Caring shall be an inbuilt character in the Noble profession ,need not be a value added service or a separate medical specialty !

Caring shall be an inbuilt character in the Noble profession ,need not be a value added service or a separate medical specialty !
Posted in Cardiology quotes, cardiology-ethics | Tagged caring, ethics in medical profession, venkat quotes | Leave a Comment »
When a life leaves the body silently in CCU , an undulating flat line in the monitor has a hidden scientific tale to tell !
A 56 year old obese women died a instant death immediately after engaging the Left main ostium after first injection of 5cc dye. The monitor showed only a short pause, few sinus beats , a long pause , asystole and death . In the last 2 minutes of survival she threw a random wave forms of suggesting EMD . At any point of time she never showed any evidence for ventricular fibrillation . 1o minutes of intense resuscitation failed that included temporary pacing , repeated shocks and ventilation.(ECMO /LV assist excluded)
What is the mechanism of death ?
Post hoc analysis of CAG did not show any significant clues except a tight distal left main.Apparently the catheter has triggered the event .( Or is it the dye ? as some body suggested it as anaphylaxis ?)
Even though we conveyed the message to the relatives, it’s was an unexpected massive heart attack , obviously we were not convinced with our uttering ! Mind you , she had normal LV function but had recurrent angina prior.
Image courtesy modified from http://www.ijaweb.org 2012 for representation purpose only.
We know if cardiac arrest is due to VF, it tends to give us at-least some time and sense. Further,the VF protocols are more clear and success rate is more .
There is always an issue of fine VF vs asystole.If the flat line is indeed VF , there is more chance of revival as we try to pump adrenaline to make the fine VF into coarse one and shock again .The sequence can continue few times.
It is well known asystole has a dismal outcome .Even among the asystole there is some hope* if asystole is purely electrical . (Like Stokes Adams in CHB or electrolytic asystole like hyperkalemia etc ) .But if asystole is due mechanical cause , death ensues in spite of prompt temporary pacing .
* Important note : We have this common form of treatable mechanical asystole .It is called cardiac tamponade .It always present with extreme bardycardia and asystole. It is extremely rare to see a tamponade to present with VF. A prompt needle tap will do the job .It is vital to recognise this in cath lab as our efforts are rewarding .
I would recommend a hand held echo machine , to hang like a catheter in every cath lab , ready to screen unexplained cardiac arrests with zero delay !
Why some hearts respond with VF , while others go for asystole with acute coronary insult ?
Final message
Sudden cardiac deaths 9 out of 10 times is electrical . Majority of them is due to fibrillation. Next comes the electrical asystole ,Rarely (is that really rare ?) an ultra fast sudden death due to mechanical asystole (Non -Tamponade ) is possible , as experienced in our patient .
These mechanical asystole are yet to be decoded.Whether it is a form of Acute stunning , electro -mechanical uncoupling or mechano electrical standstill is not clear.
Posted in Uncategorized | Tagged brady asystolic cardiac arrest, cardiac resuscitation, cpr, electrical vs mechanical sudden cardiac death, electro mechanical deaths, electro mechanical dissociation, emd, suden mechanical death |
Inserting an ICD for DCM may a be great therapeutic success for the physician as well as the patient . But there is one big truth hidden behind the statistical screen.
Following study provides dramatic data from Maanhiem in Germany in about 561 patients who had ICD .The long term patient outcome after appropriate shocks were much worse than those without shocks .This was more pronounced in Ischemic DCM .
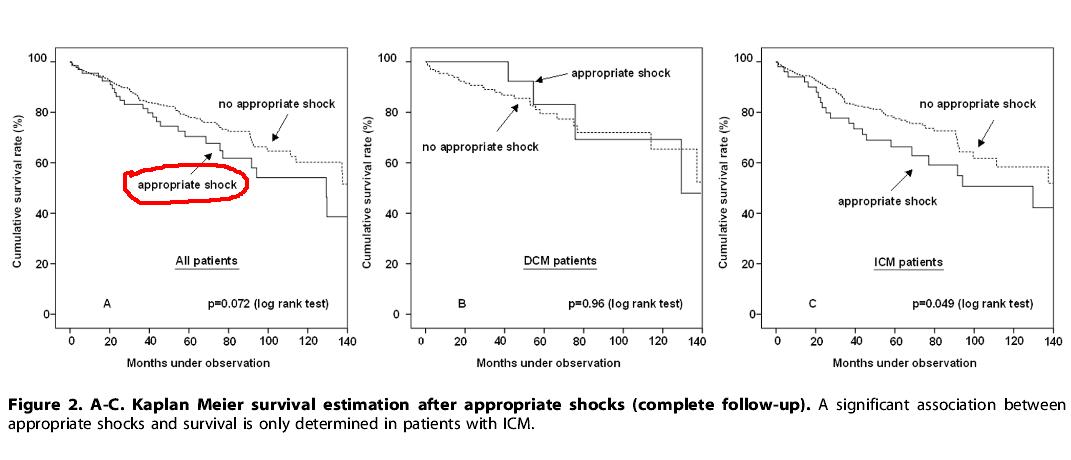
Source : Streitner et al ,University Medical Centre Mannheim, Mannheim, Germany PLoS One. 2013 May 10;8(5):e6391
The fact that these patients continue to throw VT , some thing is wrong in the cellular milieu or a fresh scar / fibrosis / ischemia is progressing .Further , the VTs and the subsequent shocks set in temporary hemodynamic instability .We have evidence , EF can be depressed for days worsening the long-term out come.
While it is easy to blame it on natural course of DCM , there are solid reasons to believe , shock induced myocardial damage is definitely contributing to this excess mortality.
One important clinical tip is to screen all these so called Idiopathic DCM patients who had appropriate shocks. They should be monitored for fresh signs of any systemic illness , like a connective tissue disorder , chronic granulomatous lesions like sarcoid etc .To our surprise some specific myocardial disease may unmask themselves in the natural history. Identifying them may offer a dramatic cure .
Final message
Some where along our EP mind-set we are conditioned to think , as along as there is an ICD in situ and it appropriately shocks, every thing is bliss ! Blame it on semantics . The word “appropriate” inappropriately soothes our nerves.
The fact of the mater is , every appropriate shock is a grim reminder that the heart in question is restless electrically and VT continue to emanate from diseased myocardium . It could mean either the LV is destabilising , or the original disease is progressing or a new disease is evolving .
Mean while, paradoxically , inappropriate shocks give us a quixotic comfort , since the heart is not really throwing any dangerous arrhythmia, after all it is the device related false alarm that could be easily reprogrammed!
Reference

Posted in cardiac resynchronisation, Cardiology - Electrophysiology -Pacemaker, Cardiology -unresolved questions, Dilated cardiomyopathy, Electro physiology, ICD -Tips and Tricks, Infrequently asked questions in cardiology (iFAQs), Land mark articles in cardiology, Pace maker Tips and tricks, Permanent pacemaker | Tagged appropriate and inappropriate shocks post icd, dilated cardiomyopathy, icd in dcm, ICD tips and tricks, ischemic vs non ischemic dcm, myocardial damage following icd shocks, outcome after appropriate shocks | Leave a Comment »
Your clock starts now !

Chronic stable angina : Most can be effectively managed by optimal /intensive medicines and life style Interventions .About 10% will require PCI/CABG.
ACS – STEMI: Primarily managed with rapid and competent pre-hospital care with prompt thrombolysis in or out of hospital .Patients with large STEMI who develop complications (Again about 10 %) require PCI and few additional lives can be saved.
ACS-NSTEMI : This is the group that demand an important role for PCI . All true high risk UA/NSTEMI patients should receive urgent coronary angiogram and critical lesions should either be stented or sent for CABG (If the lesions are multiple and complex ) The field of interventional cardiology is expected to play a major role in this category of patients for the simple reason , we not only give dramatic relief from angina and also prevent a potentially a huge MI that is waiting to happen !
* It is vital to emphasise the “Aim and objective” in NSTEMI management is critically different from other two. We know , in CSA the aim is to give relief symptoms and improve excercise capacity . Both PCI/CABG are unlikely to prevent a future MI in CSA..In STEMI it has already occurred .The aim is to salvage myocardium and prevent future events. While PCI can do the former , it can’t do the later . In STEMI scenerio ,we have very good alternate modality called thrombolysis which can easily beat the pPCI in , cost , availability and time (and hence efficiency as well in most countries !)
Counter thought
The above suggestion is too simplified ,generalized , misleading , and unscientific, should strongly be disagreed. For those people who disagree , I provide an alternate scheme .It is ultra short ,comes in 5 lines .Very practical and scientific too !
In any patient , who is suspected to have either acute or chronic coronary syndromes ,take them to the cath lab in an urgent or semi urgent fashion .Do an angiogram and stent all lesions that you feel important . If stenting is not possible manage with optimal medicines and /or send them to the surgeons.
Final message
The essence of catheter based coronary care is simple.We complicate it. To understand this concept 100’s of cardiology journals and as many conferences and infinite number of books are churned out every year !
Posted in Cardiology -Therapeutic dilemma, cardiology -Therapeutics, Cardiology -unresolved questions | Tagged csa, ethics in cardiology, interventional cardiology, management of pci, pci ptca in a nutshell, priamry pci vs thrombolysis, stemi vs nstemi | 1 Comment »
Current guidelines advice us to wait for 40 days following STEMI to implant ICD in most high risk patients.
Why this cool off period.? *
Final message
So the cool off period is not only to reduce the unnecessary ICD implantation but also to avoid lead related issues .
* This 40 day rule is based on one large study from Germany. (DINAMIT, 2004 ) . However few believe the rule is not absolute. There can be individual exceptions in high risk patients with critical LV dysfunction .
Other wise . . . How do you digest a death occurring on 35th day in a patient who is waiting for an ICD scheduled one week later ?
Reference
Link to ACC/AHA Guidelines for ICD Implantation 2013
New development
How to bridge the 40 day gap in really high risk post MI patient ?
We can’t keep him in CCU. Here comes the role of WCD (Wearable cardiovertor defibrillator.) Life vest is from Zoll . WCD can act like a bridge till the 40 days when the patient becomes eligible for ICD.
Posted in Cardiology - Electrophysiology -Pacemaker, Cardiology -Pacemakers and ICD, Cardiology -Therapeutic dilemma, cardiology -Therapeutics, Cardiology -unresolved questions | Tagged Indication fo ICD | Leave a Comment »
One of oldest hospital in the world , is now an UNICEF heritage site. Santa Creu , Sant Pau original hospital built in 1400 AD rebuilt in 1900 by Catalonian modern architect Montaner.

Architecture by Lluís Domènech i Montaner


 Reference
Reference
Posted in Uncategorized | Tagged heritage hospitals, histroy of medicine, sant pau hospital unicef barcelona | Leave a Comment »
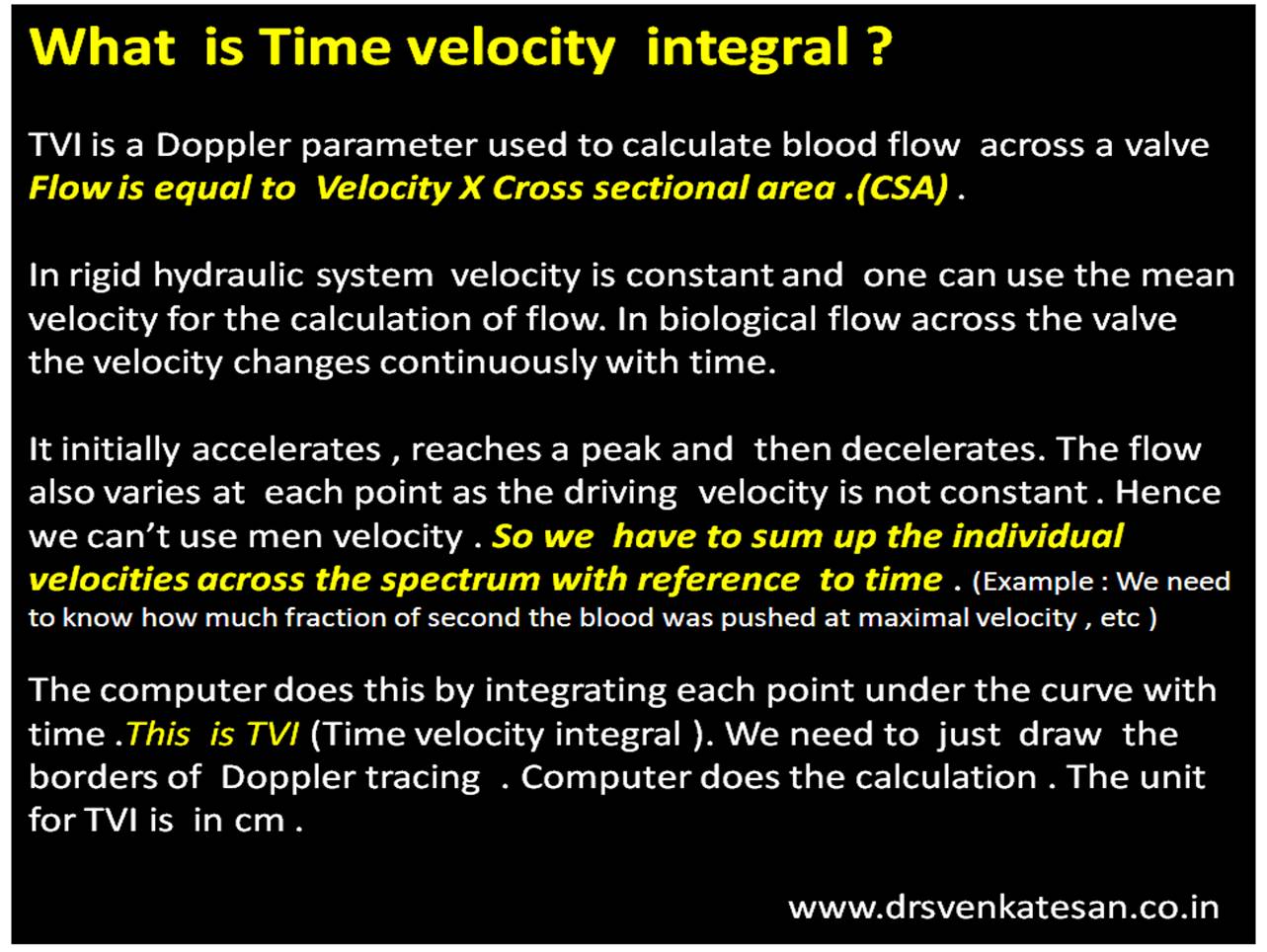
TVI (or VTI) is a hemo-dynamic echo parameter measured from Doppler spectrum across the valves ,usually in the outflow.This parameter is used to calculate cardiac output .VTI times the cross sectional area gives the stroke volume.
A correction: TVI is multiplication of velocity into time not division as suggested in the cartoon
Time velocity Integral
Summary
*VTI is a Doppler parameter described in cm , it can be referred to as Stroke distance.This stroke distance when multiplied by valve area gives the stroke volume from LV/RV (or flow volume across AV valves or through any conduit)
Posted in echocardiography | Tagged tvi, tvi by echo, tvi in doppler, tvi unit is cm, What is the unit for TVI ? Echocardiography, what is time velocity integral |
One of the hottest debate in the recent world cardiology forum in Barcelona WSC 2014 , was about how to tackle incidentally detected non IRA lesions during primary PCI.
So far , the dictum is , one should not meddle the non culprit lesions unless demanded by hemodynamic instabilty .The next option is to do a staged PCI for these lesions. (Few days later). or just forget about these lesions unless they are critical.
Now new studies are appearing that suggest doing all “do-able” lesions must be stented in one go ! This is obviously inviting trouble .The worry is not in the concept but with the dubious track record , fragile guidelines and potential ethical debacle of the cardiology community !
Stent “As you want and as you please” has already invaded our mindset in the chronic coronary scenario. Now in 2014 , we want more freedom in acute coronary syndrome as well ! We can’t ask for a referee less game of soccer !
We clearly know coronary arteries are to be respected and do not deserve indiscriminate stenting especially in ACS where the early hazard is more.
A recent story which I heard was a height of futility . A semi experienced cardiologist in the suburbs of a big southern Indian city , opened successfully a LAD which was the IRA and subsequently caused acute LCX STEMI , while trying to tackle an insignificant non culprit lesion due to procedural mishap ! (Some suggested migration of LAD thrombus !)
What a pity , when we are supposed to arrest the culprit, in reality it is simply chased down to another territory !
Here comes unique advantage of thrombolysis , you need not locate the culprit artery the drug chases it wherever it is , even if they are multiple ! Read in this link :
Final message
We call it as fate when thrombus suddenly occlude a coronary artery and the IRA becomes a culprit . We need not compete with fate and end up creating potential new culprits.Let the sixth sense prevail over the five .Use judicious discretion when trying to stent muti-vessel CAD during PCI. Please realise ,the concept of multivessel stenting during pPCI is not wrong . How we interpret is the issue !
There is no excuse to indulge as you like , simply because your intentions are good !
Posted in Uncategorized | Leave a Comment »
One of my favorite quote about Happiness from Buddha !
Posted in Uncategorized | Tagged happiness quote, happy doctor |
When a patient comes with angina at rest , it could mean two things .Either a STEMI or an NSTEMI .This , we can diagnose only after seeing the ECG .
Can we differentiate these two by the character of chest pain alone ?
Very tough task isn’t ? But there are some definite clues .
Infarct pain
Unstable angina
Mechanism of the difference : Epicardial vs Endocardial angina
The pain of UA is due to subtotal occlusion and endocardial ischemia , while STEMI is sudden total occlusion and the resultant transmural ischemia . In STEMI epicardial surface is always involved (Which lifts the ST segment in ECG .).We know epicardium is same as visceral layer of pericardium which is well innervated .Hence pain of STEMI acquires more of somatic character than a predominately visceral type pain that occurs with UA/NSTEMI where epicardial ischemia is absent.
Clinical importance
The demarcation between unstable angina and Infarct pain becomes vital when we calculate the time window for thrombolysing STEMI .Many of them have a phase of pre infarction angina which is a type of unstable angina. If we mistake it for Infarct pain then one may falsely calculate a prolonged time window and deny re-perfusion therapy.
Post -amble
It is tricky issue to differentiate the chest pain of STEMI and NSTEMI .A significant overlap can occur in real coronary care scenario . We know chest pain that occurs in both pre and post infarct phase is considered as unstable angina .(With infarct pain sandwiched between them!) Hence differentiating them may even be termed as futile.
Still,clinical cardiology can be made fascinating by indulging in such exercise !
Posted in Cardiology - Clinical, Cardiology -Clinical signs, Cardiology -Mechnisms of disease, cardiology- coronary care, Clinical cardiology | Tagged angina vs infarct, difference between stemi and nstemi, epicardial angina vs endocardail angina, heberden angina, how is chest pain different between nstemi and stemi ?, rca vs lad angina | Leave a Comment »



