A 32-year-old high-profile businessman was advised Holter monitoring for a few ectopic beats during routine screening ECG. The 72-hour extended Holter monitoring picked up a single short pause with a blocked P wave and reported as doubtful Mobitz type 2 AV block.
The cardiologist in-charge, told the patient that findings are significant, and he would need further investigation. He was referred to their associate center for an EP study. After hearing about the procedure ,the patient was freighted about inserting multiple catheters inside his heart.
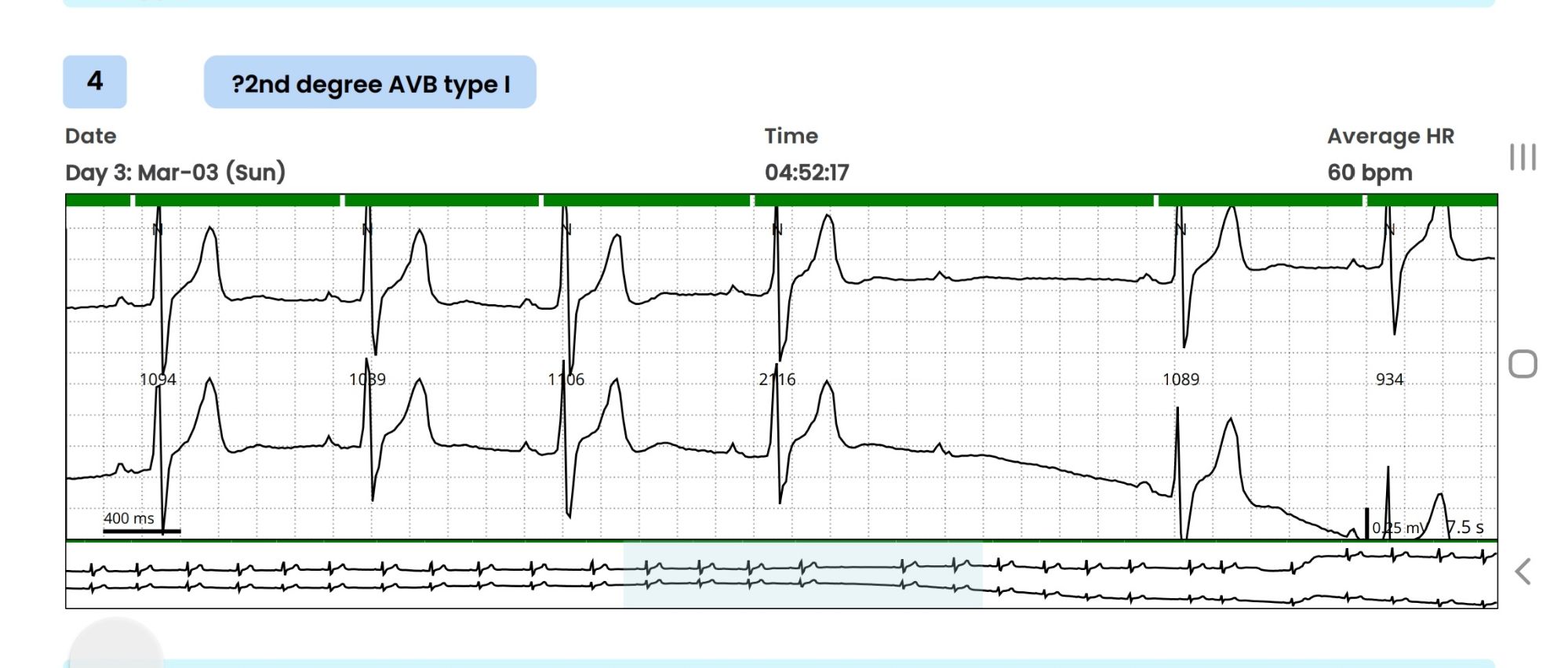
This was the time he consulted me with Holter report. It was indeed a missed QRS after a well inscribed p wave , recorded at 4.57 AM, It is a 2nd degree AV block, may be Mobitz type 2, . What if ? It could still be be blocked atrial ectopic. (Pseudo AV block) Both preceding and following PR intervals seemed to be non varying . The following QRS was narrow. I don’t know, whether a single blocked P could by any way a concealed Wenke -Bach. I didn’t have calipers to measure the PR accurately though. The baseline heart rate was around a vago-genic 60/mt, that was comforting . He had his echocardiogram done already and was normal.
What does the guidelines say ?
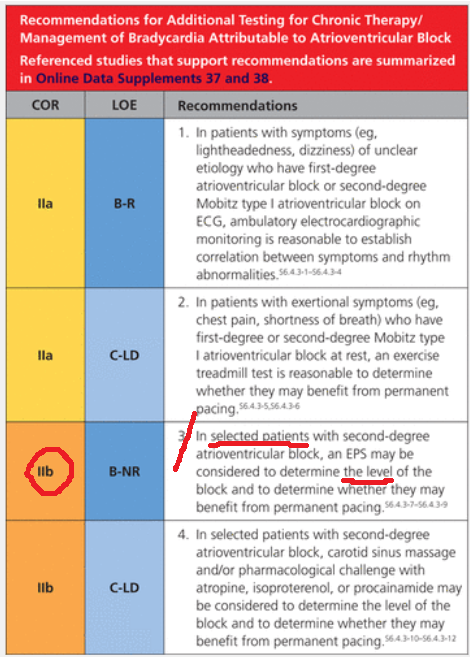
Guidelines are short of evidence , it was as vague as my thought process . It suggested EP study in selected patents with asymptomatic second degree AV block . My fellows tell, it is just 2B indication (To-be frank, 2-B indications should be called as a junk recommendation ) which would mean if you wish you can do a “potential harm”
I asked the patient two questions.
1.Does he have any symptoms like dizziness or syncope ?
Absolutely nil.
2.What is his functional capacity?
Excellent.
That’s great. Within a minute or so , I could confidently confirm, the non-seriousness of the Holter tracing. I asked him to forget everything, and sent him home, with reassurance, taking on myself a miniscule risk of missing a true AV block and its consequences. He thanked me profusely with so much gratitude. Every thing was hunky-dory , then , this thing happened. When he was above to leave the office, he came back. “Doctor, I forgot to tell, my father died suddenly at the age of 48 apparently by a heart attack” .I must admit, I was taken aback the moment he told this.
What an important past history, I failed to elicit earlier. As he left my room, I called my secretary to give a Suo-moto appointment to him 2 weeks later with a plan of TMT and possible CT -angiogram. Till late in the evening, this patient’s Holter recording ran in my mind. What was that reason for original VPDs that invited a Holter test and the subsequent documentation of Innocent appearing AV block ? Are they interconnected or inherited ? or Is it really Ischemic ones, that took his dad’s life?
The concern amplified, when I recalled about a review in EURO-PACE journal , that showed mutations of almost every structural sarcolemma proteins like Desmin and Desmoplakin can present with isolated electrical defects with or without LV dysfunction.(Brandão M, Desmoplakin Cardiomyopathy: Comprehensive Review of an Increasingly Recognized Entity. J Clin Med. 2023 )
Leaning on EP’s shoulder
That was enough for me to make a compelling call to my EP colleague, for a quick chat about this unique patient. We discussed for 15 minutes, right from Padua University paper to all the Brugada variants.(Ref 3) In the end, the basic doubts remained as before. However, the patient was advised for an EP study primarily to know the HV interval and the possibility of diffuse distal disease. The possible need for a MRI study to rule out silent arrhythmogenic intramural granulomas was also discussed. My EP friend poked me with more academic toxemia. He said a screening test called cardiac-arrhythmic genome analysis is available in certain European centers. Ref: Isbister, J.C., Semsarian, C. The role of the molecular autopsy in sudden cardiac death in young individuals. Nat Rev Cardiol 21, 215–216 (2024).
I said enough is enough , and requested for hanging up the chat.
Final message
AV blocks, even Mobitz type 2, can occur at normal times of heightened vagal tone.(Massie Block-Ref 1) But, if there is something unusual in the clinical history, be ready to investigate until the arrhythmia, or at least the anxiety disappears.
Reference










