 Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Congenital heart disease (CHD) still constitute an significant subset in cardiology practice.The moment you ask how do you classify CHD to any cardiologist , the answer would come promptly as “cyanotic and acyanotic CHD “. Such is the power traditional clinical teaching .
There is a fundamental embryological and functional classification available put forth by Clark.It lifts our understanding about congenital heart disease to a different perspective. I wish,every cardiology fellow should know this.
Link to embryological classification of congenital heart disease .
A subset for cono-truncal anomalies is also available.
 Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Posted in cardiology -congenital heart disease | Tagged clark classification of congenital heart disease, classification of cono truncal defects anomaly | Leave a Comment »
No procedure is impossible in medicine . . . but it should be useful for the patient !
Where will you ablate ? What is the purpose ?
The much hyped* ablation of pulmonary vein is never going to help in rheumatic heart since arrhythmia focus occurs at random . How can you locate a focus of AF over a huge , scarred left atrium ? ( which looks like a lunar surface sprinkled with a rocky terrain ! )

Note the huge , scarred LA .It would
be a wild guess to locate the true focus
of AF . (Image source : http://www.e-heart.org)
So , the other option was disconnecting atria electrically . In the past surgeons advocated linear or multiple incisions as in Maze and Corridor procedure after mitral commissurotomy .This helped to a certain extent , still effective , organised atrial contraction was not restored in many.
Now , some electrophysiologists tried to do the same with catheters without much benefit.* Please realise , pulmonary vein ablation even in lone and ischemic AF is struggling with a concept collision !
Can Right atrial focus trigger and sustain AF in RHD ?
Autopsy studies reveal tricuspid valve scarring in 33% of all RHD .Since RHD is a diffuse process , RA lesions can be very well be the focus . It is not an easy task to identify the real culprit focus. So ,concentrating LA for ablation may end up in futility.
There are only few studies available on RF ablation in RHD .This one from Istanbul ,Turkey and it does not favor it as recurrence rate is still significant .

Final message
Approach to AF in RHD : Opening up the mitral valve (or replacing it ) and controlling ventricular rate with beta /calcium blocker along with adequate oral anti-coagulation substantially reduce the risk of embolic events .One may never need to contemplate restoring sinus rhythm in rheumatic atrial fibrillation.
//
Posted in Atrial fibrillation, Cardiology - Electrophysiology -Pacemaker, rheumatic heart disease | Tagged maangement of af, maze corridor surgery in af and rhd, ptmc plus rf ablation of atria, pulmonary vien isolation rheumatic af is useless, rf ablation in rhd, RF ablation in rheumatic mitral stenosis, surgical la ablaton for atria fibrillation, therapeutics in atrial fibrillation | Leave a Comment »
Normal left atrial (LA) volume is about 22ml/sq.meter body surfacearea at all ages.Maximum LA volume in physiology is about 46ml in females and 56 ml in males( Average 35 ml)
LV stroke volume for each beat is about 70 ml . . . so where does the remaining 35ml come from ?
Answer .
- Pulmonary veins ?
- Residual LV end systolic volume ?
- Mix of the two ?
It is logical to assume about 35 ml of fresh blood from 4 pulmonary vein* rushes into LV with every diastolic cycle .It never stays in LA .It just uses LA as a transit route ,
*In diastole the four PVs,LA and LV all act like one single chamber .
Is this reasoning correct ?.
If we believe the continuity equation this explanation is correct . However still what we need to know the fate of residual LV volume (End systolic LV volume which is also about 35 ml that would be in queue for ejection into Aorta for the next beat !)
Further , we know the LV end systolic volume is not constant .During exertion it can reach negligible levels (<10 ml) .At times of vigorous contractions it can touch near zero as well . Then , It become vital for the pulmonary venous reservoir to be act as a major donor for LV blood volume for every ensuing beat.
If the hemodynamics of pulmonary vein LA interface is tricky even in physiology , one can imagine the complexities if the LV diastolic function and left atrial compliance is affected
Debit and credits of LV end -diastolic volume .
Let us assume LVEDV is about 1o5 ml .LA blood volume is roughly one third of LV volume .For every beat equal amounts of fresh blood from pulmonary vein . These two (LA+PV) adds to the residual blood in LV to make LVEDV 105 ml . From this 70 ml is ejected as stroke volume leaving behind 35 ml.

Image template from http://www.cvphysiology.com
Further questions
LA Chamber volume and blood volume need not be same .What I struggle to understand is , total anatomical LA volume measures 35ml , while the amount of blood it is supposed to hold is also about the same .Does it mean the LA is completely filled with blood . . . air tight !
Will the LA compliance make it accommodate twice or thrice the blood volume during exercise ?
What is quantum of residual end diastolic LA volume ?
Reference.(Normal LV and LA volumes )
![]()
Posted in cardiac cycle, cardiac physiology, cardiac volume, Cardiology -Hemodynamics, Cardiology -unresolved questions | Tagged cardiac cycle, componets of LV stroke volume, end systolic lv volume, la volume vs lv volume, relationship between la volume and lv volume | Leave a Comment »
Obesity is a major cardio vascular risk factor.We earnestly believe this by evidence from Framingham and other studies.However , epidemiological truths can be dissociated from individuals .
We now understand some of the obese patients fare better in CHF outcomes apparently because of the obesity ! Even patients who undergo PCI show some benefits.This concept is being proved in large data base of > 200,00 patients.
Possible mechanisms
The lay man’s logic may apply (Science hidden somewhere !) Obese persons have basically a large heart with better cardiac reserve and muscle mass .These hearts are pre-conditioned to extra burden of MVO2 in it’s life time . So it is able to tackle hypoxia better, takes more time to get fully exhausted .After all heart can consume fatty acids for it’s energy requirement.
Adipose tissue may also secrete favorable anti-inflammatory chemicals , though majority of adipocytokines are detrimental except adiponectin .Paradoxically the tumor necrosis factor TNF (Same as cachectin or Interleukin 6) is less in obese patients .
Reference




Reference
The landmark Lancet article that first raised the question of obesity paradox
http://www.ncbi.nlm.nih.gov/pubmed/16920472
http://care.diabetesjournals.org/content/36/Supplement_2/S282.full.pdf+html
Counter to the concept

http://science.howstuffworks.com/life/human-biology/obesity-paradox.htm/printable
Obesity paradox applies in stroke too ! This study (TEMPIS) from Berlin Germany suggest controversially though
Posted in cardiac failure, cardiac physiology | Tagged adipoctokines, adiponectin, Gross obesity, lipids and heart, obesity and tumor necrois factor, obesity paradox, paradox in cardiology, smokers paradox | Leave a Comment »
Pacemaker lead implantation is basically a blind procedure .We are supposed to pace the RV apex . It is akin to anchor a ship in the sea bed. Screwing leads are preferred in permanent pacing ,but tined leads have few unique advantages as well .
Can we combine the advantage of both ?

It is believed displacements are more common with tined leads . May be yes . . . or is it really so ?
It is not the tines or screws that is going to determine the early displacement , rather , it is the expertise , commitment and the time spent during the implantation that matters . I have witnessed equal number of early lead dislodgement in both .
One issue often goes unreported is that , when screwing lead is used operator is subconsciously complacent.While cardiologists who implant tined lead is more cautious , make sure it is well trapped in RV.
Screwing leads.
- Screwing leads should not be positioned in the same place as tine leads.
- This is because , RV apex is rich in trabeculae. Screws can enter one of the trabeculae or it may even enter inter trabecular space. or poke thin trabeculae which may break in near future.(Realise ,how blind we are !)
- Screwing should be done in area where there is least trabeculae ideally in lower end of septum. Since we do it blindly , we can’t be sure where exactly we have screwed .
- Please note , pacing parameters are less reliable than anatomy One may get surprisingly good pacing threshold even in trabecular pacing.
- RV non apical pacing is possible only with screwing leads . However , the superiority of RVOT, para hisian pacing is yet to established in patients with normal LV function (Note 90 % of individuals who require PPM have normal LV function )
Tined leads
- In contrary,tined leads are best placed where there is dense trabeculae.
- It is natural entrapment.
- The expertise of screwing in a best place of RV is not required.
- Whether screwing predispose to septal perforations in long term follow up is not known. Logic would suggest it may ! (The Initial of few mm of IVS tunneling is done by us ! )
- Diaphragmatic twtiching is more common with screwing leads.
- Explantation issues is similar in both .
What does experienced cardiologists say ?
Cardiologists before the era of EPs were using only tined leads without any major hitch . I know electrophysiologists rarely use tined leads now . In our institute , with a cumulative experience of over 3000 pacemakers over 30 years( 99% are with tined leads ) , we have no reason to believe they are vastly superior technique.
However there are few definite Indication for screwing lead
- Abnormal RV anatomy
- Loss of RV trabeculae
- Marked Tricuspid regurgitation
- Pulmonary hypertension
- Second lead in RV
- LTGV
* Note all atrial based pacing are screw based as atria lack trabeculae.
A suggestion

Final message
I would believe ,there is no major difference in both short and long term outcome between these two system of leads.Each has it’s own advantage.
After thought
Why can’t we accrue the benefits of both ? I think we have good scientific reason to request the pacemaker industry to design a lead which can have both tines and screws to provide double safety .Simple isn’t ?
Posted in Cardiology - Electrophysiology -Pacemaker, Cardiology Innovations, Pace maker Tips and tricks | Tagged advantage of tine over screwing lead, anchoring a lead in rv apex, combined tine and screw leads, inter trabecualr screwing, pacemaker lead, rv apex and sea bed, rv pacing lead acute dislodgement, tine vs screw, tips and tricks in pacemaker lead, trabecular screwing of pace amker lead | 2 Comments »
Cardiologists are not single organ specialists . They are supposed to be sincere guardians of the the entire vascular system .Sexual dysfunction in males is almost synonymous with erectile dysfunction(ED) .The male sex organ is equally dynamic organ like the heart . It demands a sudden gush of blood to the tune of 500 ml during complete erection .This conveys an important message . The penile macro and micro vasculature is as important as coronary mIcrovascular bed. Atherosclerois of LAD can be as common as atherosclerosis of pudendal artery .It can precede or follow the coronary lesion. Penile insufficiency is a early marker of endothelial dysfunction. All patients with CAD should be screened for ED and vice versa.
This is not a sexual intrusion in academics , but I am sure , a sustained erection that completes a normal sexual act may very well rule out a proximal LAD lesion 99 % of times .
Do you know , > 7 Mets on a tread mill will rule out a significant left main disease with high degree of accuracy ! Sexual acts require more than that (One may do a study on this !)
There has been some interesting guidelines for managing issue of sexual dysfunction in CAD. .Princeton consensus conference is the famous one.
References



Posted in cardiology -Sexual health, Cardiology -unresolved questions, Infrequently asked questions in cardiology (iFAQs) | Tagged erectile dysfunction in cad, princeton consenus conference 2 3, sexual dysfunction in cardiolgy | Leave a Comment »
While many of us are preoccupied with wires and balloons ,( coronary myopia ! ) , our radiology colleagues are making rapid strides . Let us spend some time to understand how the myocardial segments are inflicted the final insult . We need to realize , there is a pattern to this myocardial end game of scarring and fibrosis.
MRI is the gold standard to assess the myocardial architecture . It has a role in both assessing the anatomy , function , perfusion and viability .

- LV function is assessed by cine MRI
- Viability stud by delayed enhancement MRI (DEMRI , also called as LGE- Late Gadolinum enhancement )
- Myocardial scar best assessed by DEMRI*
* Why do you require DEMRI to identify scar ?
One can detect scars in plain MRI but contrasts make it better .Hence delayed enhancement in by DEMRI is used to detect scars.
Is it ischemic DCM or Non ischemic DCM ? ( That is the question we commonly ask
We rely too much on CAG anatomy for this. It can be misleading. Cine MRI with DEMRI gives the answer straightway with high degree of accuracy . CAG is required in all , but if it is normal , or has insignificant lesions , the dilemma of ischemic DCM would continue !)
**Note ,there is one simple algorithm proposed by the author to differentiate Ischemic DCM from Idiopathic DCM without MRI – Click here to Link
Following scar patterns in DEMRI help us to arrive a diagnosis.
Favors Non ischemic DCM
- Mid myocardial scar
- Epicardial scars
- Global sub-endocardial scars
- No scar(Ironically if no delayed hyper-enhancement is noted it is likely to be non Ischemic DCM )
Favors ischemic DCM
- Regional transmural scars
- Localised sub-endocardial scars
* Ischemic DCM will always involve subendocardium as ischemic wave front goes from sub-endo to epicardium.
examples for Non Ischemic DCM
- Amyloidosis (Can be restrictive as well )
- Chagas
- Fabrys
Why is scar localisation and Quantification important ?
Apart from differentiating various cardiomyopathies it has few clinical implication .
- Since scar indicates irreversible damage , if extensive it will argue against any re-vascularisation .
- Scar location becomes vital if we plan CRT .It will be futile to place a CRT lead over a scar.
- Scars are often form a macro re-entrant circuits for VT .Help us localize or zeroing in VT focus.
- Scar quantification is helpful risk stratification of patients with HOCM .and their family.
Final message
Myocardial scar location and quantification is the new mantra in a patient with dilated heart with cardiac failure.
It may be more important than even a coronary angiogram .MRI will prevail over any of the available echocardiogram modalities to assess the scar pattern.
Reference

Posted in Cardiac MRI, Cardiology -unresolved questions, myocardial disease | Tagged cardiac mri, demri, epicardial scars, how to differentiate ischemic from non ischemic dcm, late gadolinium enhancement, lge gadolinium, mid myocardial scar, myocardial scar Imaging, scar location within myocardium, subendocardial scars | Leave a Comment »
I know ,there is a VSD out there ! but I am unable to get the gradient across it.This situation can be quiet common .The reasons could be technical, anatomical or hemodynamic.
As a rule , if we hear a pan-systolic murmur clinically , one must be able to catch a good Doppler spectrum somewhere by echocardiography . However , If the murmur is restricted to early or mid to late systole, VSD jet is often attenuated in echocardiography .
In the following situations , VSD jets may not record a distinctive Doppler spectra. Invariably the velocity is low , spectrum is short, less intense , lacks good shape and borders are hazy !
- A closing VSD
- A Small muscular VSD
- VSD with Severe pulmonary hypertension
- VSDs with muscle bundle criss crossing
- Double chambered right ventricle (DCRV, where VSD usually drains to high pressure chamber.)
- VSD associated RVOT obsruction (Note: classical TOF VSD will never generate a murmur)
- VSD with sinus of valsalva aneurusms ( Doppler jet can be really difficult to record )
- Inlet VSDs are missed because convectional views of echo are perpendicular to these inlet jets.(Short axis better )
- Another common situation is post STEMI VSR.Both a small apical VSD or multi tract VSD associated with infero posterior STEMI gradients are difficult to obtain.
What is inference ?
Doppler spectrum will help detect small VSDs and color doppler will not miss even a tiny VSD.Doppler spectrum across VSD is dependent many factors other than the presence of VSD. However some large VSDs are detected better by 2D echo rather than doppler signals.
Final message
Presence of a Anatomical VSD does not imply it should generate a noise.The murmur as well as Doppler signals are primarily determined by the pressure difference on either side of VSD. After all , one of the largest VSD that we encounter
Posted in Clinical cardiology, Infrequently asked questions in cardiology (iFAQs) | Tagged doppler in vsd, doppler vsd jet morphology, inlet vsd jet in short axis long axis, late systolic murmur in vsd, mumur vs gradient in doppler vsd, short systolic murmur in vsd, vsd and pah murmur | Leave a Comment »
Syncope in CHB is due to unsafe escape rhythm, changing focus of VPDs, extreme bradycardia, (<20 /minute), pause induced VT, (Usually polymorphic and torsades is quite common .) ultimately may end with convulsions, ventricular fibrillation, and death.
Syncope in SND is due to extreme slowing of SA node . Sinus pauses or even arrest can happen resulting in ventricular standstill. Fortunately, a stable escape rhythm ensues more often than in CHB. (It may just be around 20 or 30/mt. still, ventricular arrhythmias are uncommon. ) This implies an important fact that stability is more important than slowness.Fatality is rare in SND.However, the mechanism of syncope in SND is influenced by the integrity of AV conduction also. If it is severely impaired it can trigger ventricular arrhythmias as well as the escape focus becomes unstable infra hisian location.
Paradoxically, in patients with SND, an episode of palpitation due to AF or sinus tachycardia precedes the episode of syncope. An intelligent patient may recognize this as a warning and can take lying posture after runs of palpitation.This is because of tachycardia-induced suppression of SA node prolong the sinus node recovery time still further.
How to differentiate cardiac syncope from simple vasovagal syncope?
Cardiac syncope is differentiated by common vaso-vagal syncope (VVS) as the latter occurs during erect posture . It may be entirely due to vascular component and hence it may simply represent hypotension without a true cardiac limb .(Vasodepressor syncope)
Hence the pulse rate and volume may take some time to recover in VVS, while Stokes Admas of CHB usually have a well-formed bounding pulse in the recovery phase, as the rate is low and systemic hypoxia is a consistent feature.
How is the respiration during Stokes – Adams syndrome ?
Intact. Oxygenation in the lungs goes on for time being. The pooled pulmonary blood gushes after the termination of syncope and causes the classical flushing. Since the hypoxia causes systemic vasodilatation the flushing is more obvious.(Unlike vasovagal syncope where they are often pale)
History of stokes Adam’s syndrome Morgagni is the one who gave credit to their discovery
Though Morgagni first described the clinical picture of this syndrome in 1761, It was published much later by Two Irish Physicians Stokes, Adams. Wish this entity is referred to as Morgagni-Stokes-Adam’s syndrome
Reference
2.W. Stokes. Observations on some cases of permanently slow pulse. Dublin Quarterly Journal of Medical Science, 1846, 2: 73–85
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -Therapeutics, Cardiology -unresolved questions, Syncope | Tagged cardiac syncope, mechanism of syncope in chb, mechansim of stokes admas syndrome, sick sinus syndrome, sinus node dysfunction, stokes adams morgagni, stokes adams syndrome, stokes admas attack | Leave a Comment »
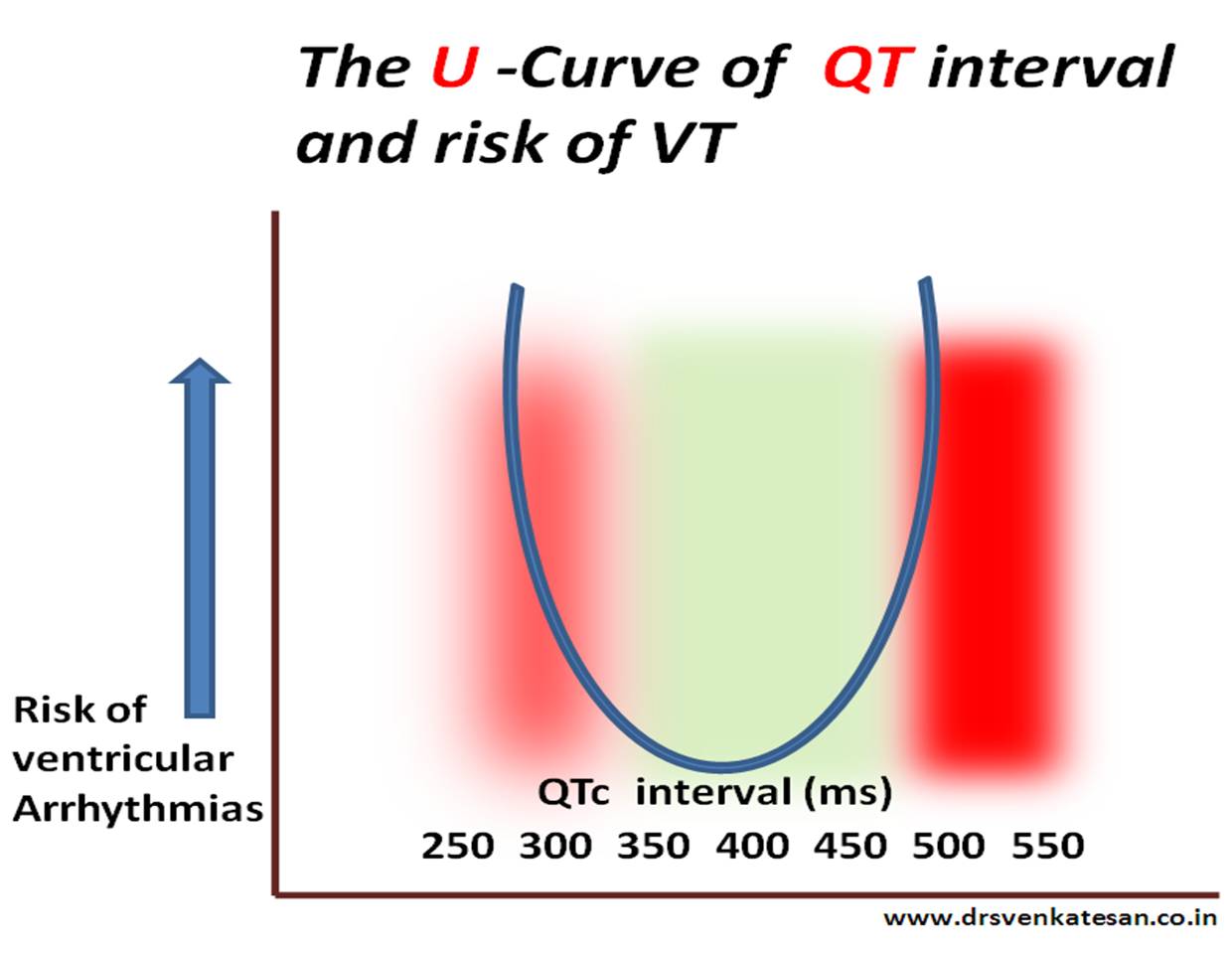
The stretch and strain experienced by the action potential’s left shoulder region is almost similar* in both long and short QT syndromes that trigger a VT.(* Hope this explanation makes some electrical sense !)
*Click over the image for high resolution
What is short QT interval ?
It is a range . Any thing less than 380 ms can be considered short.Generally It becomes important only at < 320ms.
Relationship between QTc and risk of VT .
Posted in Cardiology - Electrophysiology -Pacemaker, Infrequently asked questions in cardiology (iFAQs), Long and Short QT syndromes | Tagged how short qt syndrome induce vt, long and short qt syndromes, Mechansim of VT in long and short QT syndrome, short qt syndrome | Leave a Comment »
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- June 2026 (7)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,690,319 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

