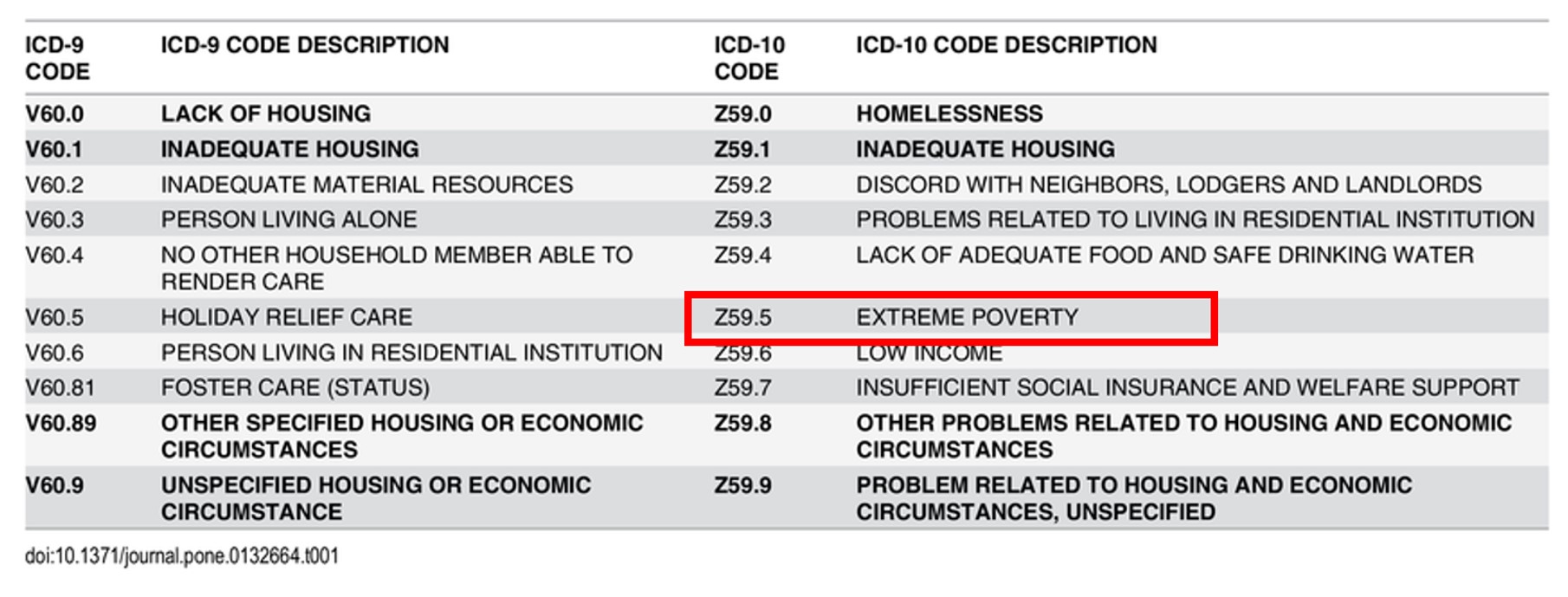
Poverty is a cruelest disease of mankind , the infective vector is not any deadly HINI or retro virus , but mostly the fellow humans themselves ! This is why WHO has included poverty in the ICD code (Z59.5 ) as a disease .

I used to wonder , as a member of Noble profession , should we fight against this disease or be happy to spend my entire life time cleaning the coronary arteries of affluent human-beings and earn few bucks !
Can growth of money eliminate poverty ?
We may think so . . . but it doesn’t most times .Of course , affluence bring more jobs to the poor , logically it should alleviate poverty. But , we know the reality. Its not that easy concept to understand . However we have robust evidence for the opposite ie affluence can aggregate poverty .
If poverty is a disease & if mindless affluence is an Indirect cause for it , then affluence also becomes a potential disease , Is in’t ? Will WHO include it in ICD listing ?
May I propose Z59.5A to be called Uncontrolled & manic desire for affluence ? Since it is made at the cost of fellow humans , it should be clubbed along with poverty as a worrisome disease. Once its included in the ICD manual , I guess it will be unethical to ignore this disease.
We all aim for growth in life .Nothing wrong in that .There are many facets of life that requires growth. Unfortunately , for most homo-sapiens , growth is synonymous with multiplication of money . . . nothing else seems to matter ! Money when it grows unregulated , begins to control you and hijack your body and mind .
One more issue to comprehend is , rapid growth of money is possible only at the cost of something (or someone) else – Akin to cancer cachexia ,it depletes the body (Earth ) of it’s resources ( Nature abuse , extreme poverty , inequality , Third world exploitation , wars, etc ) For the medical professionals it is all the more important that growth shouldn’t mean money , as it has a direct and conflicting impact on some one else’s life !
Just Imagine , if the all the car companies combine together , aim for a dramatic growth from the current 4 % to 25 % by 2030 and manage to achieve it by any means ! . . . This planet will sink in the combined weight of automobile Junk !
It is obvious , uncontrolled growth in any form requires vigorous regulation and Intervention and will eventually require a radical surgery if the growth goes unabated !
Counter point
It is foolish to link growing money and wealth equivalent to cancer. Unlike cancer cells , money multiplied can be put into use for those in need .It is the principle of charity .But the reality is , human beings who are rabidly after money rarely have this mind set.In contrary the haven’ts have it in plenty. In my opinion, excess money has a dubious capacity to contaminate human values ! (Why should some rich and elite opposes affordable health care to poor ?)
Let us amass wealth and help others . Microsoft is able to do it. Apple may do it later. What is the need for big companies social responsibility and philanthropy ? If the business worlds motive and end product promotes equality and goodness , sans exploitation , the question of charity at a later date never arises.
Final message
If extreme poverty is a disease , forces that Initiates or sustains poverty cycle can not be a bliss. In this context , the manic affluence (& the urge for it) should be included as a communicable disease since it seems to be most contagious as well.
In health care delivery “affluent and modern care” may also connote a sinister meaning. Poor people might think they are deprived of good care because they cant afford it. But ,truth hides deep. True sustainable caring is little to do with affordability+ , since most of the modern health care expenditure is jacked up with junk.
I know in my country people sell their life time assets for what they think as crucial health care .(Of course universal health care insurance is just beginning to come in. Here again insurance based health care has inflated the actual costs and threatening to impose inappropriate therapies .
As a medical professional we should aim for the cheapest and best form* of treatment to our patients . Artificially inflating the cost of therapy by worthless drugs, devices, procedures and disseminating them invariably leads to pathological growth of science.
*If any one thinks “cheap and quality” doesn’t go together in medical care it is ignorance ! Most problems has simple and effective solution.
Post-amble
* I object this statement -Modern health is nothing to do with affordability.
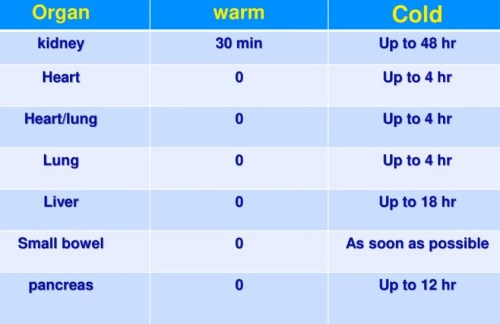
We need to go to the basics then .What is true health ? Forget about transplants, Organ Assists, Five star critical care .They seem to work in a minority , but drain the world economy. Its Impact on global health is at best minuscule. One Important analysis say 90% health care cost is wasted in prolonging the last 30 days of life of homo-sapiens.(Will get the reference for it )
Please note
Diseases that occur to affluent population is entirely different topic . Can be found elsewhere