Posted in Cardiology -guidelines, Ethics in Medicine, Social medicine, wisdom in cardiology | Tagged comparative effectiveness, cost effectiveness, cost ineffectiveness, drsvenkatesan, evidence based medicine, health budget of a country, health care indices, health care wastage, health economics, junk science, medical quote best, outcome analysis, quality of health care |
Syncope is one of the common, yet difficult symptoms to evaluate especially in the elderly. Post-prandial syncope is one condition likely to be missed out.As the name suggests It has a distinct relationship with food intake. Mild fall in postprandial BP is an expected response but if it exceeds a limit* syncope is triggered. (*Highly variable)
Hemodynamics of Postprandial state
- Normally splanchnic circulation demands up to a 25% increase in blood volume after a moderately large meal.
- When this happens there must be compensatory vasoconstriction elsewhere especially in muscles. Lack of this response results in inappropriate falls in SVR. (The second mechanism is more constant and can be disproportionate to fall of BP)
- The mediators for this are either neurogenic or hormonal or both.
- Gastrointestinal mediator (Vasoactive Intestinal polypeptide dysregulation) is thought to play a major role.
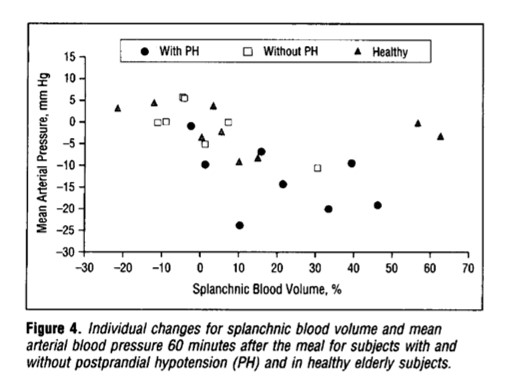
From Jansen et al Archives of Internal medicine 1995
When does it occur?
It can manifest as early as 15 minutes, up to 2 hrs. The fall in systolic BP is around 20mmhg. More common with large, hot meals. The fact that it can occur up to 2 hrs post meals, there is a likelyhood we might overlook it in history.
Other differential diagnoses
- Has a very close two-way link with diabetic patients.(Neuropathic & metabolic ) Postprandial Hypoglycemia-related syncope must be ruled out. (A review)
- Gastrointestinal issues like gastric tumors associated with or without MEN syndrome and insulinoma etc.(Prídavková D, World J Clin Cases. 2020 )
- Two other entities Orthostatic hypotension of the elderly and POTS syndrome are close associates of this condition.
Management
There is no specific therapy. Some of the following might be effective.
- Caffeine,
- Somatostatin,
- Acarbose,( α-Glucosidase Inhibitor )
- Avoiding acute high carbohydrate intake.
- A psychogenic component can be noted in a few that is attenuated by cognitive-behavioral therapy.
- Midoridine, an Alpha¹ receptor stimulant can be surprisingly more effective in some who have overlap with orthostatic hypo (Cleve Clin J Med. 2010 May; 77(5): 298–306.)
Final message
Postprandial hypotension/syncope is a less recognized entity. As always, history is the most important diagnostic tool in the evaluation of syncope, which comes free of cost as well. The diagnostic yield is much greater than sophisticated Holter and event monitors.
Please note, there is a much more prevalent, lesser version of this condition, ie postprandial dizziness or giddiness. However, as already stated there is a significant overlap between orthostatic hypotension and postprandial syncope. It’s worth ruling out diabetes and autonomic dysfunction, (even subclinical Parkinsons) in elders with such symptoms.
Reference
Here is a comprehensive and elegant study (I think, It is only one of that kind on this topic )
Postprandial hypotension Jansen1995
Posted in Cardiology -Clinical signs, Cardiology -Definitions, Cardiology -Hemodynamics, Cardiology -Mechnisms of disease, Syncope | Tagged gastrointestinal cause for syncope, orthostatic vs postprandial hypotension, post prandial hypotension, post-prandial hypotension hypoglycemia, post-prandial syncope, postprandial syncope, vasoactive polypeptide vip in postprandail syncope |
Nearly a century ago, Carl Wiggers helped us understand the dynamics of cardiac cycle with a historical diagram depicting systole and diastole. We know diastole has 4 phases. They are IVRT(nil) early rapid filling,(70%) diastasis,(0-5%) atrial contraction(25%) (Percentage filling within the brackets)
What is mid diastole?
The easiest way to define mid diastole is to divide diastole into three parts with reference to time and call the mid-third as mid-diastole. (.5 seconds/ divided by 3). But, Physiologically we can’t do that. Even hemodynamically there is no distinct mid diastole as diastole is divided into 4 phases as described earlier. When there are 4 parts how can we slice out mid diastole without an overlap?
So, what shall we do? Technically which is the best period to be referred to as mid diastole?
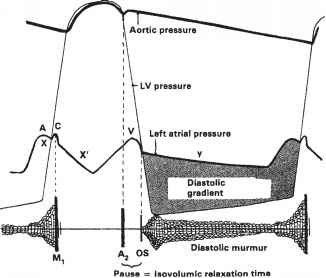
Maybe diastasis. In this period either little or no flow occurs. HR heavily influence the duration of diastasis. Cardiologists especially during auscultation created the concept of calling anything happening after mitral valve opening as mid diastole. ie after IVRT which equals* A2-MV opening interval (In the true sense, it must be the early diastole that can begin with mitral valve opening for physiologists, but for cardiologists, it begins with aortic valve closure because we can hear only closing sounds)
What happens in mitral stenosis?
Any significant obstruction of the mitral valve, the gradient builds up immediately after the mitral valve opens. The murmur gains momentum in the early rapid filling phase of diastole, gradient spills over to fill the diastasis, and finally accelerates in pre-systole to end up in loud S 1.
Is there really an early diastolic murmur in mitral stenosis?
(I can’t agree. We were never taught that way)
Yes for sure. In fact, it can be the dominant murmur in many, since the early rapid filling phase of diastole contributes 70% of filling. In mitral stenosis, the early diastolic gradient will always be present. So. mitral stenosis murmur indeed begins in early diastole and extends further depending upon the severity.
If there is really an EDM in mitral stenosis, why do we still keep calling it MDM?
Just by tradition and for convenience. Auscultatory mid-diastole is different from hemodynamic mid diastole. This irony occurs because murmur descriptions are based not on time but on phases. So, by convention, a murmur that does not occupy the IVRT phase is labeled as MDM. This also helps us to differentiate MDM of mitral stenosis from aortic regurgitation which has the exclusive rights to be called an early diastolic murmur.(Since it occupies the IVRT phase)
Final message
This is probably a too-long post to unmask a trivial nomenclature issue in the diastolic murmur of mitral stenosis. Still, it’s worthwhile to understand this. The word “mid in MDM” is arbitrarily used and doesn’t really reflect either the time or the true hemodynamics. In fact, the same reasoning is applicable for any flow murmur across the mitral valve that is inappropriately referred to as MDM.
Caution
*Let me not confuse the youngsters especially undergraduates. MDM of mitral stenosis will remain as MDM in exam halls. It will never become EDM as that of AR where the murmur starts in the IVRT phase.
For advanced readers
What is the earliest murmur to appear in mitral stenosis?
The first noise comes in the early part of diastole or late presystolic when atria contracts. Never in true mid diastole and gets filled up the in mid part as the disease progresses. So, we can have mitral stenosis without murmur in mid diastole. The morphology of murmur can best be understood when we correlate with Doppler echo profiles.
Is MDM of mitral stenosis crescendo or decresedo or both ?
Normally in diastole crescendo murmurs are uncommon as pressures are falling.( Ventricular contraction only can generate crescendo pressures.) Still, In mitral stenosis, there is minimal crescendo at the onset even when the E velocity decelerates. However, there is a definite presystolic accentuation with atrial contraction which can also be referred to as late diastolic crescendo.
*Is IVRT the same as the A2-OS interval?
It is almost the same but not the same. Find out the difference.
Further reading
Posted in Auscultation, Cardiology - Clinical, Clinical cardiology, Mitral stenosis, Uncategorized | Tagged cardiologist vs physiologist diastole, diastasis murmur, diastolic time intervals, edm in mitral stenosis, ivrt vs at os interval, mdm in mitral stenosis, mdm vs edm ms vs ar, mid diastolic misnomer, murmur of mitral stenosis, phases of diastole |
Further reading
Here is a book from Dr. Ralf Sundberg, a former general and transplant surgeon, a prolific researcher from the prestigious Karolinska Institue, is trying hard to spill some not-so-sweet truths. A must-read, especially for the heavily biased optimistic scientists.
Posted in Uncategorized | Tagged best quote in science, ethics in medicine, venkat quotes |
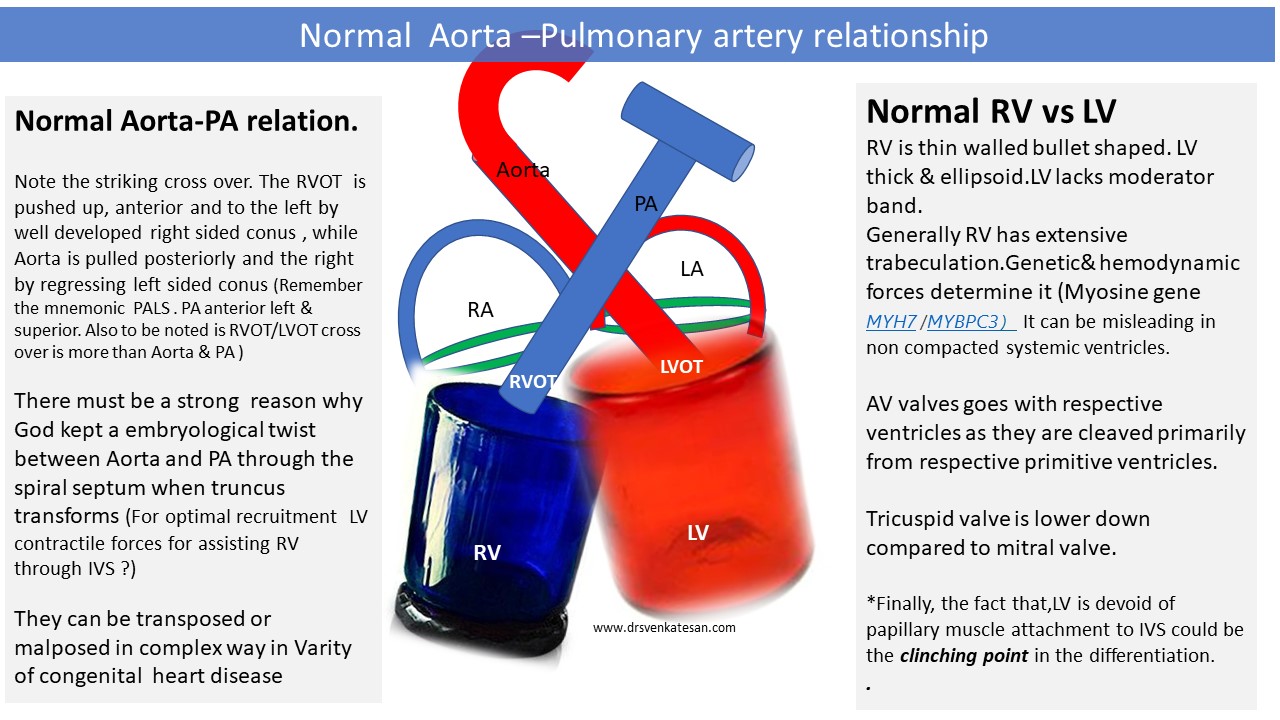
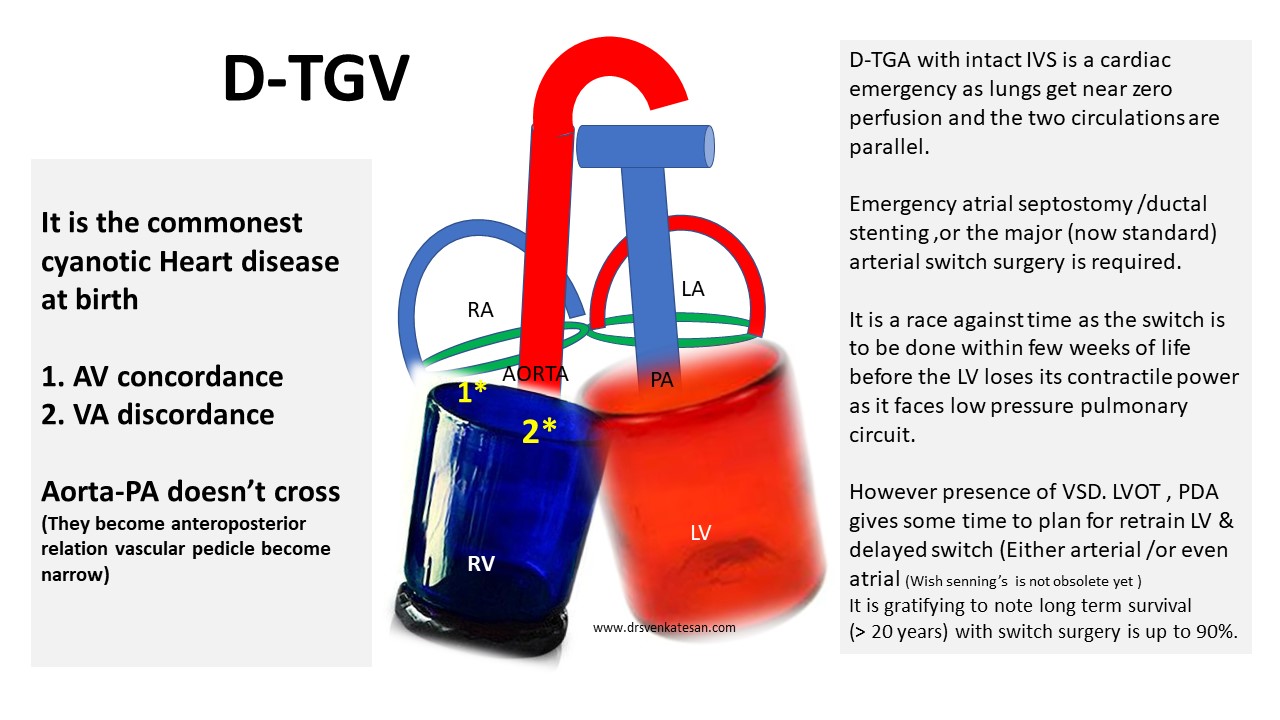
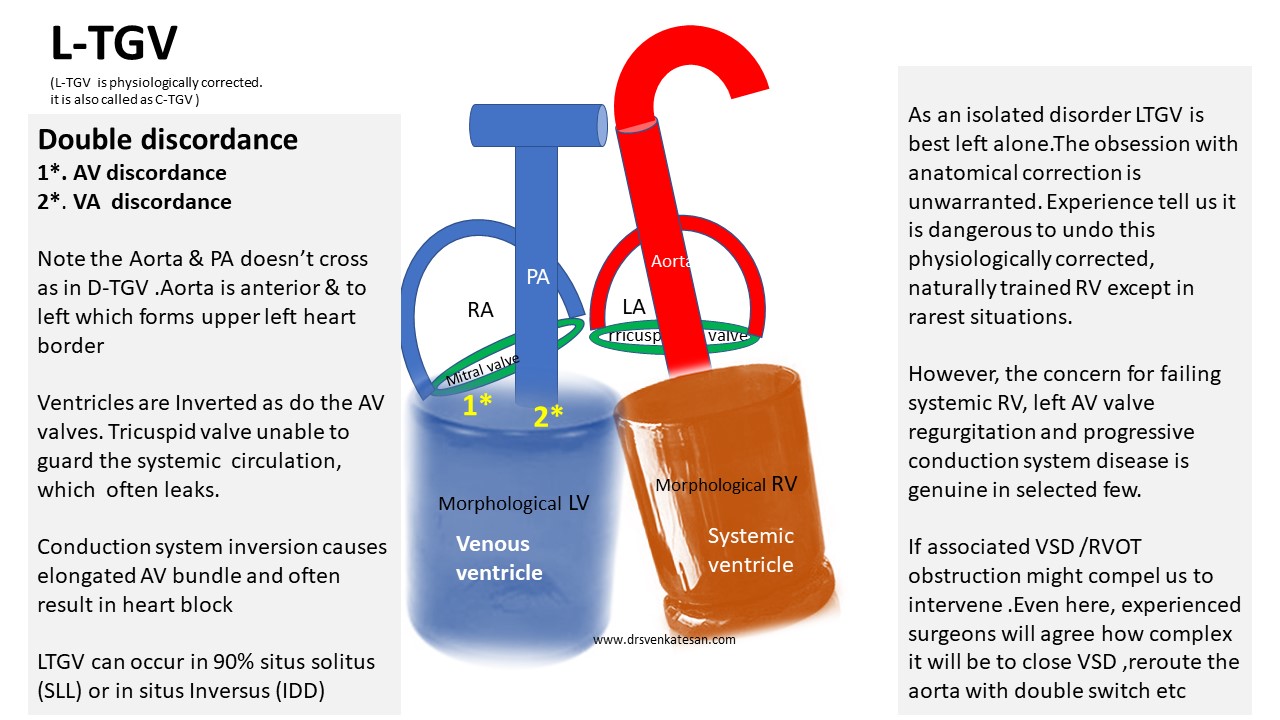
The relationship between Aorta & PA is the key to diagnose many complex congenital heart diseases. Here is a simplified illustration for gross understanding. Please refer to other sources for complete review.
Further reading
Posted in congenital heart disease, Embryology : Heart valve development, embryology of heart, Uncategorized | Tagged accessorry av node, Aorta pulmonary artery relationship, atrial septostomy, double switch surgery, dtgv ltgv ctgv, embryology of heart, left av valve regurgitation, ltgv ctgv in situs inversus LDD, rv lv function in ctgv ltgv, senning surgery, spiral septum, three letter code for chd, ventricular inversion |
Caution: Some language
News
It is heartening to note the apex body that is leading the fight against Covid in India, has responded well. It has either recalled or censured many of the Investigations & drugs, procedures that were used in this pandemic. (Not because they are futile, but they also resulted in a meaningless escalation of cost and possibly worsened the outcome)

So, what?
Beware, “non-scientific mutations” are common in medical research even in ordinary times. It is omnipresent now, and no surprise they end up as a premature evidence base. The consequences of this can be as adverse as the viral variants we fear. The global economic drain of this pandemic is definitely more than what it really deserves. The bulk of resources consumed by Remdesviers, Tociluzumabs, Ivermectins, etc. will easily cross few billions. Further, it is estimated 100s of millions were spent on Indiscriminate diagnostics like CT scans and, Interleukins, D dimers, and even RTPCRs that made a mountain out of a mole. Infinite doses of antibiotics are diligently prescribed for a viral disease knowing fully well it won’t work. One estimate In India says 800 crores worth of Zinc and vitamins were sold over the counter. (The same budget for 1000 bedded state of art hospital!) Heartless marketing. It was painful to watch hard-earned savings was siphoned from not so wealthy & poor for a simple hospital stay.
It must be acknowledged the Government (both state and central) is doing an exemplary job taking care of both private and public health against all odds. However, on a global scale, It is unfortunate many Governments of low GDP countries were politically compelled to spend on flimsy interventions for a self-expiring pandemic. If only these funds are diverted properly, that would help us build permanent health Infrastructure in each of the underdeveloped districts. The only thing, that’s worthy to spend now, is towards the largescale manufacturing of a quality vaccine. Health economists from WHO shall genuinely audit the global expenditure of this pandemic that will help tackle future pandemics better.
(In)conclusion
The virus has decided to play its own game with humanity for whatever reason. The great news is that the vaccine is working. We hope the virus will show enough mercy and leave us shortly. Please follow the required covid hygiene and learn to live in a personal lockdown mode so that countries need not shut down. Meanwhile, a strict embargo on excessive covid related information in the public domain seems as critical as the vaccine. (the demarcation between true knowledge and misinformation is as blurred as one could Imagine)
Postamble
Wishing for a smooth landing with abundant common sense (Image courtesy TIME magazine )
Happy days will be here again soon. But, never forget the harsh lessons taught by this tiny virus .“We must learn to cohabitate on this planet along with other lives peacefully. If we are adamant, God is likely to lose his patience and may not hesitate to discard us permanently “
Posted in Uncategorized |
3D printing technology is growing at a rapid pace. Both cardiologists and cardiac surgeons are expected to benefit a lot.It helps us in understanding deformed anatomy in complex congenital heart disease as well as planning for synthetic cardiac implants.
Currently, the technology is limited only by the chemical material used to print the heart and its components. The American chemical society is working at it to create more realistic heart models. Once we master this, biological printing with synthetic tissue equivalents is the ultimate aim.
Major Indications
- Planning cardiac reconstructive surgeries in congenital heart disease.
- Aortic grafts in Marfan syndrome and other endovascular grafts.
- Valve prototyping
What could be possible in the future?
A dream possibility is that, 3D printing of a patient’s own coronary artery that is diseased with an exact replica that may either act as a surgical graft or deliverable percutaneously.

It is 3D cloning of a coronary artery with a live blood flow experimental setting.(Image clipped from above video)
Final message
It is a merger of biology, chemistry, tissue engineering, and computing. Already it is used in specific conditions.(How about ordering a designer RVOT in severe TOF ?) We are approaching fascinating times in cardiology. Of course, everything would come at a price. We can reap the benefits of this path-breaking progress in science, if and only if, technology is regulated well, Indications are liberally coated with common sense.
Reference
A review article on 3D printing in cardiology Nature review
Posted in Uncategorized | Tagged 3D printing in cardiology, 3d prototyping, evolute r core valve, future of cardiology, sapien valve edwards, tavr mavr |
This 90-second video clip is a “perfect provocation”
Allan Savory is a renowned ecologist from Africa. He is a global leader in environment and eco protection. He is making this famous comment, during one of his interviews from the deep forests of Zimbabwe, after years of ground-level work in the field of desertification and climate change. I can understand his feelings, as we also encounter similar situations at ground zero of the health care delivery system. (I wonder if there is anything called peer-reviewed bedside caring)
We realize wide gaps between academia, patient care, and research are the norm, not an exception. One reason for this is, even well-learned medical professionals find it difficult to comprehend, that the practice of medicine is essentially an art, administered with love, care, service-mindedness. A cost-effective infrastructure with an immense amount of teamwork is critical ( Of course, guided by a fair amount of knowledge, expertise based on good scientific principles)
Final message
As Savory says, let us hope, the future looks bright, that welcomes young researchers from the fringes of the scientific community. Let them be conferred with all courage and resources to course-correct medical science from its frequent aberrant and awkward turns.
Posted in Uncategorized | Tagged art of healing, best book in medicine, cost effectiveness in medicine, definition of medical care, ethics in medicine, evidence based medicine, harrison principles davidson, medical education, medical science is an art or true science, nursing vs medical profession, principles of practice of medicine |
The concept of Fractional flow reserve ( FFR) has dominated the coronary interventional field for over a decade. It gave us a (false) sense of security and pride that we have been advocating physiology-based appropriate stenting.
The much-expected FlOWER-MI trial was presented in ACC & NEJM a week ago. (May 16th Issue 2021)

FFR, though physiologically an attractive concept, has many well-known confounders right from the technical factors, lesion-related errors in physics, mirage of true hyperemia induction with Adenosine, finally & most importantly microvascular dynamism. The value of FFR in the ACS setting was always a suspect. So, no surprises with the FLOWER trial conclusion. It has concluded FFR guided interventions in the non-IRA vessels following STEMI had no use in terms of the hard endpoint. Lesson: We can’t really expect true coronary physiology rules to be alive when severe pathology has set in)
Wait, there can be quixotic ways to Interpret this study be as well.
FLOWER trial reveals the number of stents used with FFR guidance was 50% less (mean 1.01 vs 1.5 stents). Though there was no difference in deaths, the incidence of nonfatal myocardial infarction was more in FFR group 18 (3.1%) than the non-FFR group (1.7% ). Similarly, unplanned hospitalization leading to urgent revascularization was more in FFR (2.6%) than non-FFR (1.9%). Though all were not stat significant, FFR has helped reduce the number of stents in non-culprit lesions. Still, recurrent non-fatal MI and urgent revascularisation were high in the FFR group. So, is it possible FFR related procedural hazards are real? Who can (& how) quantify that? or Is it Inappropriate non-stenting due to FFR misguidance responsible for this trend?
There is one more risk with the potential demise of FFR as a concept. Extreme scientists, might ditch physiology to the backyard and go for free for all stenting again. (Back to shadow physiology & oculocardiac reflex)
Final message
There is an extrapolated lesson to be learned from DEFER*/ FLOWER trial combo. FFR or no FFR, never touch the non-IRA lesions in stable STEMI* however tempting it may be. (*This rule applies even in some unstable STEMIs (Please recall Culprit shock trial )
*DEFER 15 year follow up EHJ 2015 ( Note : DEFER contain significant non ACS population)
Posted in Uncategorized | Tagged FFR FLOWER trial, FFR IFR QFR CT FFR, FLOWER MI |
Next to the atmospheric pressure, the most curious pressure to understand is stored within the human circulatory system. Yes, it is the “blood pressure” fondly referred to as BP by both physicians and patients. (When worried men & women visit us and say, that they are suffering from BP, please make it a point to clarify, BP is a sign of existence of life, rather than a dreaded pathology )
Why should blood have pressure?
BP is lateral pressure exerted by flowing blood on the vessel wall (or is it the propelling pressure head ? It is to be noted, cuff pressure doesn’t measure this !) BP is generated by the heart in systole and sustained by the vascular system in both systole and diastole. BP is measured as mmHg. It can also be expressed as PSI(Pounds /sq Inch) or Pascals or ATMs. If you allow me to spoil with some physics. Pressure is force per unit area ie Newton/m². So, pressure is essentially a force. Force is mass times the acceleration. Mass is weight independent of gravity, while the acceleration of blood is essentially the force of gravity added to the velocity of blood flow. If you think gravitational waves and planetary positions might influence the mass of blood (and hence the BP) you may not be insane. (Environmental & astrological influence of BP and cardiovascular events need not a be mythology) (Oomman A, J Indian Med Assoc. 2003 ) (Robert D Brook Cardiac clinic . 2017)
How is it regulated?
Physics uttered at the bedside is sure to appear as nonsense for practicing physicians. Forget It. BP is not only a continuous variable, the neural, hormonal, cardiac control mechanisms are also in a dynamic flux. What we need to bother is, how to sustain a mean BP of around 90 mmHg within the human circulation, with robust autoregulation. (For the fellows in cardiology, it is a dangerously simplified teaching & belief that cardiac stroke volume determines systolic BP and PVR determines diastolic BP) In fact, It is the systolic pressure that confers the energy required for diastolic BP. Regulation of BP is all about large vessel stiffness, neuro-humoral tone of small vessels, water and sodium metabolism. This makes the kidney a central organ for long-term control of BP. It must also be emphasized BP is regulated in a regional and organ-specific manner. (Ex -The cuff brachial artery pressure may tell little about what is happening at the glomerular perfusion pressure )
Who are the guardians of BP?
Though general Physicians , Neurologists, Nephrologists even Endocrinologsts have more geograhcial rights cardiologists have largely taken siege over the entity of SHT because the heart happens to be a glamorous victim organ. We are witnessing an almost intoxicating number of cardiovascular trials on hypertension, right from Framingham’s days of 1970s to just released BP LLTC in 2021, trying to bring down cardiovascular risk. Based on the accrued evidence, the guardians of human BP in various global institutions bring out strategies to reduce the risk of vascular injury. Have we succeeded in this Intravascular number game.? I think we are. At what cost?
Two repeatedly asked two trivial questions
- What is normal BP & When to start treatment?
- How much lower is best for our body?
Probably, we have got an answer for the first question from this Impactful publication.

I think this study is trying to tell us, there is no normality for blood pressure in terms of risk reduction in cardiovascular disease. (Please recall, one JNC -Joint national committee was dissolved after including a controversial term pre-hypertension in healthy public few years back) What will be the implication for this study? Its core conclusion is about 5 mmHg BP reduction across any subset of adult population will reduce CVD risk considerably. I am sure this study is so intense and powerful it will take at least a decade for its conclusion to fade away. So, can we make these funny conclusions? Hereafter we need not measure BP before starting treatment. Just administer drugs to any live adult who has blood & pressure. (J or U curve need a big debate later)
Mind you, sustained 5mmhg reduction* can be brought by any of the following habits. A salt moderated fruit-rich diet, reasonable physical activity, good sleep, a stroll in the park, yoga, a deep breath, having a pet, watching a movie in a quiet evening, having a loving family, and so on so forth (Of course, 5mg Amlodipine, 40 mg of Telmisartan, or a paradise device can do the same, with an add on pride)
*There is a big catch in this landmark paper. Read the title again. The important take-home point is that this 5mmhg lowering should strictly come by pharmacological means, not by any other means. (Correct me if I am not correct)
Final message
We got the final answer from this marvelously done meta-analysis for the toughest question in cardiology. Hereafter It’s going to be a celebration time for mankind, who struggle in a hypertensive world.
Post-ample
True, sustained high BP is a major risk factor for stroke, heart failure, and CVD. However, it is also true BP can’t* do much damage to the coronary artery without the help from its naughty cousins DM & dyslipidemia. All three parameters must be optimized in unison. May I propose a rough rule? It may be called DFL index for the collective CVD target. Diastolic BP, fasting blood sugar and LDL all should converge around a unitless number of 70 to 80.
*HT is a powerful risk factor for stroke and HFpEF.
Reference
https://www.thelancet.com/action/showPdf?pii=S0140-6736%2821%2900590-0
Posted in Hypertension | Tagged 2013 STEMI AHA ACC Guidelines, blood pressure lowering treatment trialist collaboration, hypertension and dyslipidemia, Hypertension current guidelines, jnc 6 7 8 hypertesnion, Lancet BP LTT trial, LDL vs diastolic BP vs fasting blood sugar, stages of hypertension, V index in cardiology, V index of diabetes, what is normal blood pressure ? |
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- April 2026 (6)
- March 2026 (9)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,648,295 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

