We traditionally believe LV enlargement results in dilatation of mitral annulus from below and result in functional MR.
A lesser known concept is , LA enlargement dilating the mitral annulus from above and cause MR !
Can atrial enlargement per se dilate mitral annulus ?
We often find some degree of MR associated with chronic atrial fibrillation.What is the mechanism ?We also know MR begets MR.Is it because of progressive LV or LA enlargement ?
When the literature is searched we have convincing proof that LA enlargement can lead to significant mitral annular dilatation and MR as well .
Spontaneous closure of VSD is a well recognised phenomenon, than ASD though both happen in equal frequency.The simple reason being VSD is a noisy disease , ironically the smaller the size of VSD more noisy it is . Hence it is rarely missed while ASD is largely silent in children. For this reason it is possible ASD may be the most common congenital disease .
Natural history of ASD(OS) closure
ASDs of size 3-4 mm 100 % will close by 3 years
Bulk of the ASD < 8 mm close spontaneously by 5 years.
ASD> 10mm is unlikely to close
Factors that determine spontaneous closure
Apart from size and location
Closure is accelerated by remnant of flap of foramen ovale
Fenestrations and Septal aneurysms also favor spontaneous closure.
Margins of the defect if rough triggers fibrotic reactions
Why SVC and primum defect do not close easily ?
Plane of ASD secundum is single and bridging of tissue is possible .
Sinus venous and primum defects exhibit holes which run in multiple planes hence approximation not possible . They also do not have a valve mechanism.
Un-natural history of ASD
In the current era, one more force interferes with spontaneous closure of ASD . It comes from the hyper trained aggressive Interventional cardiologists who compete with the nature and easily prevail over it !
IVC filter usage has increased many fold in recent years.Please note , it is not indicated in every case of recurrent DVT/or PE. There are specific indications.
Permanent IVC filters
Patients at risk for DVT /PE with absolute contraindication to anti-coagulants.
Recurrent DVT/PE in spite of adequate anti-coagulation
Temporary /Retrievable filters*
It is used during high risk periods for DVT following major trauma or Bariatric/Spinal /Neuro surgery (PREPIC 2 study ) .*Some of the retrievable filters can be kept for months ,years or even permanently. (If the risk period extends or it has trapped a huge clot.)
Outcome of IVC filter (PREPIC -8 year follow up study )
Fractional flow reserve(FFR) is an Intra coronary hemodynamic parameter promoted recently to assess the physiological impact of a coronary lesion . Though it sounds logically attractive the concept is sailing in rough seas .I am afraid FFR is drowning a fairly useful tool of IVUS along with it !
Read this large study on FFR (JAMA June 2014) .It seems to suggest FFR is a costly and unnecessary accessory in cath lab
Critical thoughts on FFR
It adds time , money , and procedural risk* to any given patient .The only possible use is to reduce the proliferating stent usage !But the irony is complete as we do our daily business in modern cath suits .To negate one indulgence we need to need to indulge in another ! (Junk begets Junk !)
It reflects lack of courage on the part of cardiologists to advice medical management even in obvious low risk lesions !
It is unfortunate ,we need a scientific or a pseudo scientific tool to lift up our sagging medical intellect !
* crossing delicate and often complex lesions without any major purpose is bad wisdom ! Continue Reading »
Inability to think beyond self , family, private life reflects a backward and immature state of human mind
How to eradicate this backwardness we all suffer from !
I stumbled upon a book which made me wonder , whether eradication of backwardness is little to do with education ! It lies much, much deeper in our cortical thinking influenced by inheritance , evolution , culture and economy .
The stunning truth was exemplified by American political scientist Edward C. Banfield .A must read for every one who have mind for society , community and the humanity !
In this book he introduced a new term to describe this self centered thinking as “Amoral familism”
“Banfield concluded that human plight was rooted in the distrust, envy and suspicion displayed by them in relations with each other. Fellow citizens would refuse to help one another, except where one’s own personal material gain was at stake. Many attempted to hinder their neighbors from attaining success, believing that others’ good fortune would inevitably harm their own interests”
Banfield theroy and “Moral Bankruptcy in Modern medical care”
I am afraid there is a compelling link between Banfield’s observation in a remote Italian village to the current medical community mind set who care only for their patients who pay them and keep them happy !
If you think education will eradicate social backwardness ,Why ? one of the most highly educated community that form the noble profession remain backward in their thinking !
How do you explain innumerable instances of hospitals , doctors shutting doors for lesser humans even in dire emergencies ! ?
Why do many of them join hands with powers that can be detrimental to the overall health of the society ?
The stunning irony is , they do it unashamed (with pleasure at times!) in violation of the oath they take when they join the Noble profession. Shall we call it as ” Moral Bankruptcy in medical care ?
Read further
Moral Basis of a Backward Society
Highlights of this book (Text from Wikipedia)
The Moral Basis of a Backward Society is a book by Edward C. Banfield, a political scientist who visited Montegrano, Italy . He observed a self-interested, family centric society which sacrificed the public good for the sake of nepotism and the immediate family. Banfield as an American was witnessing what was to become infamous as the “mafia” or families that cared only for its own “members” at the expense of their fellow citizens. Banfield postulated that the backwardness of such a society could be explained ‘largely but not entirely’ by ‘the inability of the villagers to act together for their common good or, indeed, for any end transcending the immediate, material interest of the nuclear family’.
While our brain perceives whatever option we choose is the best for the patient , in reality it is rarely true !
The only comment I wish to make, there is nothing called standard guidelines for complex and unusual problems .We need not be obsessed with protocols !
Please remember , If you apply standard guidelines in non-standard situations 9/10 times we are going to err !
So my choice would be, to go with your gut feeling , of course your gut should be alive , up to date and periodically maintained !
If you don’t have the guts . . . don’t worry you have plenty of other options !
A 40 year old women came with acute dyspnea who had a prosthetic mitral valve implanted 2 years ago for RHD .
An emergency echo showed a peak gradient of 35mmhg across the valve .She was on warfarin regularly and her last INR was 2.2.Heart rate was 138/minute, lungs showed congestion .LA,LV were dilated. LV function appeared mildly compromised but could not be accurately quantified as the patient was in distress.
The fellow on duty had no hesitation in diagnosing prosthetic valve thrombus .He Initiated Inj streptokinse bolus followed by infusion along with diuretics . After few hours the gradient regressed .Patient felt better .Every one was happy . The consultant congratulated the fellow for the good job done .To recognize prosthetic valve obstruction early and successfully lysing it too ! The fellow felt gratified .
Since I was hanging around the CCU , watching the proceedings , I Initiated a debate which was curious to the team that handled the patient !
Was it really thrombotic obstruction that caused his symptoms ?
No one has visualized the thrombus
TEE was not done
Fluroscopic evaluation of disk motion was not performed
There was no documentation of raising FDP that would Indicate clot lysis.
All we have is an unexplained tachycardia with raised trans prosthetic gradient . . .
Why we are tuned to think raised gradients to be synonymous with thrombus ?
There has been lot of assumption here . Subsequent analysis of history and clinical presentation revealed the patient had a febrile illness which triggered an atrial tachycardia that possibly resulted in transient LV dilatation and dysfunction.
Once the failure is controlled the gradient has come down , I argued !
Of course, this again could be a guess work , How can you still rule out a thrombus ? They wondered !
I told them , question here is not ruling in or ruling out prosthetic valve thrombus.
It is an important lesson to learn , raised prosthetic gradient is not equal to thrombus in many acute hemodynamic situations* .
Many factors other than prosthetic valve obstruction can elevate the gradient.
After all , prosthetic valve orifice is inherently stenosed .(MVO is never >2.5sqcm in any prosthetic mitral valve) . So at times of tachycardia the gradient is bound to be elevated .
Other factors that can elevate trans – mitral gradient includes
LV dysfunction
Acute diastolic dysfunction
Acute peri-valvular MR
Loss of LA compliance
*One of the commonest (yet not recognised) cause for elevation of trans mitral prosthetic gradient is acute left ventricular failure due to any cause.It can be either acute diastolic dysfunction or a sudden raise in blood pressure that result in after load mismatch.
Final message
Please remember flow across prosthetic valve is governed by delicate local hemodynamic rules .The gradient is critically dependent on heart rate, LA size and compliance , LVEDP and after-load mismatch if any !
Transient raise can occur at times of tachycardia and falling LV function (Mitral valve has to push hard, in the process elevating the gradient)
Simple raise in trans-valvular gradient should be carefully interpreted. Since visualising thrombus in routine TTE is difficult in an acutely dyspnic patient many of us have taken this granted !
Nothing wrong in playing guess games in medicine . . . but we need to acknowledge it!
*Note:Other causes for chronically elevated gradients like pannus formation, mechanical defects of valve, degenerated prosthesis should be addressed separately.
Can we close an ASD in a 25 year old women severe pulmonary hypertension ?
Volumes of literature has been written on the subject.Dedicated cath studies have been done with multiple parameters .
Still , there is a lingering doubt !
Here is a 3 minute practical* solution based on 5 easily available parameters. (*Also referred to as unscientific in medical parlance !)
1. O2 saturation
2. Pulmonary artery diastolic and pulse pressure
3. RV function,
4 .Systemic pressure
5. Functional class
If O2 saturation is > 90 % consistently there is likely to be significant left to right shunt .Closure is to strongly considered
If 02 saturation is near 95 % there is absolutely no contraindication at any level of PVR.
Systolic pulmonary artery pressure derived by TR jet is least useful index.Pulmonary artery diastolic pressure reflects true vascular reactivity of the pulmonary circulation.A wide swinging pulmonary arterial pulse indicates dynamism in circulation and hence operablity.
If pulmonary artery pulse pressure is wide (>50) , or PA diastolic BP is < 30 one can safely presume irreversible damage to pulmonary vasculature has not occurred and these patients would benefit from surgical closure .
RV function should be assessed carefully in every patient.This is as important as PVR .Significant RV dysfunction is an absolute contraindication.
Never close the shunt in patients who is in class 4 symptoms.
Never close a shunt if the systemic blood pressure is low( 90mmhg)
Some believe PDA may be closed at any given PVR , while worst outcomes occur with ASD as supra-systemic pulmonary pressure is possible.
Always monitor these patients meticulously especially in the initial days following surgery for deterioration .Most patients will do well if they cross the first 30 days. The RV learns to adopts with new pulmonary hemodynamics !
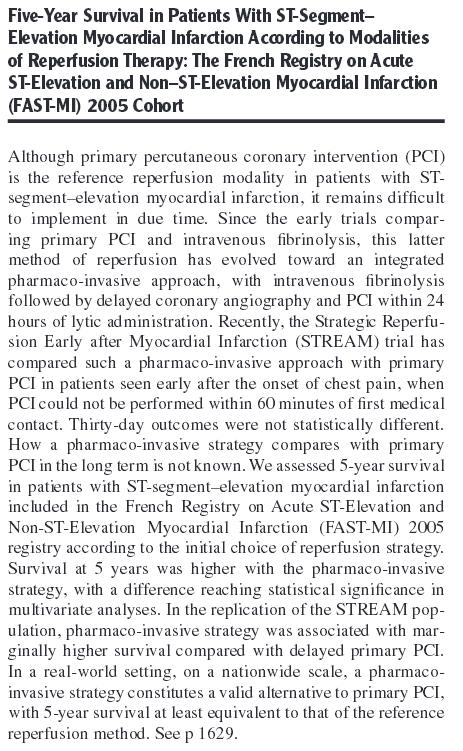
Many readers of this site might have wondered , about a series of biased articles pulling down the superiority of pPCI in STEMI.
This French study (FAST-MI) throws stunning data from the real world. Initial Fibrinolysis* defeated pPCI in all aspects of coronary reperfusion !
*When we say fibrinolysis arm it means Pharmaco -Invasive approach .Today our brain is irreversibly conditioned to believe standalone fibrinolysis is forbidden in STEMI . (Which I strongly disagree!) I am sure, very soon another stunning study will unmask the truth about standalone fibrinolysis as well !
Final message
The truth is , pPCI is really a superior modality in some of the complicated subsets of STEMI that too if performed fast.
In all other situations Initial fibrinolysis will rule supreme !
pPCI is not an Innovation for mass consumption!
Hence, “the roof top call” for pPCI for every STEMI is nether desirable nor feasible.
Now, we have this evidence from France (Which was well known to us a decade ago) As always , truth takes time to arrive , while falsehood can come instantly !
In 2014 , after two decades of celebration of pPCI the flagship Circulation journal throws this Editorial !
Unfortunately, there is a strong bias towards raw basic science when it is given in the filed of medicine.Do you know ,there is no Nobel prize exclusive for medical science ? It shares with human physiology the only field included for Nobel prize in medicine.
Evolution of human history reveals it is not the stunning scientific discoveries that impact the mankind . It is largely dependent on how we use them . It is true and natural ,invention of sub atomic particles , decoding quantum mechanics and trans-cellular signals always generate great interest than others.
In medical science, time and again we have seen problems arise in applying fruits of scientific research into practical usage in the patient domain in the bedside.
What is use of rewarding inventor of nitric oxide with a Nobel prize , when billion-dollar nitrate industry is thriving on a non existing life long indication of stable angina .
It is surprising to note , Nobel committee does give credit to wisdom & intellect while awarding prize in peace, literary or economic sciences. For some reason it lacks such a vision when it comes to medical sciences !
We have seen Nobel prize being awarded to organization that strive for peace and welfare of society and community like UN ,EU etc.The world health organization is the premier power supposed to provide and regulate the health in this planet.I do not recall any time WHO was close to considered for the Noble prize in medicine !
Nobel Ironies
Nobel committee rewards economists who point out lacunae in vital world macro and micro economics theories.
Dubious men(Heads of state ) are decorated with Noble peace prizes for preventing a war in one geographical area while doing exactly the opposite elsewhere !
In this modern millennium where scientific pursuits are contaminated and many of the research questions are misdirected or irrelevant , Nobel committee needs a through rejig in the manner in which medical Nobel prize is being awarded. We know ,Noble’s death wish was to award the brightest mind with highest scientific breakthroughs in those world . . . but
I guess Alfred Nobel if alive would have changed his rules .He wouldn’t have imagined modern science would systematically devalue common sense and reinventing it would also deserve an award equivalent to Nobel !
Some of the medical discoveries that deserve noble medical prize
States which excel in school health nutrition and other basic health programs for the downtrodden
Doctors who promote bed side clinical skills
Tobacco eradication networks
Organisations like medicine san-frontiers which strives for basic life saving medication for all
Journal houses that specialise on Medical ethics and clinical sciences
Medical professionals and institutions provide value education
Medical economists who expose the wasted financial resources that widen the gap between sick and rich
How about Nobel prize in cardiology for preventive cardiologist who successfully terminates a million statin prescription and restoring natural exercise directed lipid regulation in them ?
How about Noble prize for a noble physician sitting in corporate hospital infested with all commercial ingredients who could resist and argue successfully against inappropriate tonsillectomies and appendectomies ?
I am sure , such a man will be a laughing stock for most of us !
An appeal to Nobel committee
It is a wish , Noble prize in medicine is to be included for people who do yeomen services in preventive and clinical care and professional who carry forward the legacy of caring for the sick with clinical application of available scientific wisdom !
In this scientifically obsessed world , It will be a new beginning in the way future medical research will be directed and nurtured ! Only then the true power of Noble prize in medicine will be realised !
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.
















{kind=link}