Background
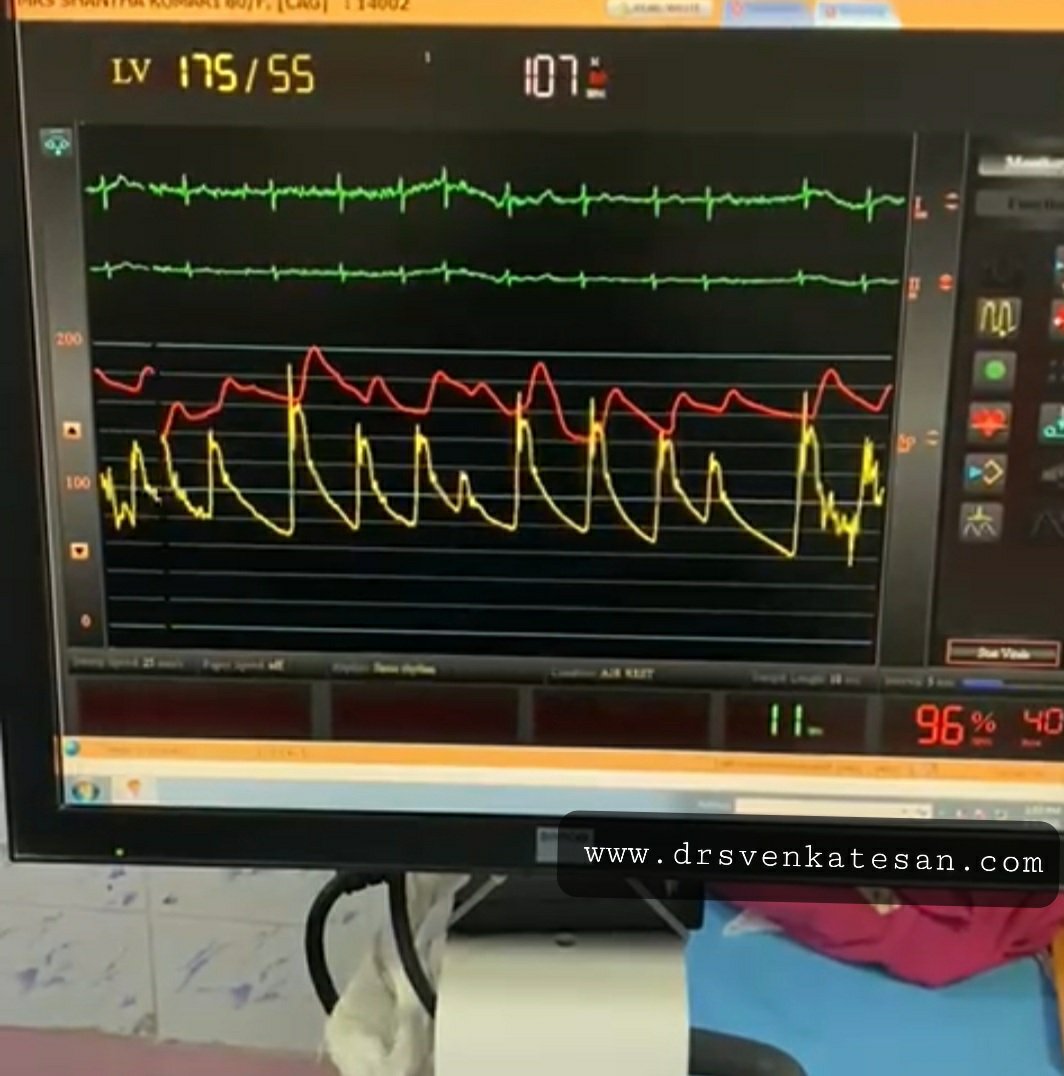
“Your husband is really lucky, his heart attack got spontaneously aborted. His ECG is near normal now. The angiogram is normal.No lysis, no stent is required. He secreted his own TPA and got rid of the clot. We will discharge him to tomorrow.”
Thank you very much, Doctor. How did this happen, doctor?
Don’t thank me. Definitely, I don’t have an answer. Spontaneous successful thrombolysis (Ref 4) happens up to 15 % of ACS. All I can say is he has a very disciplined fibrinolytic system backed up with an agile mast cell and basophil function.
Vascular events: Pathobiology
Vascular highway accidents that happen due to the sudden freezing of blood in any vital organs consume more human lives than any other disease. This can happen with or without a trigger from the vessel wall, the phenomenon which Virchow’s taught us a century ago.
By the way, who is keeping the 5 liters of blood in our body in a fluid status life long?
Blood coagulation and lysis is a fascinating balance of two pairs opposing hematological forces.
- Coagulant system (The 13-factor Intrinsic /extrinsic clotting cascade )
- Anticoagulation system (Antithrombin, protein C and S, and tissue factor pathway inhibitor (TFPI) )
- The fibrinolytic system (Commander in chief is Plasmin, It has the ability to feed and digest clots just like that It comes from plasminogen the activation of this the core concept of thrombolytic or fibrinolytic agents)
- Anti-fibrinolytic system Haemostasis 1986;16:16–20
* Among the blood component cells platelet is the only cell that plays a critical role in the clotting process. Paradoxically the fiery red clot, that is loaded with RBCs has a little direct role in the clotting process while biochemical molecules like fibrinogen, thrombin plays a major role. The fact that blood is liquid forever, tells us a compelling fact, that innate anticoagulation and the fibrinolytic system are more critical than the extensively understood clotting mechanisms.
Are you aware we all have some amount of naturally secreted heparin in blood?
Circulation, Volume XXIII, April 1961
Which cells secrete heparin?
Basophils of blood and mast cells continuously secrete heparin that keep the blood fluid. Heparin is normally present in human plasma in values ranging from 10 to 24 units percent (1 to 2.4 mg. per liter). The range of average values is from 1.53 to 1.77 mg. The native heparin secretion by mast cell population is directly related to the anticoagulation activity (Bill Eksp Biol Med. 1984 Feb;97(2):131-4. Russian. PMID: 6230117.)
Where does TPA come from?
TPA normal levels not only confers the capacity to spontaneously abort a vascular event, but it is also a critical determinant of how streptokinase is going to act as this drug can’t act alone it simple accelerates the action of Tpa complex
Mind you, the basal levels of TPA are injected instantly into the coronary thrombus with a zero-second time window. Now guess what is the potency of this enzyme cascade and who directs it?
Final message
If we think with a hematologic acumen, all vascular accidents are triggered by temporary aberrant behavior of blood or the interaction of its components with the immediate tissue interface. It is the inability to either prevent or fight the sudden occurrence of thrombus that is a primary problem than the tendency of the blood to clot spontaneously. The basal levels of natural Heparin, TPA, or anti thrombins and the way in which they get activated are much more important than the procoagulant forces, which we tend to blame often. (the famous vulnerable plaque vs vulnerable patient need to be reignited)
I think it’s time we dwell deeper into the native lytic mechanisms. This will throw an important vision on how we can replicate it in a pharmacological way. If only we have a drug that melts intravascular clots locally, vascular deaths of many vital organs can be prevented. The research in newer lytic agents has almost ceased & needs fresh Impetus.(TPA is a 25-year-old Invention)
Reference
Postamble
I think we have a problem with our basic science teaching methods. Tried a fact check. When I asked a few passing-out medical graduates, they could rattle everything about clotting factors but struggled to recall any anti-clotting mechanisms. We are still a long way to go, understanding the mysteries of how the blood keeps itself fluid, but always on the alert mode to clot whenever necessary.
DIC: The sine-qua-non of lytic dysfunction
DIC is one of the famous diagnoses in critical care medicine. It is a perfect example of defective fibrinolysis. (Also referred to as acute fibrinolytic shutdown*) classically occurs in septic shock and related conditions. We still lack good criteria to diagnose non-overt DIC-prone patients. A good review was written in 1999, still helps us understand the core concept.
*Both shutdown as well as Inappropriate activation
Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med. 1999;341(8):586–92.