VSD with Pulmonary atresia is a complex form of cyanotic heart disease .Though it’s a close companion of Tetrology of Fallot physiologically, it is a vastly different entity in embryological and anatomic terms.
TOF is cono truncal anomaly where abnormal anterior displacement of conal septum result in malalignment VSD, RVOT obstruction ,aortic override and RVH.
While ,pulmonary atresia with VSD is not a primary cono truncal anomaly, the defect occurs much earlier than TOF in fetal life , where the origin of PA fails to materialise,(Fetal arteritis?) and which triggers a series of anatomical disarray in pulmonary arterial circulation. The PA growth arrests in various levels (Somerveille Types) .It is important to realise while the PA may be patent , pulmonary valve is always atretic and disconnected from RV.
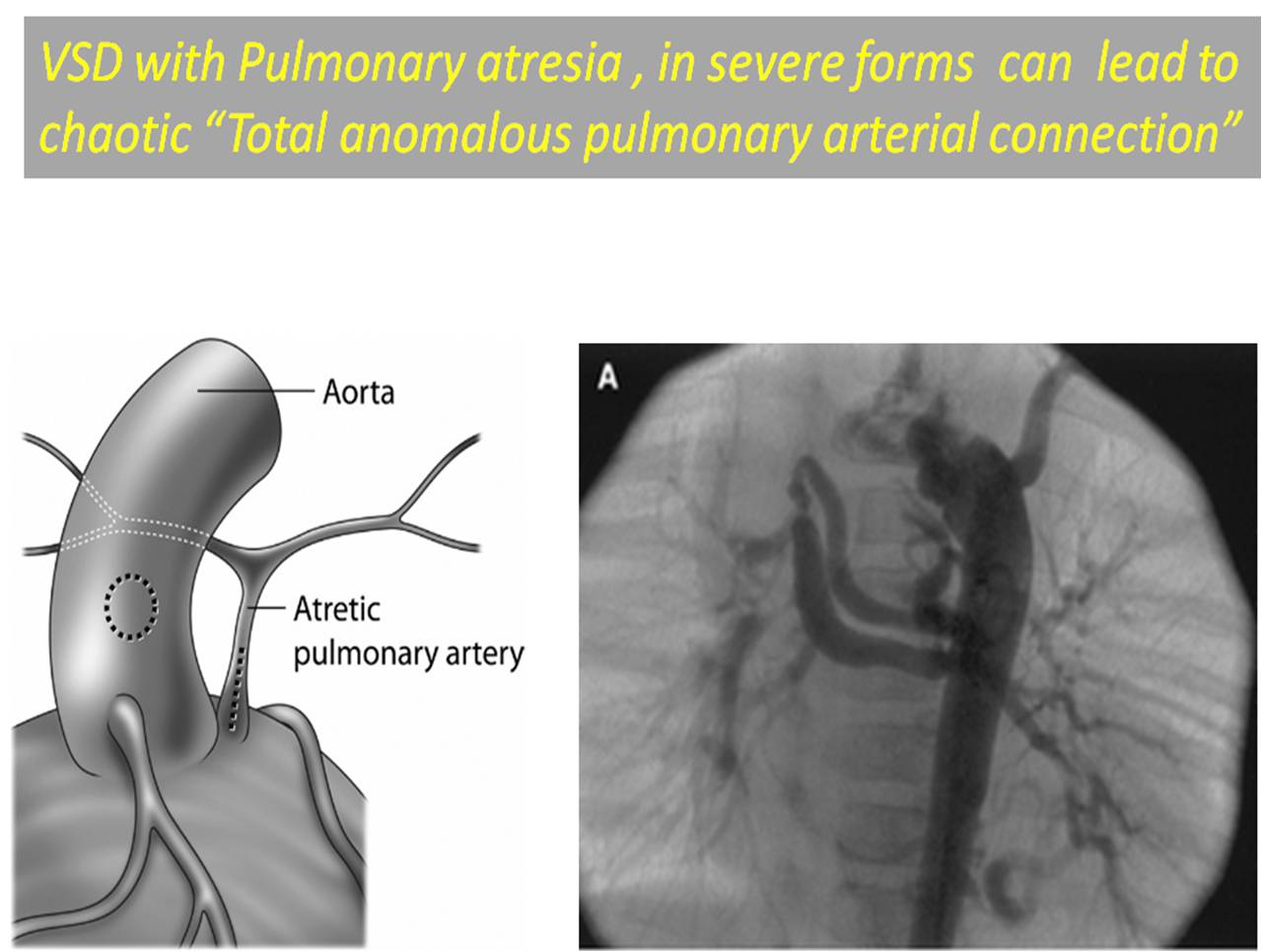
In severe forms there is Zero pulmonary artery content .The lung is perfused in chaotic manner. This situation akin to “TAPVC” in arterial side and result in total anomalous pulmonary arterial connection.

Natural History of PA with VSD .
The blood supply of lungs is maintained by MAPCAS.Since , the fetus is not dependent on its lung for survival, life goes on well , till birth and face the harsh reality that it has no independent blood supply for lungs from RV and has to depend on collaterals from aorta.
Survival depends upon the the quantum of collateral .( Size , number, arborisation pattern etc). Life is shortened in most babies and lost by 1 or two years . Exceptions are always there.Survival has been reported up to third decade in a few with a balanced pulmonary flow.these are the ones we catch up in young adults some times.
In effect , MAPCAS are the life line of these children , paradoxically the fate of these children piggyback on the behavior of the MAPCAS .
MAPCAS are not natural vessels that is meant to receive blood at systemic pressure. They are fragile and thin and when exposed to high pressure react pathologically.
Following anatomical and physiological effects occur in MAPCAS .
- Collaterals fail to grow with child
- Obstruction to MAOCAS can develop(Often at ostial)
- Collateral can be extensive causing pulmonary vascular injury.
- Regional and segmental pulmonary arterial HT can occur
- MAPCAS can suddenly rupture and cause fatal hemoptysis
- Collaterals perfusing more than normal resulting in volume overload of LV and failure
Principles of Surgery
The principle of surgery is to disconnect the arterial pulmonary vascular blood supply and connect all lung segments with pulmonary arterial supply and ultimately connected to right ventricle to restore the physiology.
Single vs Multiple staged surgery
The original concept was to do multi stage surgery , believing in the principle every stage give us time for pulmonary vessels and lung to grow .It involves extreme commitment of surgical team in identifying and understanding the pulmonary vasculature and the systemic collateral arborisation. The factors that is taken into account includes the presence of confluent PA , MAPCAS induced lung segment injury and its maturity . When pulmonary vessels are inadequate , autologus pericardial rolls are used as alternatives.
There is no point in vascularising a zone of lung with physiological low pressure neo pulmonary circuit which is unlikely to to work because of immaturity of distal veesels or its already damaged by the harsh pressure of MAPCAS!
We have realised the hemodynamci behavior of lung segments supplied by MAPCAS and the subsequent undoing of it is so unpredictable. The current concept is to recruit maximum lung segments and aim to provide revascularization through physiological manner.
An early single stage unifocalisation is suggested as a best option.(Reddy VM, J Thorac Cardiovasc Surg. 1995;109:832–45). Single stage repair is attractive not only in long-term hemodynamic advantage but also in the logistics . In multi stage repair ,only about 20-30% of children ultimately complete the treatment for various reasons.
It is heartening to note one of huge accumulated experience for surgical management of PA with VSD has happened in the southern Indian cities of Chennai and Hyderabad where i live.
Kudos to Dr Murthy and team for the pioneering work .Incidentally ,Dr KM Cherian is the legend in the filed of cardiac surgery and in my opinion he should get the title of the Father of pediatric cardiac surgery in India !
And this seminal paper from his team shares one of the largest experience who underwent single stage unifocalisation for PA with VSD in 124 patients.

What is the cardiologist role in VSD and PA ?
Cardiologist are expected to play a limited role . They can’t provide any cure as such.A meticulous cath study is all that required from them for the surgeon.
Selective MAPCAS angiogram requires special expertise ad through knowledge of anatomy .The MAPCAS are clustered around few specific zones.Now MRI and CT scan also can delineate the anatomy.
What is the surgical outcome ?
it is steadily improving globally.But only a hand full centers in the world can undertake such complex procedure(Lucile packard Children’s hospital Stanford is pioneer )
Hemoptysis in PA and VSD
It is a rare but an important issue .This can occur any time in the natural history even post operative. Most are managed conservatively .Interventional approach with embolisation is possible in expert centers.(K.Greaves et all)
Can the natural history be better than these complex unifocalisation surgery in these tender children ?
Statistically , it is possible in few cases, but to identify those children you need to get an appointment with God ! If parent’s take such a decision it should be welcomed and cardiologists and surgeons should not lure them with scientific excess !
Final message
The surgical correction of PA with VSD continues to be complex .Meticulous recruiting and unifocalisation of PAs and creating confluence , connecting the RV through a conduit may be the key.However, ultimately what is going to matter is the how the lung responds to these surgery hemodynamically !
It appears to me the whole process is more of a vascular surgery of lungs rather than heart !
Reference
2. An entirely new approach from Melbourne make this entity still curious !
3. An excellent resource on MAPCAS from Sao Paulo , Brazil