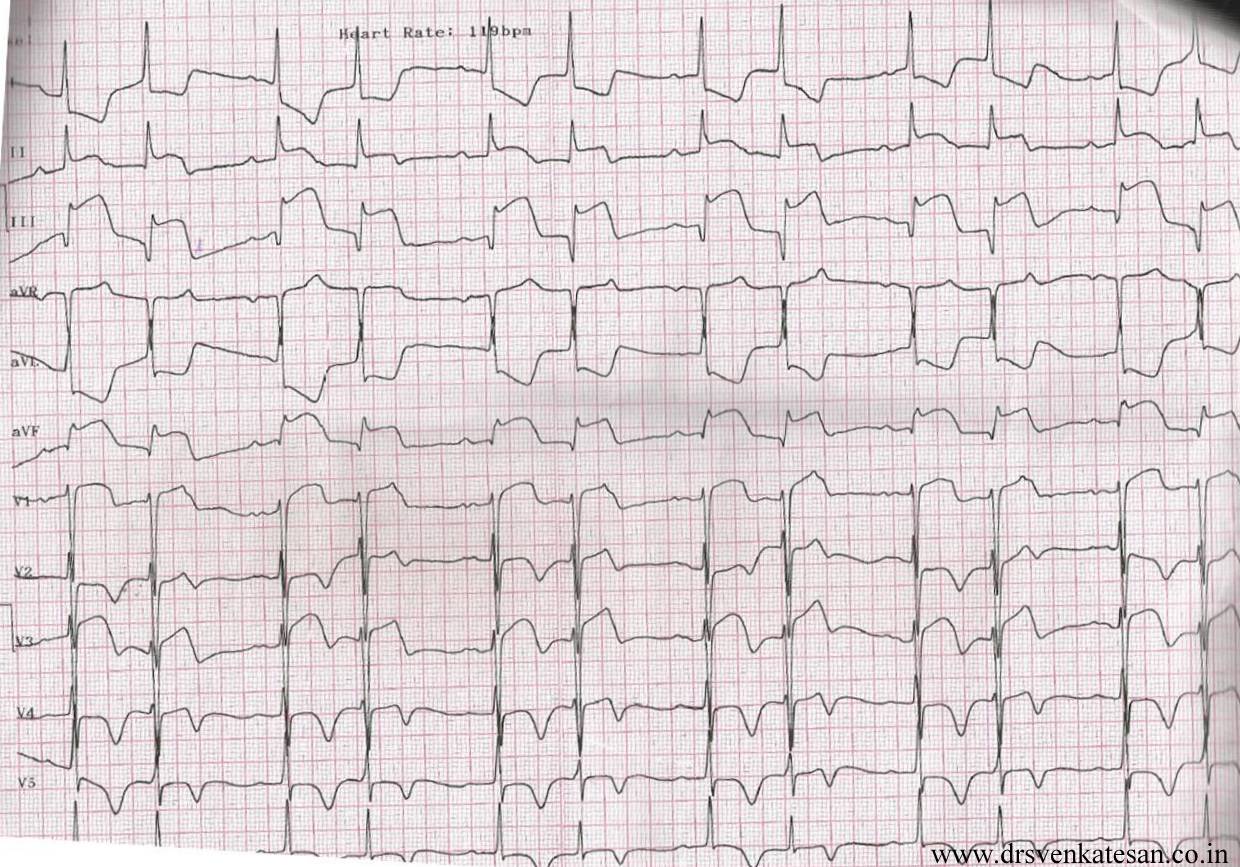
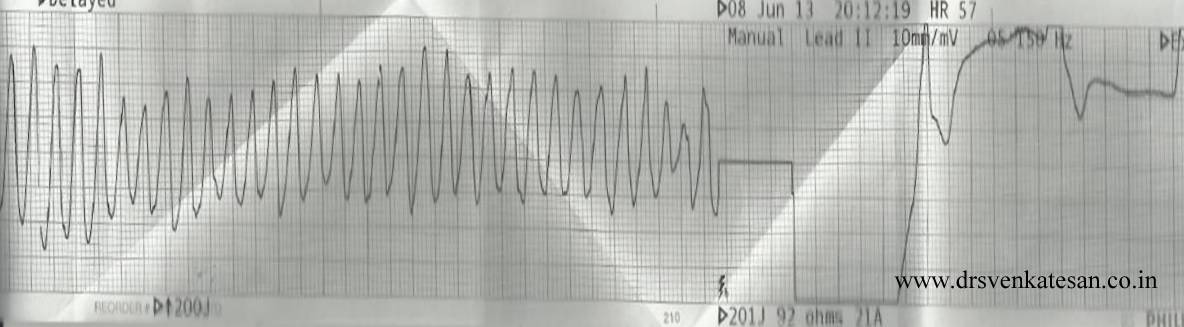
This is the story of a 55 year old women , who was received in our CCU with a dramatic STEMI (ECG looked like an action potential ) , LV S 3 and hypotension. It was impending cardiogenic shock.Since we do not have full fledged primary PCI program , thrombolysis was planned. She had cardiac arrest immediately after starting streptokinase infusion . She was promptly shocked and revived . The ECG changes rapidly reversed(ECG -3) . Every other hemodynamic parameter got stabilised as well . To our surprise ( few hours later ) this patient was so comfortable , sat up on her bed , demanded a discharge . (Which was refused of course !) One week later coronary angiogram was done, a near complete recannalisation of RCA was documented.
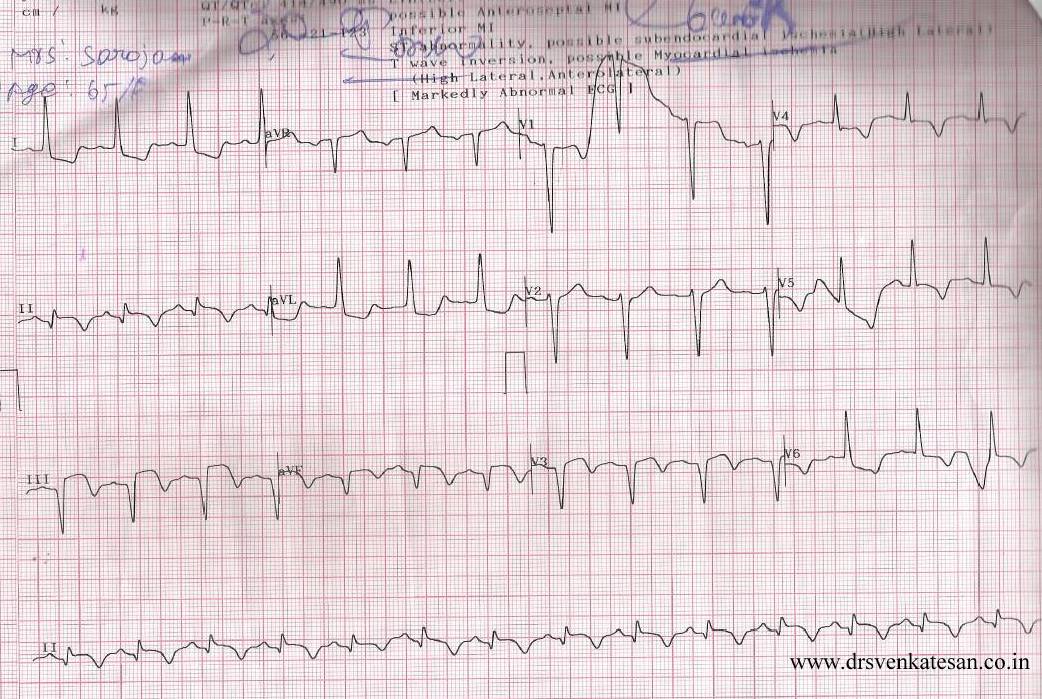
ECG 1 on arrival

ECG -2 Developed cardiac arrest 10 minutes after starting the Streptokinase Infusion

ECG -3 .Taken few minutes following the VF

Acute myocardial infarction (STEMI) kills more than a million life every year . Majority of death happens within an hour of onset of symptoms. Ventricular fibrillation is the arrhythmia of death. Why this occurs only in few , while many are immune to it ?
God keeps this secret close to his chest , how and why he selects candidates for this arrhythmia !
Scientists are still far away in finding the truth . But , one thing is obvious .The moment coronary artery is totally occluded , the heart begins a fight and try to get rid of this obstruction . In the process , it goes into convulsion (VF) with a foolish belief , it can shrug of the thrombotic insult . Death often ensues if not intervened . (Very rarely VF can be a non sustained one and patient survives cardiac arrest !)
VF as a electrical response to reperfusion injury .
Often times , we witness patients to go for VF very early following thrombolysis . The thrombus in situ is an irritant , it triggers the inherent fibrinolytic system (Natural TPA included) If it is successful it opens the occlusion ( atleast partially ) and salvages the myocardium .If the fate is against the patient , very early reperfusion of IRA triggers VF . If this occurs at home survival is low .If the VF occur at hospital the probability of survival is near 100 % .
The intensity of natural lytic mechanism is the major determinant of early reperfusion . Ironically the same factor determines occurrence of the deadly VF .
I would believe , the STEMI patients who die early (even before reaching the hospital ) are (un) blessed with a fighting heart ! Ironically , the lazy hearts reach the hospital alive ! (slow & steady win the race !) . Of course , reperfusion injury is not the only mechanism of VF . Other common suspect is left main STEMI .
Link to related video “Ignorance based cardiology ”
https://www.youtube.com/watch?v=J9DH6Vr04es
Final message
While , VF is referred to as arrhythmia of death , it may in-fact , represent a common form of reperfusion arrhythmia in the setting of STEMI ! . . . Hence , it can Initiate a new lease of life in many lucky ones ! I hope the title of this article makes sense !