Answer :
In cardiogenic shock it is A . In all others it is probably C.
While D may be considered as an essential target criteria for completing the rescue PCI
Read also
Why-we-often-follow-a-reckless-time-window-for-rescue-angioplasty ?
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, Cardiology-Coronary artery disese, tagged rescue angioplasty, rescue pci, time window for rescue angioplasty, waht is the time window for rescue angioplasty on March 31, 2013| Leave a Comment »
Answer :
In cardiogenic shock it is A . In all others it is probably C.
While D may be considered as an essential target criteria for completing the rescue PCI
Read also
Why-we-often-follow-a-reckless-time-window-for-rescue-angioplasty ?
Posted in cardiology -Therapeutics, Cardiology hypertension, cardiology- coronary care, Cardiology-Coronary artery disese, tagged after load -preload mismatch, afterload mismatch, lvedp and ef in lvf, mechansim of lvf in hypertension, waht happens to ejection fraction in hypertensive lvf ? on March 31, 2013| Leave a Comment »
Answer
The tie is between “B” and “D ”
We know in hypertensive hearts LV primarily fails in diastole . Lungs get congested due to raised LVEDP .Here is a catch . . . if diastole is terribly dysfunctional how can be systole be near normal ? (After all . . . systole is not a distant cousin of diastole !)
How is that high blood pressure maintained in spite of LV failure* ?
Is it due to well-preserved EF and cardiac Index ? or Is it due to extreme levels of peripheral sympathetic activity mediated by catecholamine surge triggered by LVF.
We have attempted to measure LVEF in patients with flash pulmonary edema and acute severe hypertension .It was a real messy echocardiography . We could not conclude much but one thing is clear in acute hypertensive LVF the LV was vigorously contracting in , probably making the option D more correct .
* The other way of reasoning is . . . it is because of high blood pressure the LVF has occurred . LV contractility has no contribution in maintaining the high BP ( Not in line with the age old concept of LV contractility a major determinant of systolic blood pressure !)
(Having said that . . . we also see patients with severe LV dysfunction with severely stunned , ventricles in association with hypertension and LVF . In fact many of the reversible DCMs are due to sudden surge in blood pressure )
Other mechansims of LVF and lung congestion is
Postamble
If this article has confused you a little , It has achieved one of it’s objective . ! I expect more from young cardiology fellows to address the issue !
Reference
This NEJM article authored by Sanjay Gandhi has almost answered the hemodynamics of acute LVF and HT .

Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, tagged concepts in primary pci, ethics in cath lab, indication for rescue angioplasty, rescue angioplasty, salvaging myocardium, time window for rescue angioplasty on March 28, 2013| Leave a Comment »
Myocardial salvage is like coronary fire fighting.When fire is fought very early after the accident , benefits are accrued more . Text book primary angioplasty is . . . fire engine arriving at the scene when the house is on fire .
Rescue angioplasty is asking for more force , when the initial fire fighting was inefficient to control the fire. So , it is obvious the rescue efforts should be fast and brisk.In fact the pace should me more than the primary (The the second engine should reach the ground zero faster than the first ! – Read as door -balloon time ! )
But what happens in real world ? We would tell time window for primary angioplasty even in sleep ! but will struggle to come with clear cut answer for the same in rescue angioplasty even in a fully awake state !
It is an overwhelming fact , we have not taken enough efforts to define strict time limit for rescue .( Even though guidelines say it should not be beyond 24 hours , common sense will tell us rescue PCI should not go beyond 12-15 hour window ! .One more definition for rescue PCI could be within 3 hours after diagnosing failed thrombolysis. In real world it is a race against time in a different perspective .In many centers rescue angioplasty “enjoys time less windows “
I was funny witness in a big private hospital when a colleague of mine has posted a case for “elective rescue angioplasty” and was waiting in the side cabin for his turn !
Coming back to the title question
Why we often follow a reckless time window for rescue Angioplasty ?
The reason is simple
Time is not only muscle . . . time is money too !
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, critical care ccu, tagged 90mmhg and ntg infusion, balanced vasodilatation with inotropic support, ischemic lvf and ntg infusion, iv nitroglycerine in acute pulmonary edema and shock, nitroglycerine, shock and vasodilators on March 25, 2013| Leave a Comment »
An elderly man with past H/o CAD was admitted with ischemic LVF and hypotension .Blood pressure was 90/60 mmhg and pulse rate was 140 . Urine urine output in the immediate past hour was 50 ml . Saturation was 95 % .He had fairly extensive crackles in both lung fields.
A bed side echo showed moderate LV dysfunction , with wall motion defect in LCX territory and mild MR .A dignosis of post MI -ischemic LVF was made .
He was put on intensive anti failure protocol. I asked my fellow to administer IV NTG and left the ward .
On my next visit after few hours . . . the patient was in much bad shape , and when I enquired , I learnt NTG was never administered . I was curious to know why the fellow dis- obeyed my instruction .
He felt sorry . . . But he earnestly told me , he could not comprehend the principle of administering NTG in a patient with shock ! . I was happy to note his genuine concern for the patient ! But . . . I had to take a brief lecture to convince the importance of NTG in some forms of shock !
What is the cause for hypotension in ischemic LVF ?
Lungs are flooded due to very high LVEDP . Blood not only struggles to enter the LV but also finds difficult to leave the LV , former due to defective relaxation later due to poor pumping.
The extremely high pre-load actually stuns the left ventricle in diastole . (Primarily diastolic stunning ) . Here is a hemodynamic paradox . Excess pre-load occurs in terms of pressure , but in terms of volume there is miniscule amount blood that traverses LV .
This is pre-load mismatch at play .Empty ventricles with high wall stress and that is reflected in aortic afterword as well .
We have to some how reduce the very high levels of LVEDP . IV NTG can dramatically reduce the pre load ( and reduce the LVEDP .) The other major benefit is , NTG can reduce the MVO2 by improving sub endocardium coronary perfusion and de-stress the heart.
Once LVEDP is lowered , the ventricle will tend to recover and gain at least some original elasticity ( Frank starling forces) . Of course it will be defective due to ongoing ischemia . Even slight fall of LVEDP (say from 25 to 18 mmhg can have significant benefits as the LV function curve labors on the steep shoulder region !) .
This is one situation where NTG can increase the blood pressure once the hemodynamics is favorably altered.
*Yes . . . heavy doses of Frusemide injection can do the same job but it largely depends the kindey’s cooperation to flush out fluids .In a shock like situation one can trust the kidney perfusion !
Additional benefits of NTG
Mitral regurgitation is a serious destabilizer of LV function .NTG can reduce the regurgitant fraction in acute MR effectively .
Caution
NTG may worsen the hypotension of RV infarction . Make it very sure , you are not dealing with this unique pre-load dependent circulation.
What happened to this patient ?
He did show improvement with IV NTG . Of course it was not dramatic as I have projected in this article .Still it was really helped him .He required simultaneous dobutamine infusion as well .The BP did not fall further and lung congestion was relieved .He went on to recover fully by 48 hours and was posted for elective cath study .
Final message
We tend to worry more about falling blood pressure when administering NTG. . .It is a wonderfully effective drug especially in the setting of ischemia and cardiac failure even if the blood pressure is low !
Acute cardiac hemodynamics is complex phenomenon .No one has mastered it .Paradoxes are common . Hypotension in the back ground of acute pulmonary edema especially due to ischemic LVF can be corrected by NTG . Of course physicians need some courage to administer NTG in patients with a systolic pressure of 80-90mmhg.
This should ideally be done with intra arterial line in place and a simultaneous inotropic line (Doubtamine /Nor-epinephrine ) back up in case of worsening perfusion pressure .
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology- coronary care, cardiology-ethics, tagged commercial guidelines for stemi, etical guidelines for stemi, guidelines for stemi, primary pci thrombolysis on March 24, 2013| 1 Comment »
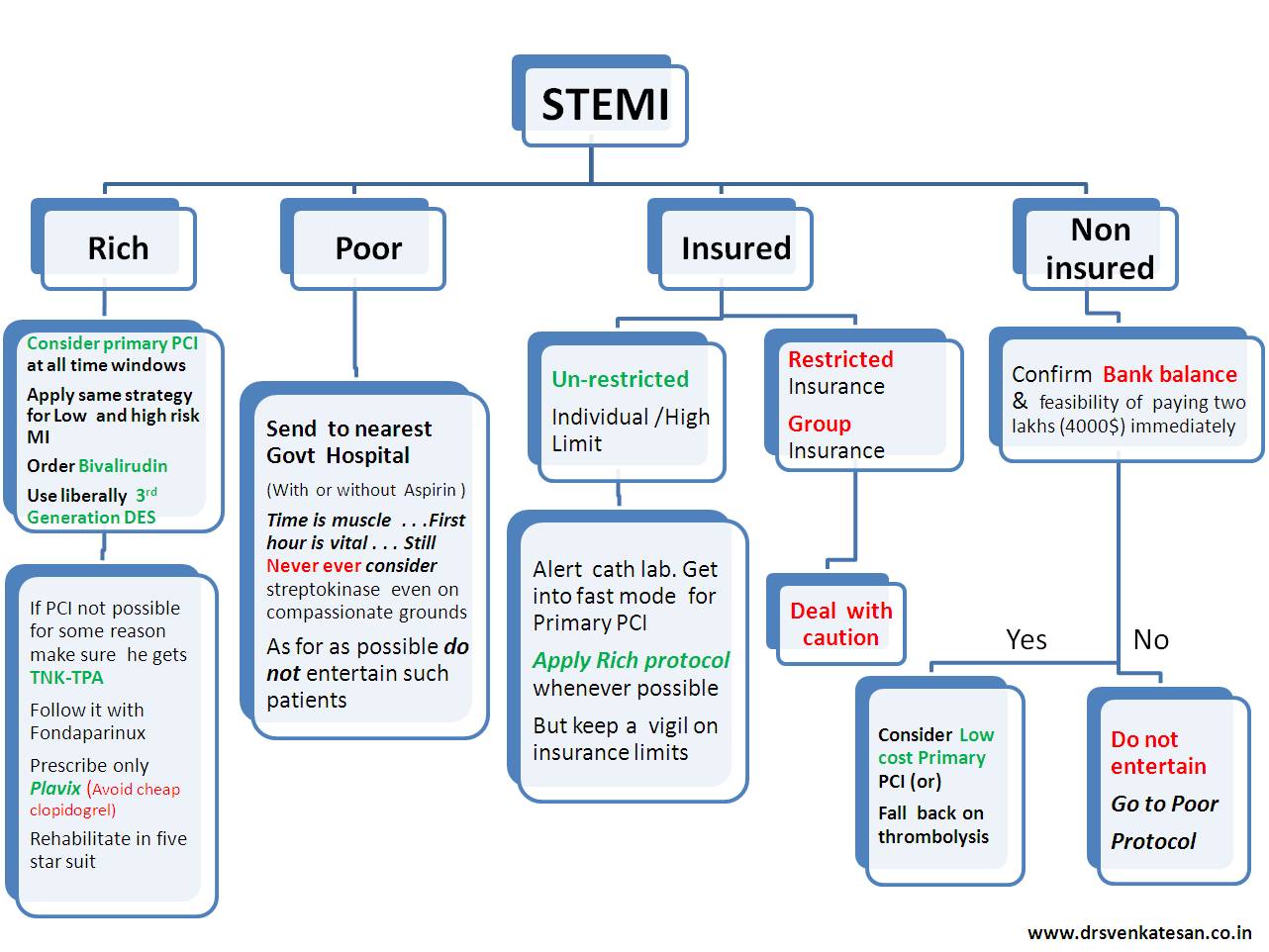
Acute MI kills a few million people world-wide every year .It does not differentiate rich from poor. Logic would tell us , principles of management should not differentiate the people when dealing with a myocardium in distress .
Unfortunately , we scientists do it with passion !
The problem is enormous . . . the rich is suffering from too much* care and the poor is suffering from want of care !
The following flow chart is a result of my observation from close quarters about the management strategies in corporate as well as Govt hospitals .
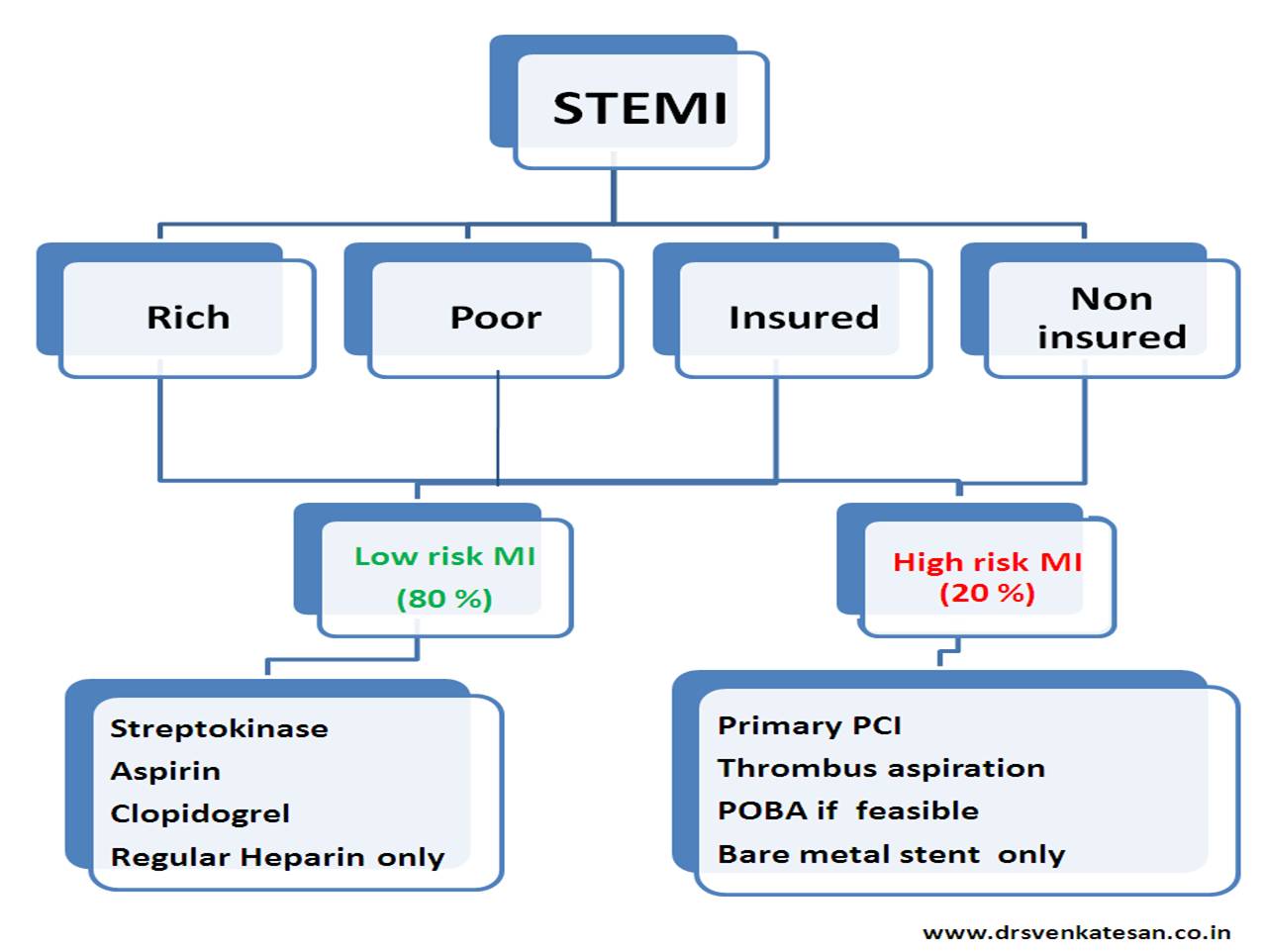
The first chart exposes the problem .The second one tries to address the issue
Please bear with me . . . if the stuff sounds too crazy !
* Too much care is also referred to as inappropriate care
And for the solution . . . try this
Posted in cardiology- coronary care, Cardiology-Coronary artery disese, cath lab tips and tricks, cto chronic total occlusion, Hardware techniques tips, tagged chronic total occlusion, cto, fielder xt, pci for cto, retrograde cto crossing, success in cto pci, tips and tricks on February 27, 2013| Leave a Comment »
Answer :
While each one of the above factor appears very much important morphology of the lesion is the clear winner ( Which includes , the content of the lesion , hardness , micro channels , thickness of the proximal and distal caps, the length and tortuosity of the CTO ( which is invisible ) the collateral status will ultimately determine the success)
It is becoming increasingly clear cardiologist expertise is getting less and less important .
Finally , it must be told to our younger generation of cardiologists , crossing a CTO and deploying a stent is not synonymous with success .It should result in long term sustained distal flow and make a significant impact on the patients symptoms (If at all any !) and survival.
Posted in Cardiology -unresolved questions, cardiology- coronary care, tagged right ventricular myocardial infarction, rvmi v4r, rvmi with st eelvation in v1 to v2 v3 on January 31, 2013| Leave a Comment »
Traditionally RVMI is suspected only with infero -posterio MI .
Can RVMI occur with LAD disease ?
Yes , it is reported up to 13 % of Anterior MI (Cabin AHJ 1987) . Right ventricle has an anterior wall and blood supply to this area is from LAD .
Have a look at this ECG
Reference
2. http://www.nejm.org/doi/full/10.1056/NEJMicm030315
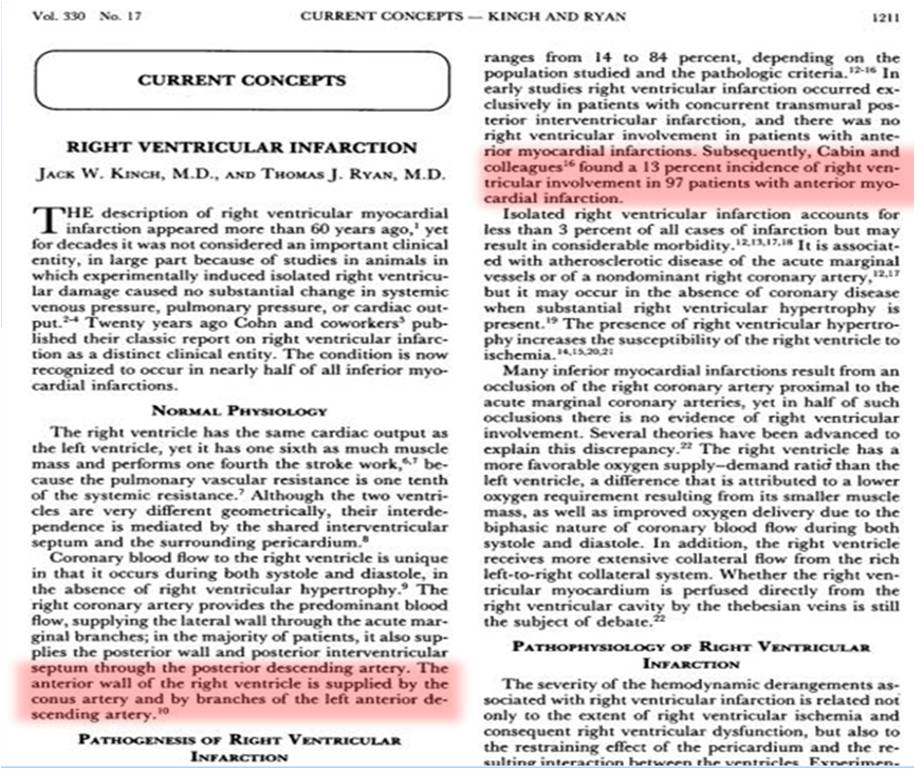
Final message
RVMI is not an exclusive complication of Infero -posterior MI.
Posted in Cardiology -Interventional -PCI, cardiology- coronary care, cardiology-Anatomy, Cardiology-Coronary artery disese, Echo library and gallery, echocardiography, great illustrations in cardiology, tagged left main by echo tte, left main coroanry artery, left main ostium, rare echocardiogram images on January 23, 2013| Leave a Comment »
If only . . . we get an image like this , echo can help rule out most left main disease with conviction .
Have a close look at it ! One can get a good image of coronary ostia in short axis view . But , here it is well visualized in long axis .

I tried to put color flow within left main .
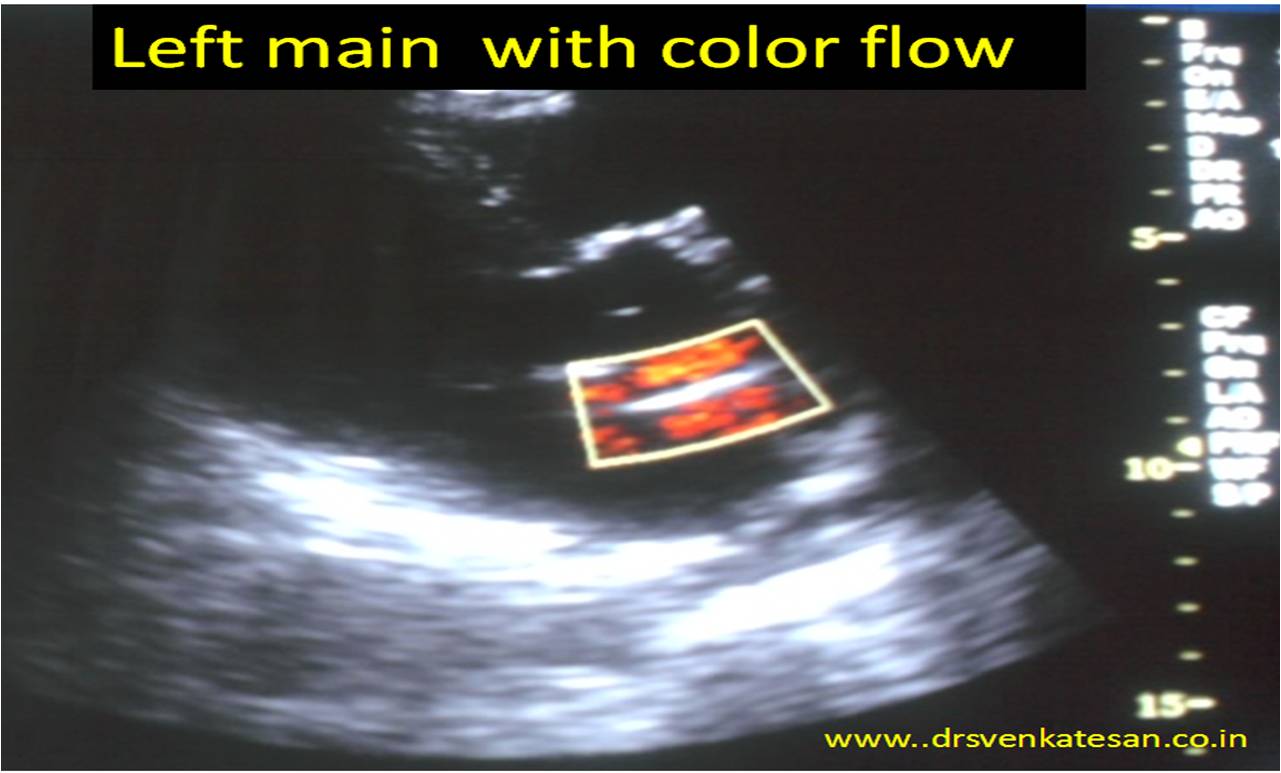
What about pulsed Doppler across left main ?
After all it needs 2mm sample volume and this left main was near 4.5mm . So keep trying !
Posted in Cardiology - Clinical, Cardiology - Electrophysiology -Pacemaker, cardiology -ECG, cardiology -Therapeutics, cardiology- coronary care, Cardiology-Arrhythmias, Clinical cardiology, Uncategorized, tagged adenosine, amiodarone, antidromic avrt, approach to narrow wide qrs tachycardia, Approach to tachycardia, avrt, dc shcok for vt, dc shock contrindications, hear rate in various tachycardia, icd rf ablation, idiot's approach to cardaic arrhythmas, incessant junctioanl tachycardia, maangement of cardiac arrhythmias, magnesium in vt, maze corridor procedure, multi focalatrial tachycardia, multiple accessary pathway, orthodromic avrt, pottasium channel blockade, pulmonary vien ablation and isolation, sinus node dysfunction, sinus tachycardia vs avnrt, sodium channel blockers in vt, tachy brady syndrome, wpw syndrome on December 30, 2012| Leave a Comment »
As I expected , my earlier algorithm “An Idiot’s approach to tachy-arrhythmias” has elicited mixed reactions .Some EPs calling it a dud while few physicians termed it awesome . Here is a follow up .
Heart rate of a tachycardia is the most neglected parameter by physicians . They are often seen spending hours together for decoding arrhythmia , splitting the brains for P wave location , VA conduction, Fusion beats etc .Finally they end up either administering Amiodarone a broad spectrum anti arrhythmic agent or DC shock.
Here is an unusual algorithm for arriving at a diagnosis in all tachy-arrhythmias based only on heart rate and the width of he qrs complex.
(Click over the table for high resolution image )

General principles in diagnosis of tachycardia
Narrow qrs tachycardias.
90 % rule : If regular It is sinus tachy if irregular it is A-FIB . Take some efforts to r/o sinus tachycardia . (In children and young adult it can be extremely difficult at times )* Please note : Sinus tachycardia can show some irregularity due to sinus arrhythmia and frequent APDs and JPDS . Further at fast rates P may fuse with T it should not be confused with A-fib .
Wide qrs tachycardia
Common things are common , if you sight a large animal with a huge trunk in a Kenyan safari , it is most likely to be an elephant and not a Dinosaur ! Please diagnose VT when you encounter wide qrs tachycardia by default especially when the BP drops !
Management issues
It would be foolish to split our heads for decoding an arrhythmia when a patient is unstable .Any hemo-dyanmic unstable tachycardia needs DC shock . (Synchronized will be better unless it is dire emergency )There are very few arrhythmia where DC shock is contraindicated ( MAT/Dig toxicity/Underlying sinus node dysfunction )
Only if the patient is hemo-dynamically very much stable the physicians have enough time to confuse themselves and the real ordeal begins .Please remember the 5 arrhythmias constitute 98 % of all known tachy-arrhytmia . So where ever you practice , whether in remote Nigerian village or sophisticated Cleveland university hospital , when you are confronted with a tachycardia the diagnosis should be one among the following five !)
All other tachy-arrhythmiaa are largely academic !
Regarding drugs
Knowing the mechanism of arrhythmia genesis is less important at bed side . They are triggered , sustained, and maintained by either functional or structural component .Ionic basis operates in every arrhythmia , but it is the anatomical substrate that maintains it .This happens in only diseased heart.The only point worth remembering regarding mechanism of arrhythmia genesis is , automatic and focal tachycardias will not respond to DC shock . All other can be termed some form of re-entry . Micro reentry for all practical purposes behave like triggered activity. Ischemic and electrolytic VTs are primarily ionic based and often polymorphic.Structural VT are commonly mono-morphic. Any VT just prior to degeneration to VF become polymorphic
Every patient with cardiac arrhythmia should be checked for hypoxia,acidois , electrolyte defect or exposure to any pro arrhythmic drugs. (The commonest cause of tachycardia in any IMCU , is inotropic induced (dopamine /doubtamine ) tachycardia .
We have 5 pharmacological options
General principle is ventricular arrhythmias are blocked successfully by sodium or potassium blockade Atrial and functional tachycardia are blocked by calcium or adrenegic blockade .Of course, there would be some degree of overlap when the arrhythmia origin hovers around the junction on either side of the AV ring . This is basis of verapamil sensitive VT .Clusters of calcium channels are scattered in the junctional region
Refractory tachycardia
In AVNRT/AVRT 90 % success can be achieved in most EP centers .VT ablation is still a complex process with success rate around 60 % ICDs are indicated in all recurrent VTs except incessant forms .(Where the battery will deplete within a month !) Surgical cure (Maze etc ) is possible in selected few while undergoing mitral valve surgery.Contrary to the modern scientific mood , I can ay with conviction most A-fibs can be managed medically except a fraction will require pulmonary vein ablation / isolation .
Final message
Mastering the field of of cardiac arrhythmias , though appear a daunting task , it does not require immense sense to understand real world problems are only a few and can be tackled in a simplistic manner !
Posted in Cardiology - Clinical, Cardiology -Interventional -PCI, Cardiology -unresolved questions, cardiology- coronary care, STEMI-Primary PCI, tagged bio markers in nstemi, ischemia mediated troponin realese, mechanism of eelvation of troponin in unstable angina, troponin i, troponin in ischemia, troponin t on November 20, 2012| 1 Comment »
Does Troponin release during Ischemia ? (Without myocyte necrosis )
How often this happens ? . Some believe , it is rare . Here is a possible explanation for it .I feel the mechanism is still not clear . It all depends upon the degree of ischemia.




