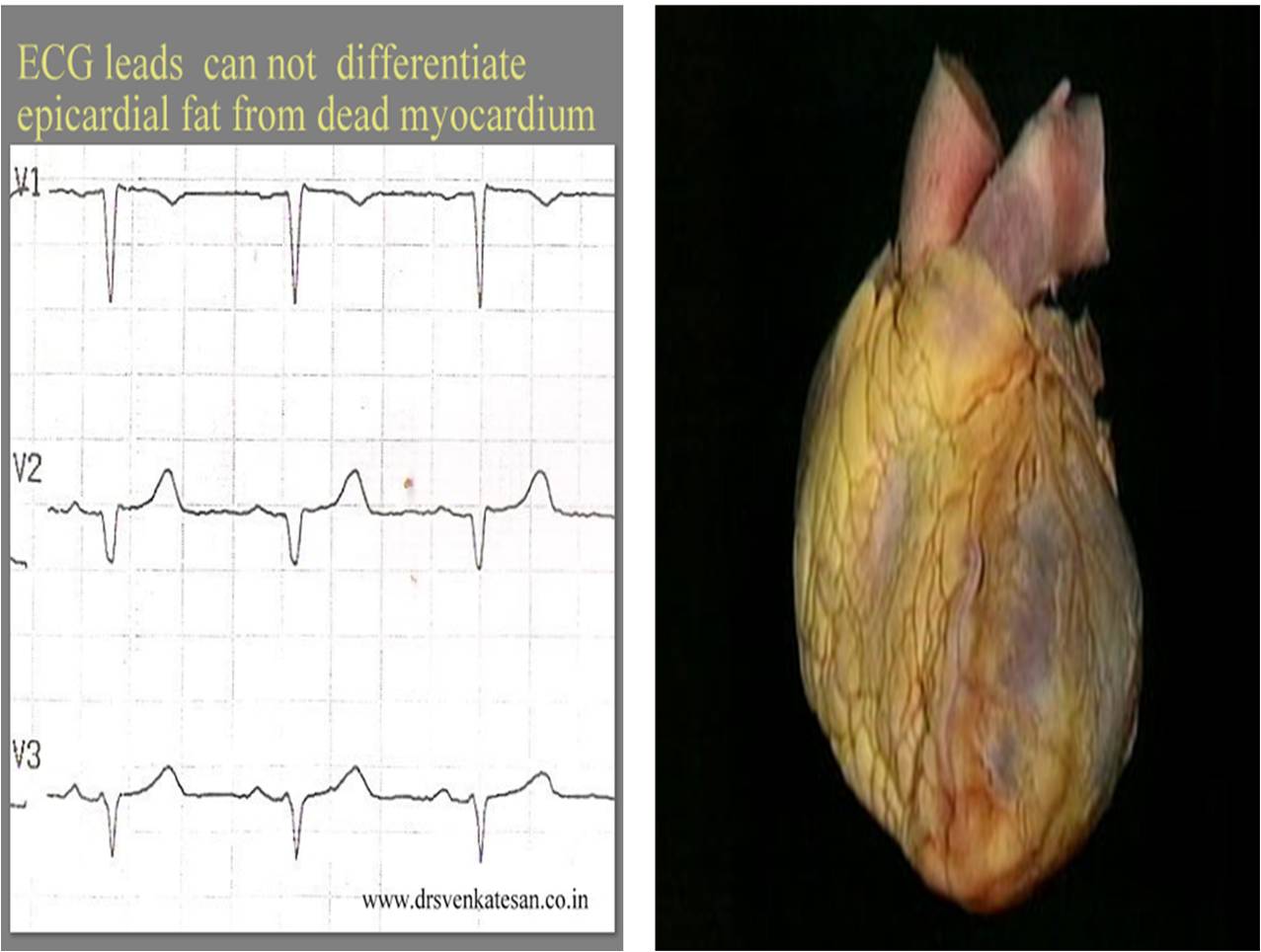
She lacked wall motion defects even after a meticulous search . Instead she had a good layer of epicardial fat measuring 9 mm .That was more localised in anterior wall extending little to LV apex.Her EF 65 % .
*She was a fairly obese (not gross ) individual with a BMI of 34 .The fat pad thickness was not that huge , I thought , still it was producing the q waves . I have seen much thicker fat pads with good R waves in ECG . I wonder , is it the type of fat that adds up to electrical insulation ?
This patient was sent back to me again for ruling out ASMI . Echo was done two weeks later . No evidence for ASMI could be detected.
What is the normal thickness of epicardial fat pad ?
It is less than few mm . Exact normality is not known .(Empirically < 5mm ) it is very rare for fat deposition in infero posterior aspect , except in morbid obesity.
What is the function of epicardial fat ?
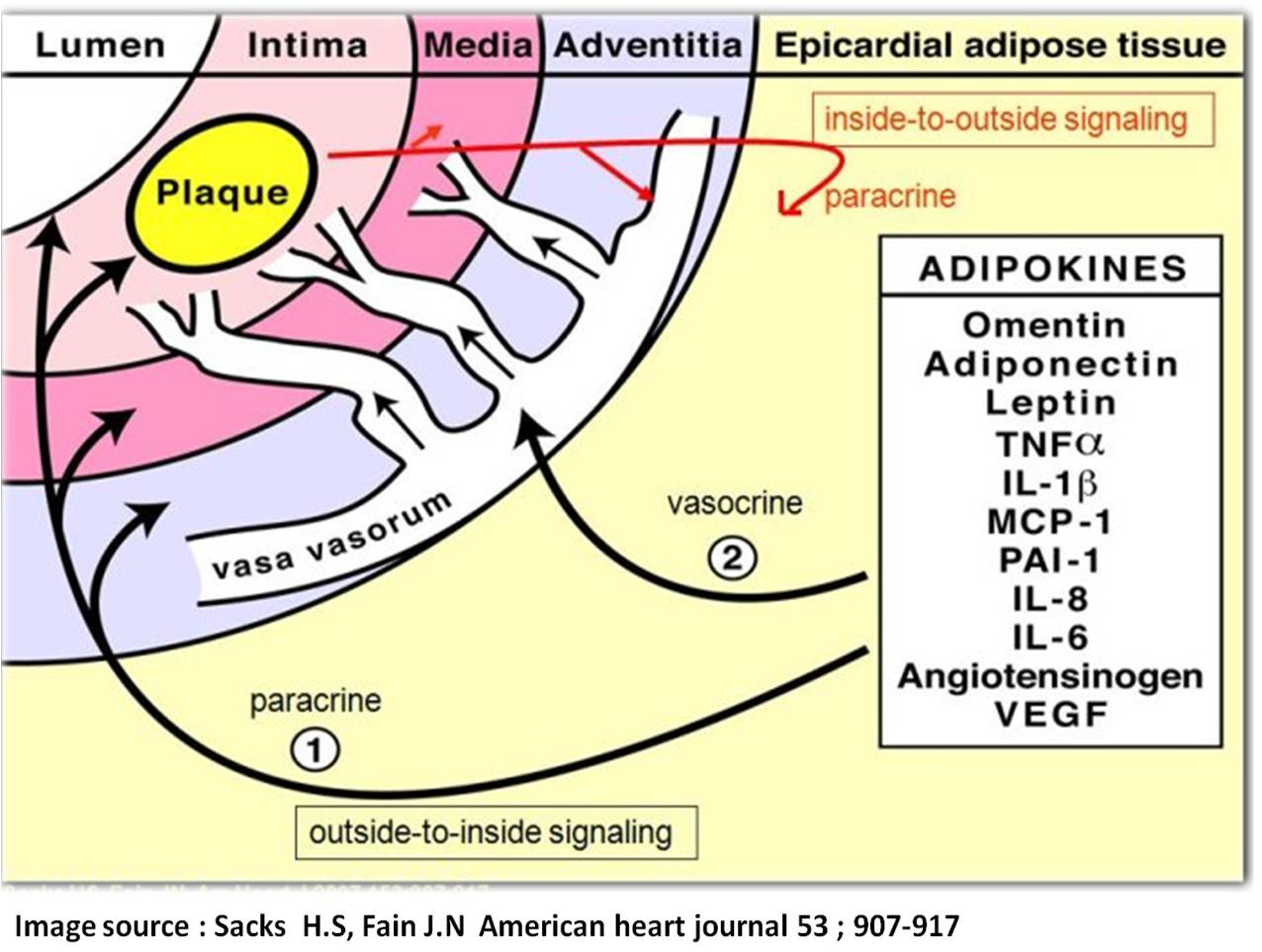
Role of epicardial fat depot in the genesis of atherosclerosis
Subcutaneous vs Epicardial fat.
We know thick chest wall can also interfere with ECG. Epicardial fat is more likely to record q waves than sub cutaneous fat , as the insulation is more closer to heart in epicardial fat . In thick chest wall current leaks from heart and well scattered hence poor R wave is more common in such situations rather than q waves !
Following things can generate q waves (Other than Infarct )
Final message
In obese men and women anterior Q wave can be misleading .Such medical errors can be so convincing .
After thought
If epicardial fat can extinguish R waves and replace it with q waves , these innocuous looking fat pads has every reason to influence the ST segment shifts during an episode of ACS as well ! . Isn’t ? . If so . . . how reliable is our ECG criterias to diagnose acute coronary syndromes in grossly obese men and women ?
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, Cardiology -unresolved questions, Clinical cardiology | Tagged epicardial fat and q waves, non infarct q waves, pesdo infarct patterns in ecg | Leave a Comment »
News : It seems the pharma companies are worried about the new MCI (Medical council of India ) guidelines that restrict sponsorship for conferences and freebies to individual doctors . They think it is a big set back as it may interfere with doctor’s education and knowledge !

They have proposed new amendments and has asked the health ministry to advice the MCI accordingly .(ie To help them bring back the corrupt and bad practices that influence doctors prescribing behavior !)
It is true , for the growth of medical science , we require some sort of a business model and tax holidays for the companies for true & land mark discoveries . Currently the MCI allows to sponsor medical events or a conference for an institution or organization . But what these companies want is official permission to provide incentives to individual doctors and influence them ! . More shockingly they said doctors knowledge will suffer without these industrial support . It is an outright insult to all doctors who get educated for over decades* . In fact the heads of pharma companies require few lessons from the medical fraternity , how many drugs with dubious scientific value is playing havoc in health of the society !
Of course ,we can not blame the pharma companies for all . It is a collective evil.
Counter point
*This is a second slap on the face of medical profession ! I am sorry to say this , many of us ( Including the blogger ! ) are some way responsible for this state of affairs . Shockingly , few of our colleagues are proud to have illicit relationship with drug companies ! Younger generation no longer consider this as an offense , since they are born and brought up with capitation fee as their principal fodder. Commercial forces has taken over medical profession . Many of the colleges are owned by business barons and alcohol vendors in India . It is a well known fact , MBBS seats are now sold for 50lakhs (like 3 bed room flats ) . Agents transact black money in secret basements of medical colleges once considered as temple of the noble profession .
So what is in-store for the future ? . . . Self regulation is best regulation . . . Mahatma told us ! . It may be the most idealistic solution . . . but currently it appears self regulation is as bad as no regulation !
Link to the article
Posted in bio ethics, cardiology-ethics | Tagged doctor drug company nexus, ethics in medicine, freebies pens and doctors drug company, hippocrates oaths ethics, industry sponsorship of drug trials, MCI regulation and doctor ethics, medical practice ethics', pharma companies and doctor sponsorship | Leave a Comment »
Why should mitral annulus gets calcified ? . Degenerative calcification can be benign in elderly . If it occurs prematurely (say < 55 years ) there is enough reasons to worry . This may represent a systemic vascular inflammation and is considered a surrogate marker for athero- vascular -sclerosis . A study from Cidar Sinai , Los angels has well documented the link way back in 2003 !
This is a large study involving 17 735 patients (who were investigated for symptoms of CAD ) were screened.
The incidence of MAC was high (As expected !)

Image source S.Atar , Heart 2003 : 89, 161-164

Posted in cardiology -Therapeutics, Cardiology -unresolved questions, cardiology women, Cardiology-Coronary artery disese, echocardiography, MVPS, valvular heart disease | Tagged annular vt, mac, mitral annular calcifcation, mitral valve calcification and cad, posterior mitral annulus calcification, vpds in mac, vpds in mitral annular calcification | Leave a Comment »
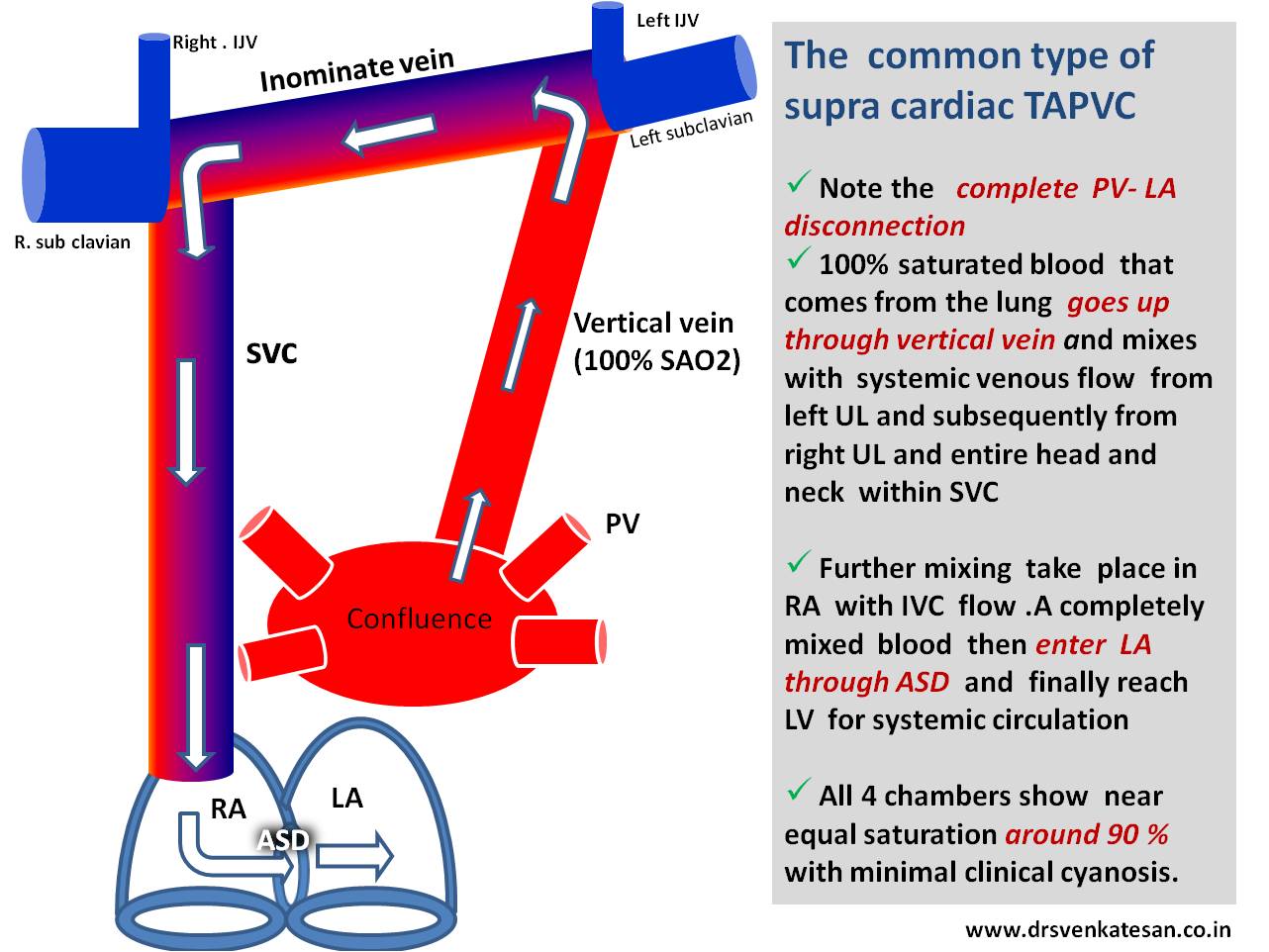
While 2D echo visualizes the LSVC , it is the color Doppler flow (in blue ) that confirms the flow going away from transducer towards coronary sinus .Please note , if the LSVC shows red flow it indicates the left vertical vein and the flow is from below up .This is supra cardiac TAPVC . It makes immense embryological sense to understand LSVC and and left vertical vein are both same entities only the connections are different .
Click over for a high resolution Image
Posted in Echo library and gallery, echocardiography, Infrequently asked questions in cardiology (iFAQs) | Tagged dilated coronary sinus, echocardiography of lsvc, lsvc, persistence lsvc, supra sternal short axis view for lsvc, tapvc vs lsvc vs left vertical vein | 1 Comment »
Those who answered “Yes” , can leave this article . Those who answered “No” read further .
* Logic would tell us myocardial revascularisation should correct stress induced ischemia and it should disappear promptly . This does not happen in all cases real world ! That is why medicine is different from mathematical science .
Some of the reasons for persistence of stress positivity even after an apparently successful PCI are . . .
* Optimal time to do EST for assessing the efficacy of PCI/CABG is not established .Six months may be the reasonable point .If done within 2- 3 months it may end up in embarrassment for the Interventionist . (So only it is kept at 6 months , this also help us greatly as we can always blame it on poor life style control and progression of the disease !)
** No reference for this , a personal observation .We know Q leads following MI , will show ST elevation during stress test especially if the segments are dyskinetic . In leads diagonally opposite to q leads , ST depression is observed . This may not be a evidence for true ischemia . It probably represents ST drag due to mechanical stretch .
Posted in Cardiology - Clinical, cardiology -ECG, Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, chronic total occlusion (CTO), Clinical cardiology, cto chronic total occlusion, Diabetes and Heart, excercise stress test .EST, Infrequently asked questions in cardiology (iFAQs) | Tagged does tmt become negative following pci, est following pci, excercise stress test following pci stenting, pci in multivessel cad, ptca and pci, ptca and stress test, stenting and tmt positivity, stress positivity after pci, stress test in cad, tmt positive and pci | Leave a Comment »
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology- coronary care, cath lab tips and tricks | Tagged bifurcation lesion, bifurcation pci, carina plaque shift bifurcation lesion, medina classification, true bifurcation angle | Leave a Comment »



