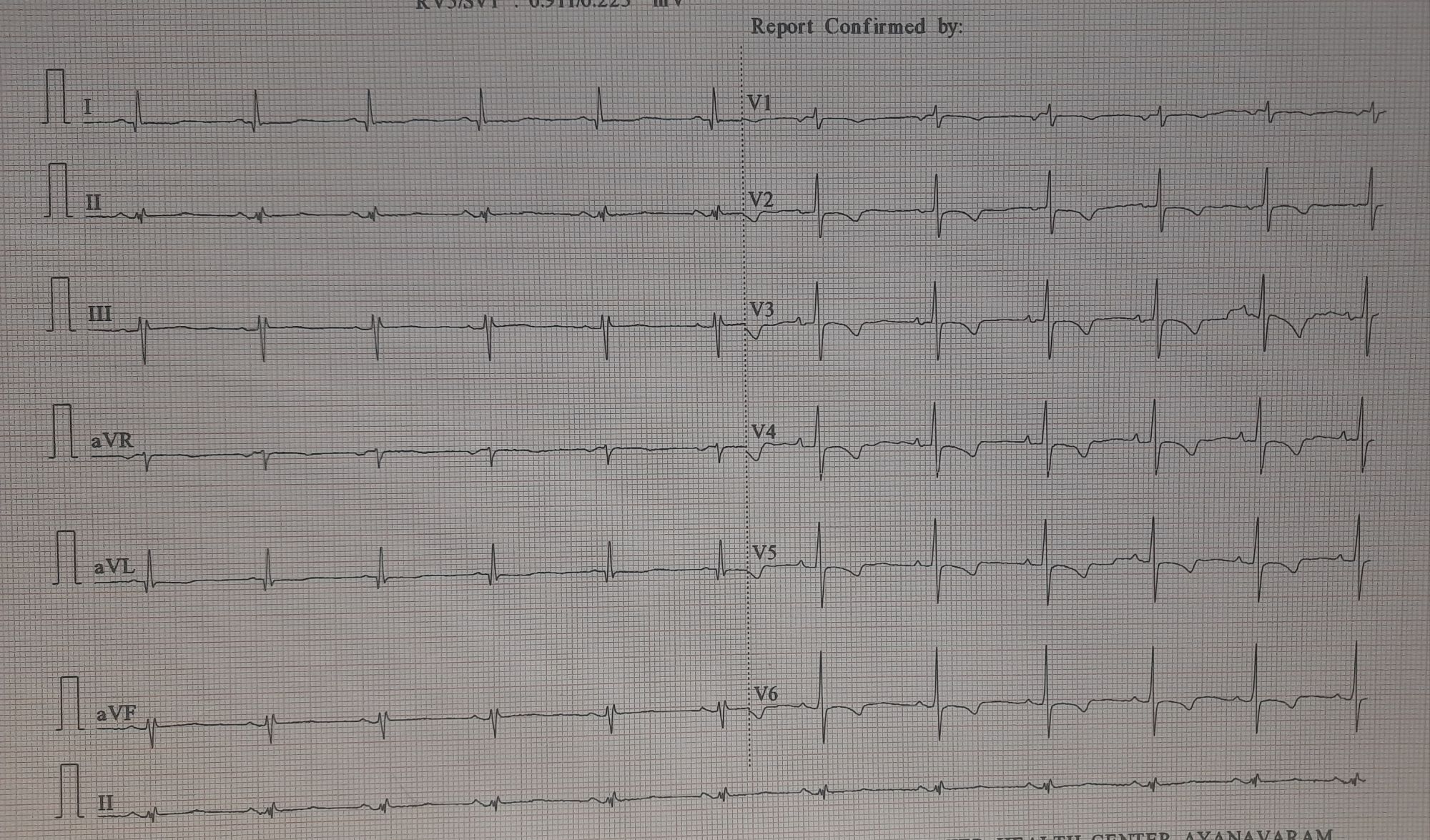
How do you report this ST segment ?
A. Isolated ST depression
B. Isolated T Wave Inversion
C. Combination of both
D.Primarily T wave Inversion ,with secondary ST dragging
Answer: Response C, is logical, but applying some ionic sense to the various repolarisation currents in the left shoulder region of action potential , it is the clash between late phase 2 and the premature phase 3 activity, that deforms the initial limb (forward) of T waves , dragging and effacing the ST segment mimicking ST depression. This we have proposed to call it as ST drag effect by T waves. (ST drag is generally more benign , than ST segement depression that begins at J point.
Clinical significance of such ST segment
Without knowing the symptoms or the reason for which this ECG was taken, we shouldn’t interpret this ECG. In this case, it was taken in a 36-year-old woman, routine health check and who has no specific symptom. This almost rules out an ACS or even a CCS. Firther, the fact that the heart rate is normal rules out demand side ischemia as well. Very likely, it should be LVH or anemia or some other systemic medical conditions. (Rarely, neuro-adrenergic-emotional signals from brainstem can tilt the ST segment like this. (Tansient Tako-subo equivalents)
Next step
However, we can’t leave her alone. She needs an echocardiogram to rule out any subclinical myocardial disease. TMT would seem to be a necessity, but false positivity is very likely.( A flamboyant cardiologist would order a CT angiogram either striaghtaway or a day-care radial angiogram. Nothing wrong with that, as long as the patient insists on reaching the bottom of the truth)
What will you do?
Will sit with the patient for atleast 15 minutes, listen to her daily activity ,past history and look for any subtle symptoms, and then decide. It needs lots of courage (or Ignorance) to leave her without any further Investigation. Echocardiogram is a must. (Have seen a HCM variants like this ).TMT is redunant, if her excercise capacity is excellent.
Final message
One more concept on ST segment can be extrapolated by curious observation of some of the ECGs who present at ER. . It is the secondary ST sagging by primary T wave downward forces. (Pushing ST up is also possibe , as we already know it as ERS pattern )
Postamble.
We know, the S point (Technically J ) in ST segment is well defined , while the end of ST segment is hidden in deep mystery in many clinical situations.Mind you, a flattish ST segment, with absent T wave can be an aboslute normality. Here, you can’t measure either ST segment or even the QT interval.
Reference