Let me see how many find sense in this Nonsense !

Let me see how many find sense in this Nonsense !
Posted in Uncategorized | Tagged cardiology, definition for interventional cardiology, ethics in cardiology, interventional cardiology, What is Interventional cardiology |
Cath labs are probably the best place to practice preventive cardiology . . .
Practice of medicine is primarily guided by Infinite Information , plenty of Intuition, little bit of Intelligence and unquantifiable amount of Ignorance.The science of coronary reperfusion is standing example for variable mix of the above.The term no reflow is a jargan used liberally in cath labs right from first year fellow to super consultant without knowing what exactly they mean by it.
What really is No-reflow then ?
The academic definition :According to Kloner no-reflow is defined as suboptimal myocardial reperfusion through a part of coronary circulation without angiographic evidence of mechanical vessel obstruction.( Kloner RA, Ganote CE, Jennings RB. “The “no-reflow” phenomenon after temporary coronary occlusion in the dog.” Journal of Clinical Investigation, 1974; 54: 1496–1508.)
With due credits to his seminal paper, I always wonder what exactly Dr Kloner meant when he labelled it as No-reflow!
No is ok , Flow is ok , What does the adjective “re” mean to you ?
Re stands for repeat ? recurrent ? Yes , it may mean any one of it. It may mean nothing in many patients as their post PCI flow is same or found to be no better than pre PCI flow with no significant forward flow at all ! In this situation No-reflow is same as No-flow (Never flown ) in physiological terms irrespective of epicardial patency.
Literally, the term no re-flow tell us, there has been a dramatic procedure related*( or preexisting ) destabilization in distal blood flow. It can be any downgrading of basal TIMI flow. ( Example : TIMI 3 becoming Zero , or TIMI 1 becoming 3 then back to 1 or Zero.) The terms slow flow, low flow, stuttering or trickle of flow all fall under the common category No reflow. In a crude manner one may conclude no reflow to be masquereding term for failed PCI.
*Mind you , No reflow can also occur with pharmacological lysis as well.(Less common)But personal experincee suggest it has a less benign course.
Mechanism of No- reflow
Many mechanisms has been proposed and disposed by experts. However , all suggested mechanisms end up in the final common theme ie micro vascular obstruction.
Can no-reflow precipitate a fresh ACS ?
Could be yes . How ? The distal thrombus migration clogs the active collateral channels at its entry point.This is probably the most unrecognised concept which is difficult to prove though.The problem is , we may not realise this as it could be silent or may just present as LV dysfunction , Infarct extension, or Ischemic cardiac failure.
Why is treatment of no reflow is so dismal ?
I think, by now you can guess the answer and get it right too !
Is no flow better than No-reflow?
It may seem a foolish question one could come across in coronary hemodynamics. The prevailing coronary doctrine, as we understand is , all ATOs need to be opened in STEMI in an emergent fashion. (Other wise patients or their myocardium can’t be salvaged )But, we also realise ATO do get converted to CTOs in a safe manner following a STEMI in a significant number. It’s the ultimate myocardial mystery when we realise even the ATO fails to damage the myocardium significantly in some patients.
Presence of acute collateralisation to IRA from non IRA is observed instantaneously and spreads rapidly towards myocardium in distress.It is observed in atleast 40% of all patients.(Ref 2,3).
The anatomical and physiological codecs of acute collaterals in ACS is secretly located close in the God’s domain.But, Interfering with it, is definitely in human domain.
Should we need to worry about the impact of PCI on these acute collaterals ?
It is estimated up to 5 grams of thrombus could spilled over to the distal coronary bed. Mind you thrombus formation is not a one time process.Can you guess where these thrombus lodge in ? We don’t know what is thrombus clearing capacity of LAD/LCX/RCA vascular bed. But. we have observed naturally formed thrombus is less likely to disseminate and migrate than the catheter and wire induced.My presumption is , coronaries show their dissent and disapproval in the only way they know, ie non stop generation of thrombus (Not withstanding our DAPT/2b 3a /Bivaluridins etc)
Acute collateral shutdown : A new concept

We are not sure if there is a collision between two streams of reperfusion that happens after a STEMI. One spontaneous from the collateral and other from antegrade(Either spontaneous or man made)
Is it benefitial, detrimental or neutral ? We don’t know the answer for sure. My understanding is some of subset of critical STEMI are heavily dependent on this life line however miniscule it may be.
It doesn’t require a double blinded study to prove what would happen when a hurried cardiologist attempt hurried PCI who often has to a change his target to thrombus instead of myocardium .
When aggression is shown on the thrombus, it’s more likely you end up in no reflow . One possible new mechanism(Proposed by the author) of No reflow is distal dissemination of thrombus debri that plugs the lateral entry points of collaterals.
This is the time , no reflow shows its violent face. Invariably hemodynamic deteriation occurs and the entire reperfusion team would seem to count their luck than expertise.
Can we perceive, predict and prevent this ?
We should , we need to , but how ? Since we know the true success rate of no reflow is miniscule, serious introspection to be done. Funnily (but realistically) one can take a famous cue from the most underrated medical specialty Social and preventive medicine .
Yes it’s “Prevention is better than cure” and mind you, if there is no cure, how important prevention becomes.Strangley , preventive cardiology is meant for lesser professionals , who and talk about diet, excercise and lifestyle.
No , it’s not . Preventive medicine needs a new defintion , rather new understanding .Its’ all about preventing an expected or unexpected adverse event anywhere.
How many of us really believe there is no effective cure for No-reflow and it is directly related to aggressive thrombus clearance strategies .
Should we argue new age Interventionists to practice preventive cardiology right inside the cath lab and do away with non-academic temptations.(Surprise , this is exactly mega trials on thrombus aspiration told us (Class 3 Indication for routine thrombus meddling)
Final message
Stable and comfortable, late ATOs need not be opened like defusing a time bomb. We will never know which side of the bomb the cardiologist is sitting.
The incidence of new onset No-reflow can be higher than what we presume.Further it can trigger a fresh ACS by whipping up the injured and resting myocardium.(Mostly attributed to late reperfusion Injury and the acute collateral shutdown.)
Postample and Counterpoint
As an interventional cardiologist, No-reflow is one among the expected complications , which are part of the profession.Never bother about these unscientific utterrings . That’s the job of critics. You go ahead and fight with the coronary artety in every case of ACS. Only weak minded unprofessionals would love to sit on a case of ACS and play a waiting game in CCU. True professionals shall look for multiple criminal targets beyond thrombus, myocardium, IRA , non IRA, doesn’t matter . Do it with confidence.Hope for the best, don’t bother too much about the endpoint.
Mind you, that’s what , we are trained and paid for and possibly respected too in this most glamorous subspecialty of Medicine.
Coming next
*Is Catheter, Guidewire Induced thrombus radically different from natural denovo thrombus ?
*How common is angiographically blind No reflow.(TIMI 3 with good and bad blush included)
*What are the residual defects and long term myocardial sequale ? (Inspite of successful tackling of No reflow )
Reference
1.Claire Bouleti et all The no-reflow phenomenon: State of the art Le no-reflow : état de l’artArchives of Cardiovascular Disease (2015) 108, 661—674
2.L YJ,Masuyama T,Mishima M, et al Effect of pre-reperfusion residual flow on recovery from myocardial stunning: a myocardial contrast echocardiography study. J Am Soc Echocardiogr 2000;13:18–25. doi:10.1016/S0894-7317(00)90038-5
Impact of coronary collaterals on in-hospital and 5-year mortality after ST-elevation myocardial infarction in the contemporary percutaneous coronary intervention era: a prospective observational study
Posted in Uncategorized |
Human body is intertwined collection of lives of Individual organs.We believe death occurs when brain dies , respiration stops and circulation ceases . Curiously ,when life ends , these organs don’t die as a single unit . These three events can happen in any of the six possible permutations.Each organ takes different times to die after loss of life.It is like a crashed computer , where the mother board /RAM memory may be transferred to another and be functional . Out of these three , heart function appears to be supreme as it can function without the need of brain (Science of brain-death) and keep the body alive with intact circulation. Though the concept called heart dead organ donors is catching up as well. (Use and Outcomes of Kidneys from Donation after Circulatory Death Donors in the United States
The science of organ transplant has rapidly evolved .We can transfer an organ from one who is dying or dead to another person who is also dying due to failure of a different organ. Though most organs can be transported and transplanted , we need to maintain life in a dead donor organ . A new and curious specialty in medicine is emerging which could be named a Critical Care of Dead or Critical Cadaveric Care Units !) till harvesting happens. Paradoxically ,after the harvest , the organ gains independent life that has to be sustained.This is where the science of organ transport is waiting in to explode!
How to transport a dead man’s heart ?
There are two Ischemic times in organ donation.
Warm ischemic time refers to the amount of time that an organ remains at body temperature after its blood supply has been stopped or reduced. Cold ischemic time refers to the amount of time that an organ is chilled or cold and not receiving a blood supply. These times quiet vary with respect to different organs.
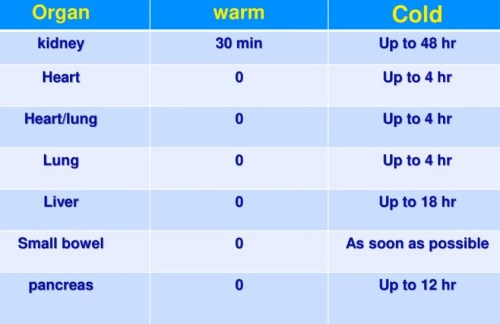
Image source https://slideplayer.com/slide/11955534/
So far, we have been carrying organs in cold boxes with custodial solutions. (HTK*)

This makes the transport time a big limitation of success of the procedure. *HTK -histidine, tryptophan ,a-ketoglutarate, solution
Whats new in organ transplant science ?
Trans medics is an exclusive company , that has pioneered in this unique science of organ transport .They have developed separate organ care system for heart ,lungs and liver.
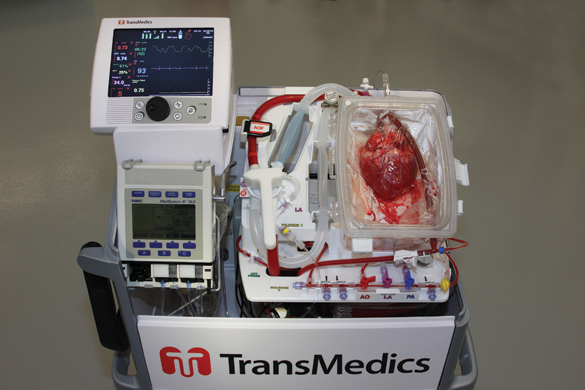
It is the first portable heart perfusion system , which increase the time between the harvest to transplant . It avoids cold ischemic time ,replaced by warm perfusion with metabolic activity monitored till it is transplanted.Ideal far long distance transplant .Soon one can expect trans-continental transplant as well !
This technology could make the difference between warm and cold Ischemic times blurred and in future one may expect to prolong the warm ischemic period and there is near zero cold Ischemic time.
A heart is perfused by transmedics system while being transported
A lung breathing in transit
Final message
Modern medical technology can be seen in action , in so many ways and brings both accolades and agonies in equal proportion. While, even flimsy ones tend to get due attention , Transmedics , probably deserves a grandest reward for uplifting the science of organ donation . I would think this is the most unique service (playing God ) . . . shipping dead man’s organ with assured life on delivery !

Posted in Heart transplantation | Tagged donor heart transport, transmedics | 1 Comment »
A middle aged women , with acute onset left sided chest pain and ECG changes was seen by a general physician. He had little hesitation in labeling the patient as ACS( To be precious he reported the ECG as lateral wall Ischemia) and asked for an echocardiogram to rule out a heart attack (This is how cardiology is practiced in many areas) .

This patient came to my lab for the Echocardiogram .The echo window was poor , It showed a structurally normal heart and there was no pericardial effusion. I suspected something systemically wrong in this patient and asked for a X ray chest .

Subsequent scrutiny of this patient revealed she had moderate left tuberculous effusion. ECG changes are attributed to this. We know pericardial disease can cause ECG changes that mimic ACS. While pericarditis can elevate the ST segment. Can pleuritis without effusion cause ECG changes. What is the demarcation point between pleural from pericardial surface ?
What are the ECG features of pleural effusion ?
Mechanism of T wave inversion in plural effusion.
T wave represents ventricular repolarisation. To be frank I am not able to give an exact mechanism of such defects in pleural effusion.
The following mechanisms are suggested
Teaching points and potential error
To label a left-sided pleuritic pain with ECG changes as ACS can never be considered as a serious error.However , rushing such patients to cath lab or lytic therapy along with heparin leads to more trouble. ER physicians should always keep in mind T wave inversion in isolation is indeed a rare cause* of ischemia. Still, as a physician first , we need to have a check list to rule out common non cardiac conditions. Pneumothorax is one another entity that can exactly mimic a STEMI with ST segment shifts and q waves.It’s also possible left sided pleural effusions produce q waves and mimic an old MI as this case report reveals.(Constatine A Manthous Chest 1993)
I think X-ray chest is least used modality in a coronary care unit for various reasons . Still ,the utility of which can never be undermined and should be used diligently .
*Of course we shouldn’t forget a sinister form of ACS referred to as Wellen’s LAD syndrome which may present with dynamic T inversion.
Reference

Posted in acute coronary syndrome | Tagged Causes of T wave Inversion, ECG changes in pleural effusion, mechanism of ECG changes in pleural effsuion, pleuro pericardial effusion, pleuro pericardial ligamnet, pleuro pericardial rub | Leave a Comment »
The prime job of cardiologists is to restore coronary blood flow in an emergency fashion. While we do this with reasonable success ,there is still a missing link between our Initial aim and achieved goal.
It’s all too common situation in any busy cath lab , to see two similar STEMI patients with identical time window & proximal LAD as IRA , in totally different scenarios. In the first patient we find a trickle of flow in LAD , who is relatively comfortable with normal LV function (In whom , emergency primary PCI might appear redundant.) While the other patient , even after rapidly established TIMI 3 flow , LV wouldn’t look good at all . All our efforts to reperfuse is found wanting. Ultimately LV goes in a downward spiral , ends up in irreversible cardiogenic shock or fatality inspite of Impellas, ECMOs and other LV assist exotica !

I can promise , you can never guess from the angiogram whether this ACS patient was very much comfortable or he is in cardiogenic shock on ventilator unless I reveal the history. Am I right ? That is the mystery of coronary circulation and hence its so critical to serve the myocardium what it wants ? Never treat a coronary artery in isolation !
What is the possible explanation ?
The first trickle (Say TIMI 1 which is usually spontaneous or lytic related ) is the one that’s going keep the muscle viable and possibly prolong the time window for the subsequent reperfusion strategies .Hence it is the timely TIMI 1 or 2 is much more critical than delayed TIMI 3 (Still rapid).
Time window woos :
Who fixed the reperfusion time window as 6 to 12 hours ? Do you know on what basis the acceptable delay of 30 to 60 mts related to primary PCI ? was made acceptable by cardiology community ? If you analyse the published data both are highly contentious and empirical. ( Suggest you scrutiny the data from DANAM2 , PRAGUE and AIR PAMI and come to your own conclusion) (*These are the 3 sacred studies done with few thousand patients that redefined our approach to STEMI and gave the licence to waste the golden hour ! )
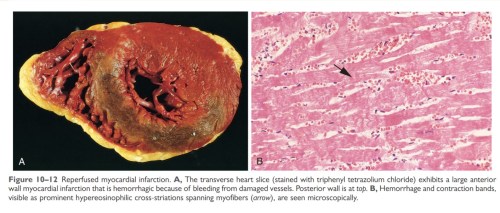
I remember reading the Robins pathology book (Bible of pathology William Boyd as well ) in early days of medical school myocardium may die even within 1 hour with wavy necrosis, contraction bands etc. Looking back some times I wonder how the clinicians have conveniently prolonged time window with whims and fancies of science Intact.
Concurring with the pathologists , we have learnt some harsh lessons inside the cath labs. One of them is that even ultra fast pPCI can fail to salvage myocardium, meaning that time is not the ultimate thing in our race. (There should be other important determinants )
A brief journey back into our pathology classes : Have a look at this table
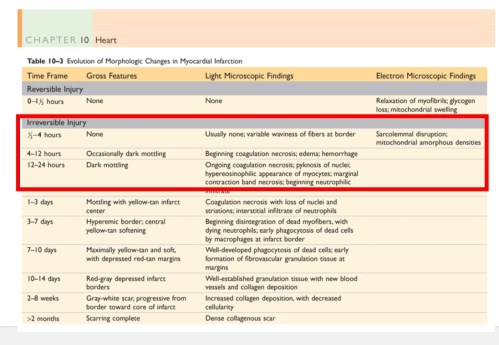
Please note, Irreversible Injury might happen any time after 30 minutes .Of course it can vary . But, the question is how are you going to identify these patients with ultra short time windows? source : Robbins Basic Pathology 9th Edition.Elsevier
Other factors that influence myocardial cell survival
Re-perfusion is not a single edged sword
We may wish the concept of re-perfusion Injury is a myth : Unfortunately it is not ! Myocardium doesn’t relish (not always) the return of circulation in full dose. (May be it’s laying and taking the much needed rest with the initial Injury!)
Sudden gushes of blood leads to extravasation into the interstitium (due to damaged capillaries) increases the Intra myocardial resistance and obstructs the microvascular flow. We have witnessed more than a handful of patients going for cardiac arrest once IRA is opened (of course, we might be able to resuscitate many of them )
Myocardial hypoxia resistance time
Please realise ,true STEMI clock starts not with onset of symptoms but with time of total occlusion.There is more than subtle difference between the two. Onset of total occlusion to symptom time is not a well explored or understood Interval. We take it for granted that the onset of symptoms coincides with total occlusion.
But in multi vessel CAD, even a CTO can cause a STEMI through loss of distal collaterals. Further ,the presence and absence of pre-infarction angina (PIA*) , ischemic pre-conditioning (IPC*) sensitizing effect of remote CAD , manifest vs recruitable collaterals all these make the fixed time windows with which we did our land mark studies of PCI / lysis academically questionable.
* Both PIA IPC are master confounders in the true time window calculations .We don’t know whether its due to ischemia tolerating myocytes or pain tolerating nerve fibres responsible for this varying presentations.But the mystery is certain , when we realise the angiographic spectrum of ACS can range from silent ATOs to painful CTOs
Final message
Is timely reperfusion (and its favorable effect ) lies in God’s domain ? If you we believe myocardial susceptibility , arrhymogenicity and recovery to hypoxia is genetically determined ,then the difference between fate and science Is much narrower than we think .Its appears we can change the former with the later with both positive and negative outcomes. So ,the “f” word may not be a forbidden at-least in the STEMI management. It resides not only within the human genomic codecs written with double-helical nucleic acid fonts . . . but also in the nimble and restless hands of both novice and experienced interventionists !
A study proposal
Let me make a hypothetical statement .A significant subset of patients with STEMI have ultra short myocardial survival and we are unable to identify these hypoxia challenged hearts where primary PCI related delay could be a myocardial sin. Any one willing to prove or disprove this hypothesis ? If some body take this quixotically important study in STEMI management please give me some credit as a contributor !
Posted in Uncategorized |
We learn from basic physiology lessons that human body is made up of 60 % water. What about heart ? There is no reason for the heart should behave differently from rest of the body . If my assumptions are correct when the normal heart weighs 300g , 180g of which should be be water. The same thing could be applicable for LV mass( * Reference requested)
Is there myocardial congestion in cardiac failure ?
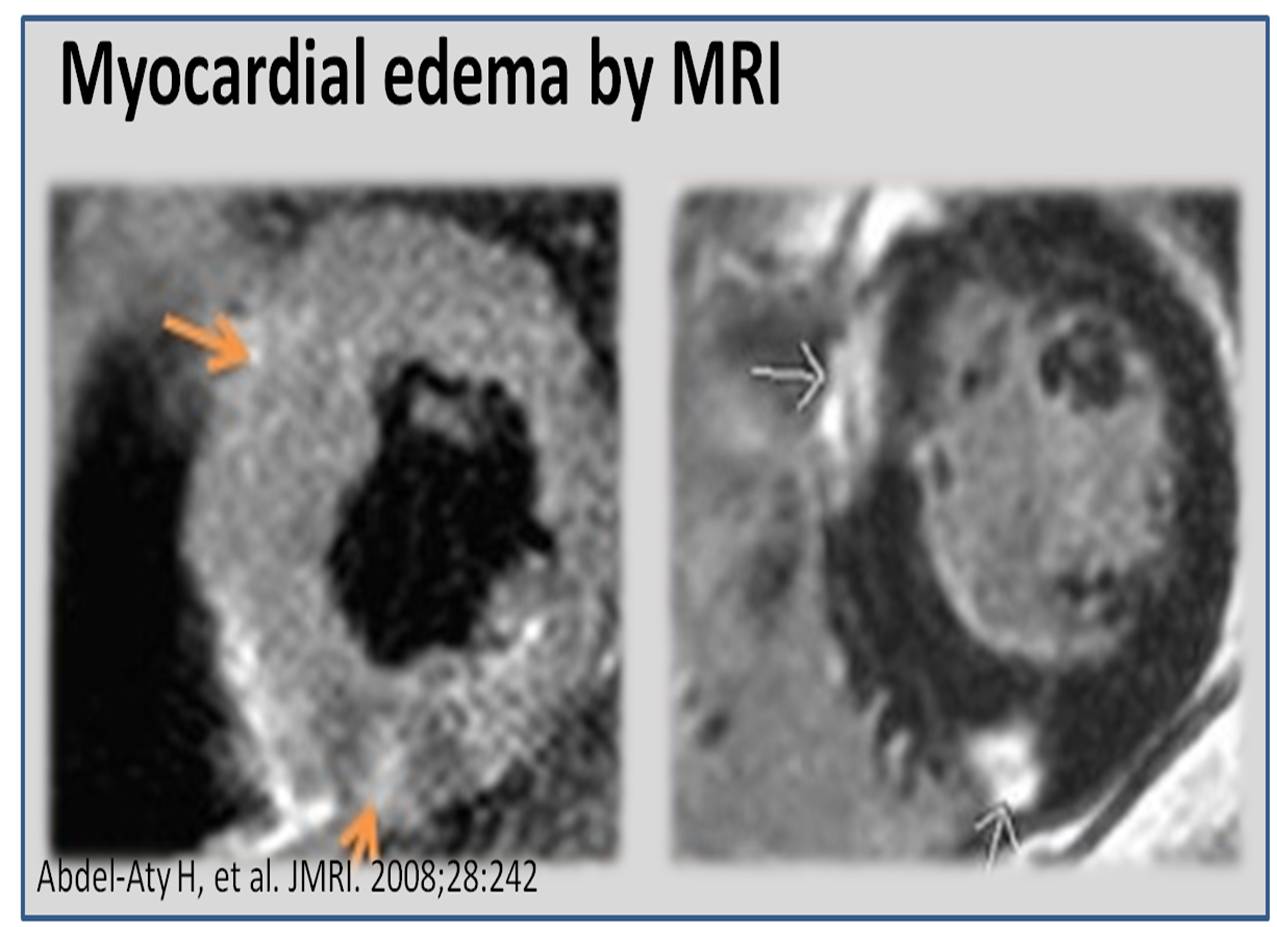
Genesis of edema in any tissue depends on local hydrostatic pressures, tissue resistive forces, osmotic balance, and cell membrane permeability. In the myocardium individual contribution of above factors are not known. Apart from total myocardial water content , myocardial water logging depends upon the trans myocardial venous gradient and the coronary sinus exit pressure in right atrium.Technically ,any severe right heart failure should lead to myocardial congestion at least to some degree.Unlike the lungs , the myocardial edema fluid doesn’t produce crackle , (May cause S -3 gallop instead) . However ,we have modern technology to image water inside the myocardium. Yes, it is called proton / hydrogen imaging or simply called MRI .
This is especially evident In chronic kidney disease , where in the fractional water content within the myocardium is expected to increase further as the whole body is water logged.
We have seen time and again patients with CKD improve in LV function immediately after dialysis . It happens like a magic . The mechanism is simple .The over-hydrated cardiac Interstitium threatening to drown the myocytes is promptly dehydrated by dialysis. This was my wild guess until I came across this paper which proved the exact points.

Other situations where myocardial edema may play a significant clinical Impact (*Includes increased permeability of myocardial capillaries)
Final message
Myocardial interstitial edema in cardiac failure is a grossly under diagnosed entity. A water-logged myocardium is classical at least in CKD. We know it can severely compromise the LV function especially, the diastolic function that explains the all too common flash pulmonary edema in CKD.
The number of studies in this topic (Myocardial Hydrology !) is minuscule compared to other areas of research in cardiology literature.There is a need to involve both Nephrologist and cardiologists to explore this curious concept of dialysable left ventricular mass in CKD/Cardio renal syndromes !

One more area of research
It is reasonable to believe, cardiomegaly in cardiac failure is primarily related to the increased end diastolic volumes .Still , we are not clear whether there is net increase in cardiac mass as the surface area of the heart increases with dilatation. (Even in DCM ? ) Whenever myocardial mass increases relative increase water is likely. Does the beneficial effect of diuretics in cardiac failure , and the restoration of LV dimension is due to myocardial interstitial diuresis as well ?
Reference
Posted in cardiac failure, Cardiac MRI, Cardio Nephrology | Tagged effect of dialysis on myocardial water content, lv amss and myocardial edema, myocardial edema, myocardial edema and ckd chronic kidney failure, myocardial interstitial edema, myocardial water content, myocardial water imaging, water logging in myocardium | Leave a Comment »
Evening cardiac clinic is generally a relaxing place until an occasional patient with vague chest discomfort present with this sort of an ECG .
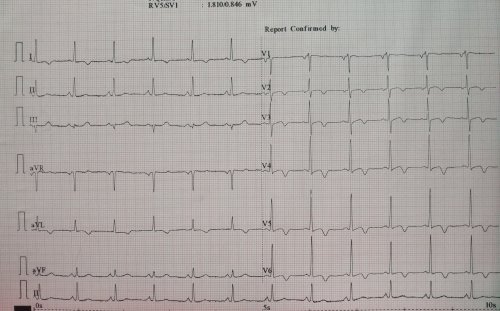
He was a 68 y old hypertensive and was on Tablet Amlodipine .After a cursory look at his ECG , eyes wandered to look for some specifics. Suddenly ,my ECG reading skill was stretched . Is it really LVH ? or Ischemia ? I asked for any old ECG which he couldn’t provide. I had to blink more than a moment , before asking him to describe his chest pain in detail one more time . I got almost convinced it was not ACS since he was having only localized pain over left side of chest. Still , I didn’t have the courage to send him home. An Echo was done.
Curious to know what the Echo showed ?
Yes , you also probably guessed right . It is LVH and there is no wall motion defect either.
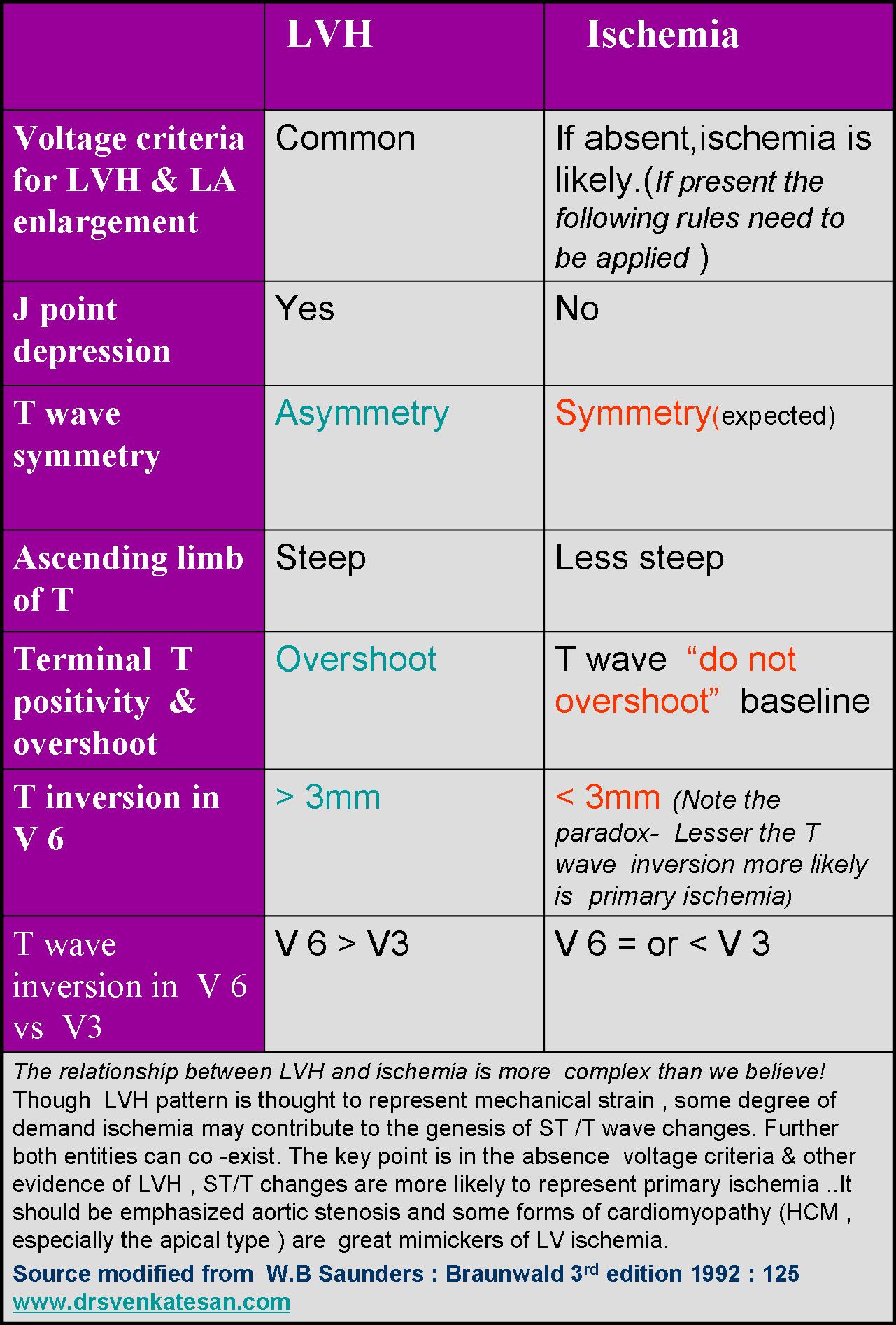
How to differentiate between Ischemia and LVH ?
This is a common question asked in the board exams.There are number of ECG clues to differentiate the two .Mostly it will help fellows to pass exams. Academics rarely comes to your rescue when patients land with chest pain especially at odd hours.
Find the answer in this link
How to differentiate LV strain pattern from primary LV ischemia ?
Now comes the real twister , Does presence of LVH exclude Ischemia in any way ?
Why can’t be ACS in a patient with LVH ?
When I posed these questions , some one suggested global longitudinal strain with speckle tracking to rule out ischemic wall motion defect, my resident suggested high sensitivity Troponin and Ischemia modified albumin.
Whatever is the technological assistance , one thing is certain, we need to finally fall back on patient’s symptoms . Unstable angina is neither an ECG diagnosis nor biochemical or Echo diagnosis . (Its all about patient description about his angina , that clinches the diagnosis !)
It remains a fact normal spot Troponin can never rule out ACS on time ,( Even patients with unstable angina who harbor tight LAD lesion can be both ECG /Enzyme negative )
When we are not sure ,the traditional coronary care dictum shall operate .It demands admit, observe, with serial ECGs and enzymes. This protocol cant’t be followed strictly for a variety of reasons . We may have to rely entirely on our clinical Intuition accrued over the years.
A modern-day cardiologist might have a different dictum .The simplest solution in such situations is a diagnostic radial snap shot coronary angiogram .It is an easy way out . . . , and avoids the trouble of spending wasteful minutes of personal conversation with the patient .The ethics of outsourcing history taking , patient record review or even clinical examination has pushed the definition of professional competence in coronary care into murky grey zone.
One more reason we should hesitate to rush these patient to cath lab is the detection of incidental insignificant CAD (Which will loom larger than life when they are wheeled in from ER) that will lead on to further inappropriate chain of events.
How relevant is clinical acumen in modern era ?
Clinical acumen in medicine can never be taught in class rooms or read in text books. It is the innate ability to combine knowledge, experience ,skill and lastly (and most importantly) courage to ignore conflicting and pervasive data from new generation Investigations. Instead of helping us ,they often directly affect our increasingly vulnerable native medical cognition.
Even if some one is blessed with a good clinical acumen it seems to have little value many times as power of Investigations and fear of missing a event will prevail over it ! I have been victim of this phenomenon many times and not able to follow what my mind preach me !
What happened to this patient ?
I had to admit him against my wish (Of course I was safe!) He too got admitted reluctantly and was observed till morning , spent Rs 5000 for pack of investigations and stay , was discharged without any issues with a diagnosis of simple Hypertension and LVH.
The non academic bug didn’t stop there . . . again contrary to my conscience I had to suggest optional coronary angiogram to rule out true CAD as a precautionary statutory advisory !
Counterpoint
How do you know this is really not CAD ? I won’t believe unless and until I see the CAG and its normal.
Ok, Let me post his angiogram if he decides to undergo it.
Posted in acute coroanry syndrome, acute coronary syndrome, Clinical cardiology | Tagged lvh vs ischemia, primary vs secondary st t changes, triaging chest pain |
We know pleural effusion (hydrothorax) is disproportionately more common on right side in cardiac failure.Though its a well observed phenomenon, the mechanism of which has not been clear to us. It could be due to multiple anatomical , physiological factors.
*The are right and left lymphatic (Thoracic) ducts that drain the corresponding lungs and pleural space . There can be overlap and contribute to the differential occurrence of pleural effusion
Reference
A meticulous paper written some 75 years ago (1946) from Harvard medical school teach us some important points in this phenomenon.

There is still lot, to be understood about pleural effusion in cardiac failure. We need to know why some pleural effusions tend to occur independent of hydrostatic forces. It is also noted long-standing transudative effusions can become true exudates. Role of local pleural capillary hypoxia resulting increasing permeability is underestimated.Hepatic congestion and trans-abdominal seepage of fluid is a distinct possibility.
One more area we are not clear is the relationship between the genesis of pericardial effusion in cardiac failure and concomitant pleural effusion. Post operatively , after univentricular repair (as in Fontan ), pleural effusions can be much problematic with high venous pressure interfering with pleural drainage.
Impact on symptoms
Finally, even mild pleural effusion can increase the work of breathing and result in dyspnea which is out of proportion to cardiac dysfunction.While we expect the diurteics to clear the effusion of cardiac failure, it doesn’t happen always arguing for a non transudative mechanism in at least some of them.
Further reading
Discerned readers are advised to study the pleural space dynamics in detail.
Link to the original Article of Edgar Mcpeak and Levine 1946
Posted in cardaic physiology, cardiac physiology, Cardiology Patho physiology, Clinical cardiology, Infrequently asked questions in cardiology (iFAQs) | Tagged hydrothorax, hydrothorax in cardiac failure, pleural effusion in cardiac failure, right vs left pleural effusion, why is pleural effusion more common on right side |
Though heart is known primarily as a pump, it is the four cardiac valves that ensures the critical , non-stop unidirectional flow that sustain the circulation . It is to be recalled these valves originate in the very early days of cardiac development when the primitive heart tube loops , even as the chambers expand from primitive ventricle. Mesenchymal differentiation controlled by various genes that cleaves the valve from myocardial tissue.
While heart by itself is the supreme vascular organ , its surprising few structures inside the heart , like the valves are quiet avascular ( or is it really so ?)

The valves that beat average of 30 billion time in life time ,seem to get its nourishment from Nowhere ?
Layers of heart valve
Image source : Huk D., Lincoln J. (2017) Oxidative Stress in Cardiac Valve Development. In: Rodriguez-Porcel M., Chade A., Miller J. (eds) Studies on Atherosclerosis. Oxidative Stress in Applied Basic Research and Clinical Practice. Humana Press, Boston, MA
It’s primarily made up of complex stratified connective tissue covered by endothelial cells with intervening interstitial cells. The extracellular matrix (ECM) layers are rich in elastin proteoglycan (spongiosa) and collagen (fibrosa). It has been found myocytes and dormant fibroblasts are scattered in the valve leaflets. This forms the basis of focal origins of Cuspal Ventricular tachycardia J Cardiovasc Electrophysiol. 2002 Jun;13(6):551-6. from electricaly activated myocytes.
Is there a dynamic cell turnover within the valve tissue ? Where does it get the nourishment ? What is the effect of aging and CAD on valve tissue ?
There is growing evidence for valvular extra cellular matrix are indeed dynamic. This explains valvular lesions in connective tissue disorders like Rheumatoid arthritis. Progressive degenerative changes of aging involves remodelling , tissue engineering . Calcification of cardiac valves in endocrine disorders like hyperparathyroid states implies cardiac valvular interstitium is in continuum of systemic metabolic pool. There has been very little published evidence correlating CAD and Ischemic degeneration of valve.
Evidence for vascularity of valves
It is surprising , this simple question of vascular supply to cardiac valves has confronted the scientists for too long.
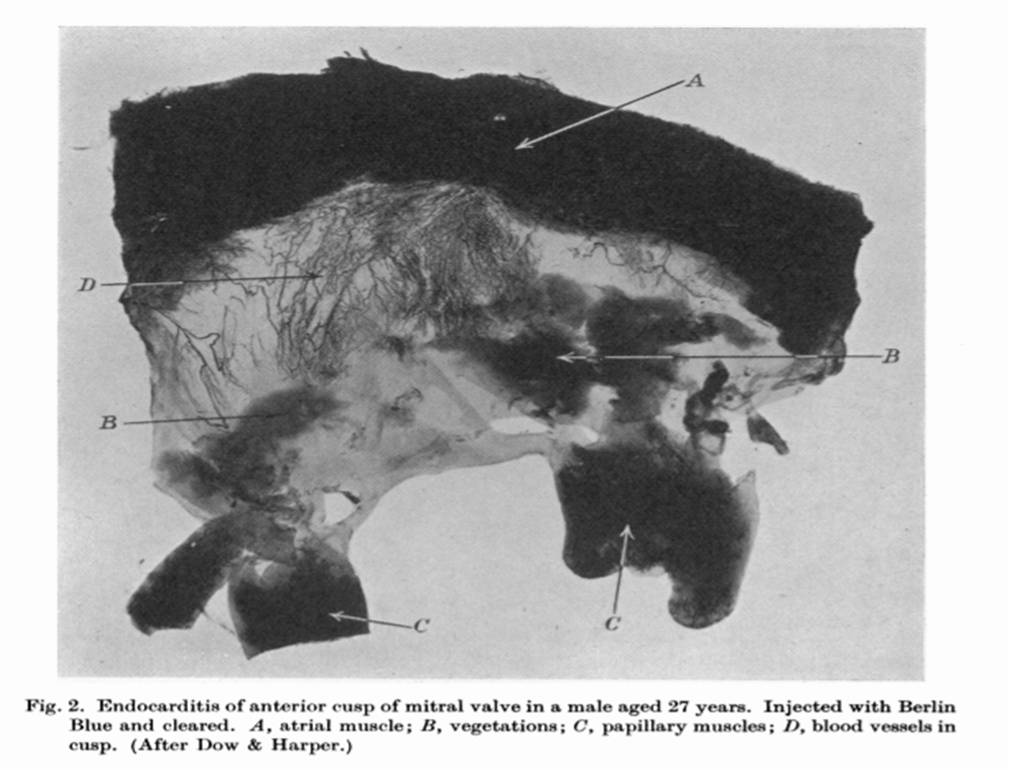
1.Histopathological and autopsy studies have revealed vascular channels.(Harper 1938 BMJ)
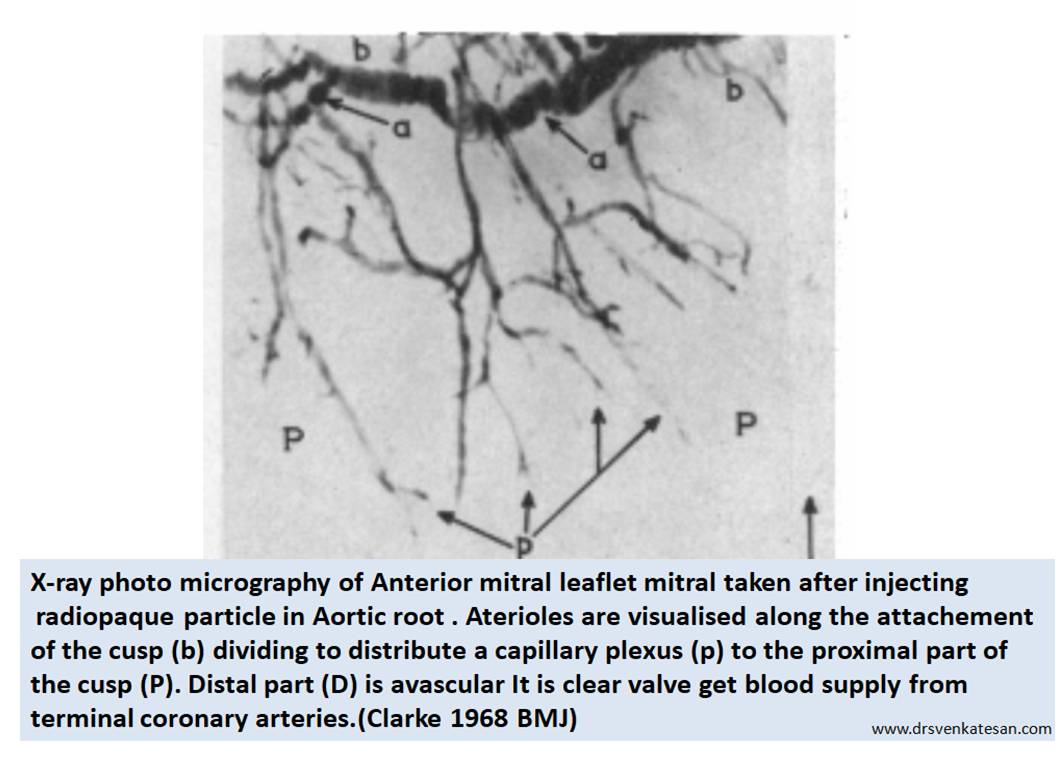
2.X-ray projection microscopy was used to image the valves after injecting radio opaque microparticles in the ascending aorta. This is probably the one of the few original studies done in UK in 1968 (Clarke et al ) it revealed significant vascularity of the valve .It was found 16 % the tricuspid valve, in 10% of the mitral valve, and was maximum in Aortic valve (24%).
3.The fact that statins reach the Aortic valve tissue in lipomatous Aortic stenosis indicate significant vascular port of entry to valves.
Direct evidence : Why don’t we ask the surgeon ?
When I asked my surgical colleagues Does the valve bleed as they cut it ? Most of them were amused with my query , still Iam not sure I got the answer right. At least one of them said since the heart is on pump , it won’t bleed any way !
Conclusive evidence : From a 1968 study
It is academically humiliating to note we have to go back 50 years in time to get a proof for vascularity in cardiac valve.(Or anything new I am missing ? readers may share !) I think , this is strongest proof for valve cusps are supplied by end coronary arteries. However the penetrance is not deep into all layers of the valve and distally
Is hematogenous spread of Infective endocarditis(IE) occur ?
How does systemic infection reach the valves ? We still believe the IE is due to direct colonisation from circulating blood .Hematogenous spread of IE do occur but difficult to prove. It seems infection of valves primarily happen from outside initiated by endothelial injury over the valves .
*There seems to be a contribution from systemic bacteremia reaching from within through the pre-existing capillary twigs as well.(Evidence elusive !)
Final message
Is cardiac valves vascular ? It is curious even in this era , we struggle to answer this query with certainity.
Yes, they are vascular structures , but at best it has partial vascular capillary network. It is also possible the valves can live a durable life even without these vascular Innervation.(I haven’t heard of a condition called mitral valve infarct or necrosis in RCA/LCX STEMI which supply the base of the heart)
Still, this partial vasculaity can become Important at times of pathology like infection or degeneration. Expecting more research in this unique area of valvular heart disease
Reference
1.JOHN A. CLARKE AN X-RAY MICROSCOPIC STUDY OF THE BLOOD SUPPLY TO
THE VALVES OF THE HUMAN HEART BY From the Department of Anatomy, University of Glasgow, Glasgow Brit. Heart J., 1965, 27, 420
2.https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC1252531&blobtype=pdf
Posted in cardiac embryology, Embryology : Heart valve development, Infective endocarditis : Pathology, valvular heart disease | Tagged blood supply to heart valves, hematogenous spread of infective endocarditis, how bacteria reach mitral valve in infective endocarditis, is cardiac valves vascular avascular ?, is mitral valve avascular ?, layers of mitral valve, mitral valve vascularity, three layers of heat valves |
Cardiologist are always worried about the supply side of coronary blood flow. It’s fair enough, we can condone our brain for this one way thinking , afterall arterial supply remain the life-line for the heart. Some of us could (should) realise the importance of these humble coronary veins which are anatomically and physiologically tied together.Its existence is as unique as their arterial counterpart.Coronary blood flow of about 250 ml traverses both the arms every minute.Imagine the scenario if the veins refuse to clear the blood from previous cardiac cycle . . . total hemodynamic chaos right ? Luckily such situations are rare !
See how the the two coronary arteries and its branches interwine with the 4 major coronary veins.

J. M. Bourgery from Atlas of Human Anatomy and Surgery / Atlas d’antomie Humaine et de Chirurgie by Jean Marc Bourgery (1797-1849) Los Angeles: Taschen, 2005. Atlas Case QM 25 .B67 2005
Is the LAD flow coupled with Great cardiac venous flow ?
It is curious to see the LAD hugging its spouse great cardiac vein within the anterior Inter-ventricular groove , but directing the flow exactly in the opposite direction . One should wonder is it the same stream of blood from LAD ?(Near 100% So2) goes out into myocardial tissue comes back with 30 % *saturation in GCV ? If this is true , one can measure the “LAD micro-circulatory bed” integrity by computing the arrival time of levo phase blood in GCV.

J. M. Bourgery from Atlas of Human Anatomy and Surgery / Atlas d’antomie Humaine et de Chirurgie by Jean Marc Bourgery (1797-1849) Los Angeles: Taschen, 2005. Atlas Case QM 25 .B67 2005
* Its an important physiological fact the most desaturated blood(30%) in the body is from coronary veins as the aerobic organ extracts maximum oxygen .(For comparison IVS/SVC saturation is around 75% )
What happens to GCV flow in LAD STEMI ? or CTO ?
In ATOs of LAD there is temporary collapse of GCV. If it prolongs it may end up in complete thrombotic occlusion of GCV which has implication in slow flow , no reflow and poor myocardial salvage.
What happens when there is acute coronary venous occlusion ?
Nothing alarming happens. God’s masterly protection ? Yes it is .Still its a mystery , sudden death is not the rule if we clip the coronary sinus as thebesian venous system take over which drain direct to chambers.The fact that obstruction of these veins may not result in acute coronary syndrome brings less attention to this circulation , in spite of vital hemo dynamic role . Acute venous infarct due to coronary sinus infarction is still possible.
Is there chronic coronary veno occlusive disorder ?
We know ,venous system is Intrinsically prone for thrombosis in susceptible individual as the flow velocity is sluggish . Almost every venous system right from portal, hepatic pulmonary , renal cortical venous , experience this pathology. It’s surprising to note coronary venous system is largely devoid of this.(or at least it’s not recognised as often !)
Some of the patients with chronic CAD with syndrome X /Y show extreme slow flow with normal epicardial coronary arteries.We need to study them for sluggish coronary venous flow syndromes.
Assessment of coronary venous hemodynamics
Coronary venous circulation integrity is critical component of coronary micro -circulation.We have done original studies in the timing of filling of coronary sinus that reflects integrity coronary micro circulation.( Sangareddi V, Alagesan R. Coronary sinus filling and emptying time: A new parameter to assess coronary microcirculation by a simple angiographic frame count. 59th Annual Conference of the Cardiological Society of India December 7–10, 2008. (Abstract).)
Microscopic analysis of coronary venous debris following PCI is our future area of study to assess the mechanisms of no reflow.
Clinical utility of coronary venous circulation
Reference
Coronary venous circulation has an Integral link with micro circulatory bed .It will be of huge importance to understand the highly unpredictable response of PCI with reference to myocardial salvage in STEMI and revascularisation in chronic CAD.Youngsters are encouraged to dwell deeper into the mystery of coronary microcircualtion .
This one from Dr. Muller ,Florida is a perfect review to start with.

A good review about the venous anatomy with reference to electrophysiology

Posted in cardaic physiology, cardiology-Anatomy, coronary sinus anatomy and physiology, coronary sinus filling and emptying time drsvenkatesan, coronary veno occlusive disorder, coronary venous circulation | Tagged acute coronary sinus syndrome, coroanry vein, CORONARY SINUS, coronary sinus occlusion, coronary venous anatomy, venous infarct of heart | Leave a Comment »



