Posts Tagged ‘evidence based cardiology’
A forbidden quote in medical science
Posted in Uncategorized, tagged empircal medicine, ethics in cardiology, evidence based cardiology, evidence based medicine, FAKE VS TRUE EVIDENCE, jama network, lack evidence, lancet, MBEST QUOTES IN MEDICAL ETHICS, MEDICALEDUCATION, nejm, randomised controll trials, venkatesan sangareddi on September 14, 2024|
Take a break from cardiology : How to debate a complex topic in a forum ?
Posted in Uncategorized, tagged evidence based cardiology, medical education, religion and god medical profession on January 16, 2023|
Pardon ,this video is nothing to do with cardiology. It is from the archives of the United nations library .This can teach some important lessons in art of communication , sharing to all folks, especially medical students. It was recorded in 1959 in Newyork, UN head quarters.Four 17 year old school girls & boys were invited for a debate on a complex topic. Does God exist ? How do you pray ? and what is the purpose of different religions ?
I keep wondering , how these youngsters accumulated so much wisdom and express it in such a polite manner too. Mind you, this was recorded , when learning happened with out any digital aids.The word Internet was unheard off. No ego, no bluntness, no diatirbes that has become a norm in many debates now. I got a punching lesson from this clip, be gentle when taking extreme views in any topic.
I wish, every medical debate in class rooms should happen this way.The key to succesful debate is, to accumulate knowedge, willingness to question the convention, and respecting the oppositie point of view.
The high point of talk show, was, when the Brazilian girl(due respects, she should be nearing 80 years now) tell us casually some things are not meant to be understood in life .I tell the same when some patients ask too many questions about their illness which may not have an answer.
Curve of wisdom in ACS : Open Cath lab doors may mean nothing , if the windows are closed !
Posted in acute coroanry syndrome, acute coronary syndrome, Cardiology -Criteria, Cardiology -guidelines, cardiology -Therapeutics, Cardiology -unresolved questions, tagged acc aha esc scai gudilines, acs, acs management, evidence based cardiology, open artery hypothesis, primary PCI vs thrombolysis, reperfusion, reperfusion injury, stemi, time window in acs on February 1, 2022|
“We have a 24/7 cath lab with an open door policy. Our cardiologist arrives at 15 minutes’ notice. Door to balloon time is less than 60-90 minutes”,
“Great, so, you can always offer a successful treatment for STEMI”
“No, that we can never guarantee.”
“Oh, It Is not the answer, I expected”
“I agree, it sounds disappointing, but. truths are less pleasing. What I am trying to say is, there are a number of factors other than the availability of a grand cath lab and agile and effortless hands, that try to reperfuse the myocardium in distress. I agree, we do save lives occasionally in a dramatic fashion. Recently we resuscitated an almost dead man with CPR and ECMO-guided PCI. But, most times it turns out to be just a customary ritual that takes us to the legal and therapeutic endpoint* of STEMI management”
*Both salvage & non-salvage
“I didn’t get you, Can you explain further?
See this curve and try to understand it yourself. (I would say, this is the ultimate curve to understand in the entire field of coronary care)

Can you guess what will be the outcome for C to B, or B to A ? In the real world, a substantial number of interventions take place at an Invisible point E beyond A Source: Gersh BJ, Stone GW, White HD, Holmes DR Jr. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future? JAMA. 2005;293:979–86
Acute “Corona” syndrome : Glad to know plaques are also in lockdown mode !
Posted in acute coronary syndrome, Cardiology -guidelines, Cardiology -Interventional -PCI, cardiology -Therapeutics, Ethics in Medicine, Uncategorized, tagged Acute corona vs coronary syndrome, ethics in cardiology, evidence based cardiology on April 3, 2020|
The Country of mine with 140 crore population, is under complete lockdown mode. We are anxiously tense in one aspect, but enjoying the free time due to the peculiar “Corona effect” on cardiac emergencies.
Unable to understand you . . . please go away
What happened to our 24/7 busy CCU ? Does it happen only in my hospital? Can’t be. Let me check it right now. I called my fellow, who has since become a leading cardiologist in the nearby town.

I have since called many of my close contacts. In both Government and private hospitals. The pooled data were analyzed in a virtual cloud memory. I am fairly convinced, our observation was indeed true.
The following can be considered as near facts.
- There have been at least 50% minimum dip of Overall ACS cases. It even went down to 80%reduction in a few places
- Even UA/NSTEMI showed a significant drop.
- There was general hesitancy to do primary PCI even if it’s technically Indicated.
- All most all STEMI were lysed. Heparin was liberally used.
- Many patients preferred telephonic consultations.ECGs were reported over mobile platforms
- None of the back pains & gastric pains were admitted as atypical chest pain.
- Most cardiologists closed down their regular OPD
- For the first time, Govt institutions were considered worthy to refer.
Why ACS Incidence nose dived?
- Under recognition?
- Under-reported ?
- Low Incidence?
- Low rate of referral?
STEMI that goes under-recognized and unreported? The consensus was, it’s less important factor as currently, very few are unaware of the Importance of chest pain and widespread availability of emergency services 108/911
Does that mean real incidence has Indeed come down?
The global atherosclerotic burden,(the substrate for STEMI) in the society is nearly constant. Still, the incidence of ACS has declined dramatically in the lockdown period. This conveys an important message and compels a search (research)
The plaques that are waiting to rupture in the population somehow getting a reprieve. Mind you, the presence of a risky plaque in LAD alone won’t cause a STEMI. It needs a trigger. The day to day physical stress, spikes of catecholamine, emotional swings, traffic pollution etc. The only plausible explanation appears to be the vulnerable patients along with their plaques are also locked up inside its Intimo-medial home. (Armchairs and bed rests can not only treat STEMI , they can prevent it too !)
Why the incidence of NSTEMI /UA has also come down?
Again, the same factors might operate. But, more likely self-stabilizing pseudo / Low-risk ACS is a distinct possibility.
A significant chunk of UA /?CSA/suspected NSTEMI patients come from referrals by GPs.The biggest pool of cases for cath labs comes from this group of noncardiac/Atypical chest pain syndromes*. Which shows some Incidental (In)significant lesions that subsequently becomes a cardiac emergency.
Since they have reduced their consultations the numbers have quite significantly reduced.
*Chronic CAD masquerading as ACS is not a forbidden concept
Final message
We are taught some important lifetime lessons in cardiac practice by this 20 nm, lifeless RNA particles.
1. The bulk of the ACS in the society is triggered by the day to day stress of the fast and furious “Just do it” world. The mitigating effect of social lockdown on physical and emotional stress on plaque dynamics on the incidence of ACS will be a big research subject in the coming months.
2. More importantly, It has exposed the existence of one more hidden epidemic in the community “manufactured coronary emergencies” propagated by a resistant cardio tropic virus that has disseminated deep into evidence-based cardiology. Let us cleanse this virus too after finishing off the Corona.
Postamble
It’s just a crazy opinion from a scribbling, blogger. However, I am sure, It’s only a matter of time, great journals like NEJM, JAMA, and Lancet will be screaming the same truths in a more palatable evidence-based manner.
Meanwhile, I can see early signs of restlessness(withdrawal) among us waiting for early release from the lock-up and resume the customary mode of evidence-based cardiology practice.
As I complete this write up . . . .surprised to find this report from TCT MD. Similarities if found, could only be coincidental.

An Idiot’s approach to evidence based cardiology !
Posted in bio ethics, cardiology journal club, Cardiology quotes, tagged ethics in cardiology, ethics in medicine, evidence based cardiology, guidelines in cardiology, guidelines in medicine, principles of medicine on October 20, 2013| Leave a Comment »
The current fad called EBM has lots of lacunae. Though evidence based approach is considered the ultimate journey towards truth ,lot of non academic factors contaminate it .In it’s current form , it is difficult to comprehend it.
This is an attempt to decode the mystery of EBM expressed in a simplified lay person’s term .They are the ones from whom we learn medicine. They are our teachers in the true sense.
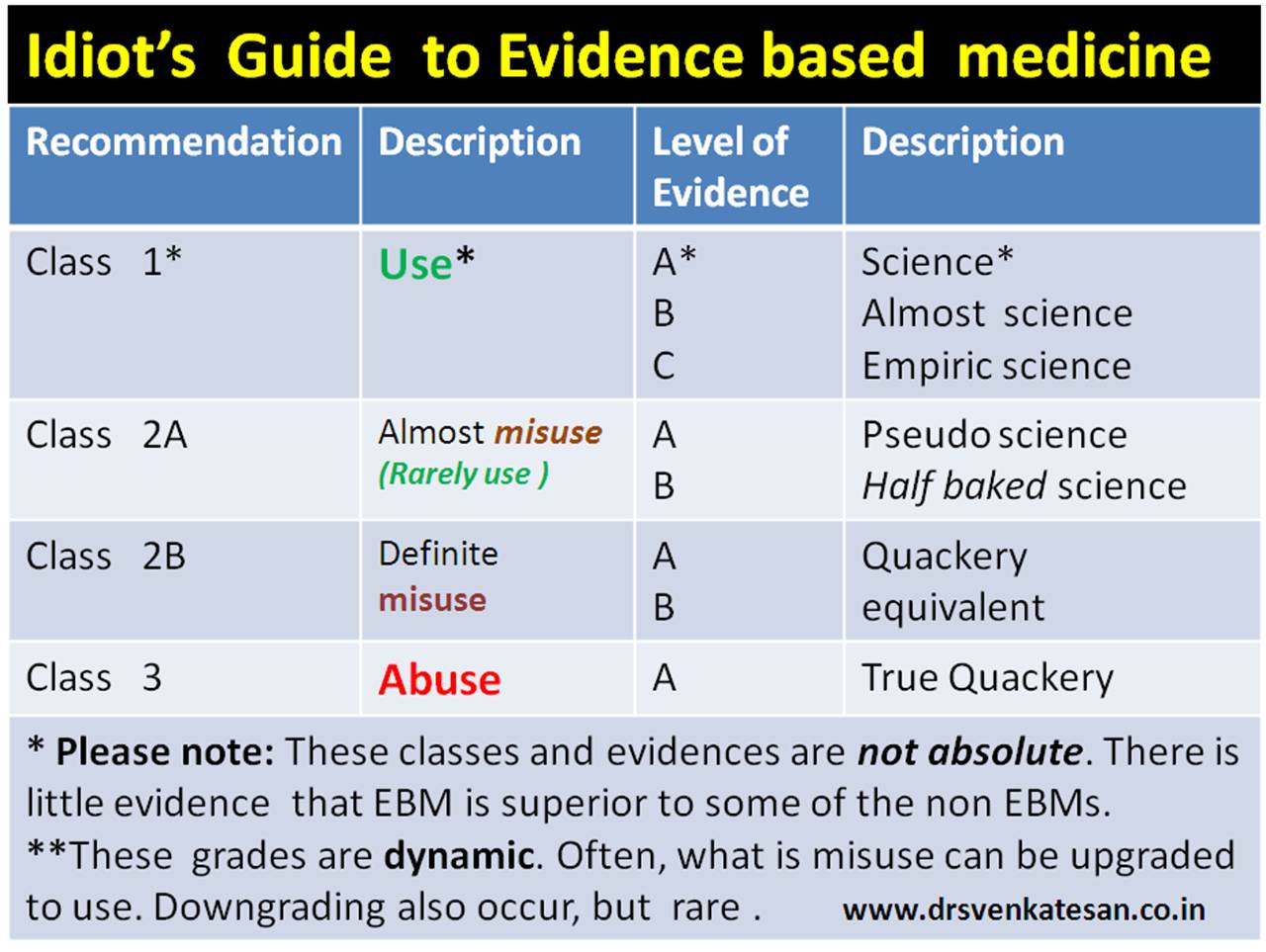 By the way ,it is also my approach to EBM .Sorry , if this post sounds arrogant ! It is not the intention .Truths often times appear brutal .
By the way ,it is also my approach to EBM .Sorry , if this post sounds arrogant ! It is not the intention .Truths often times appear brutal .
And . . . the Genius approach to EBM for comparison

How common is “Junk articles” in mainstream medical journals
Posted in Uncategorized, tagged evidence based cardiology, junk medical journal, medical journals on May 28, 2010| Leave a Comment »
There are about 5000 medical journals , churning out tens of thousands of articles every month .Most of these papers come from developed world where publication is made mandatory to get a medical degree . So it is not surprising to find proliferation of medical journals .
Publishing a paper is strictly monitored by a peer reviewing system in most journals . But , it is also a fact an article rejected out right by a journal , invariably appear in some other journal.
There is a joke going around among medical researchers, if it is difficult to get your article published in a journal , you start your own journal . . .It is much easier !
Where is the problem ?
Further , bulk of current day research work is sponsored by drug and device companies .It is possible these papers may have 100% acceptance rate.
Brighter side
Even in this scenario , it is heartening to find occasional excellent academic treasures and landmark research articles .

How common is irrelevant , pseudo , futile , clinical research articles published in medical journals today ?
I agree , I have prejudiced view on this issue . I would like to know am I really wrong ? What is your take on this issue ?
The most important journal in cardiology !
Posted in bio ethics, cardiology -Therapeutics, cardiology journal club, cardiology journals, tagged ahj, cardiology, circulation cardiovascualr quality and outcomes, evidence based cardiology, great cardiology journal, jacc, nejm, top cardiology journals on April 17, 2010| Leave a Comment »
Which you think is the most important journal in cardiology ?
- JACC ?
- Circulation ?
- American journal of cardiology ?
- American heart journal ?
- Heart rhythm ?
- European heart journal ?
- The Heart ?
- Journal of invasive cardiology ?
- NEJM ?
- Lancet ?
None of the above . . . is the right answer !
Probably, the best journal that is going to have the greatest impact in cardiology practice in the future could be this . . .

Unfortunately most cardiologists are unaware of this journal . The need for this journal , that too from most respected Circulation family , will vouch for its importance in the current era of cardiology that is driven more by the market forces than by the academics.
Click here to reach journal
Journal Highlights
- This journal is 3 year old , and most of the medical colleges do not subscribe to this.
- None of the 100 cardiologists who were questioned , were unaware of such a journal.
- Even those who read this journal often term as boring , academic and not practical !
The Circulation team which started this journal with only one purpose . . .that is , auditing the uncontrolled proliferation of pseudoscientific literature without proper quality assessment and dubious outcomes. Three cheers to the circualtion team for publishing this journal and let us propogate the importance of this publication.
Adventures in Cardiology : A great story , must read by all interventional cardiologist & electrophysiologists !
Posted in cardiology-ethics, tagged atrial fibrillation, ep study, evidence based cardiology, pulmonary vein ablation, rate control vs rhythm control, RF ablation on December 19, 2009| 1 Comment »
This is a real life experience of a patient who underwent a electrophysiology study and ablation procedure for atrial fibrillation .The blog describes how the procedure became a nightmare .Written in a most readable fashion . Interventional cardiologists need not get hurt by this narration instead they should do a reality check on the dangers of the some of the complex procedures !
Click over the image to read the real time experience of Pulmonary vein ablation

Image courtesy Mayo clinic
The message from the above story :
- Atrial fibrillation is one of the relatively benign cardiac arrhythmia , that can be treated with simple and effective drugs . Now we have strong evidence to say rate control is equally , if not more effective than the rhythm control modalities .
- The RF ablation , which aims at rhythm control is a too complex a procedure with lots of expertise technology .
- This should be reserved as a last resort in an occasional patient who had exhausted all other options .
- Patients should realise , the consent forms they sign before any new and innovative procedure is always incomplete and he may be the first person to experience a new complication hitherto unreported .
- A cath lab is run by a team , you can’t expect the chief doctor to be on your side always. Many of the procedures are done by either experienced or inexperienced fellows . That’s only the way medicine can be practiced !
- So beware all patients , many times, modern medicine is nothing but experiments on live humans !
Can we afford to miss a diagnosis of acute coronary syndrome in the emergency room ?
Posted in cardiology -Therapeutics, cardiology-ethics, Uncategorized, tagged acute coronary syndrome, cardiology, drsvenkatesan, ethics in medicine, evidence based cardiology, hippocrates on December 16, 2009| 1 Comment »
Modern era of cardiology aims to treat ACS as and when it develops .That is , as soon as the vulnerable plaque ruptures or a thrombus blocks the victim’s coronary artery.
But this can be achieved only if the patient reacts to this event.We know 20% of ACS can be totally silent. Some produce very vague symptoms especially in elderly and diabetics. ECG and enzyme changes may help us in patients who do not have clear symptoms.There are variety of markers available for STEMI & UNSTEMI.(CPK-MB, Troponin T , myoglobin etc) Now we are working at finding a marker for ischemia without necrosis. Ischemia modified albumin is one such molecule that is showing promise.
The ER department world over have vigorous screening protocols to diagnose ACS for the patients with chest pain. There are thousands of triaging protocol in the emergency management of chest pain.In spite of the highest awareness and availability of scientific expertise , knowledge base the error rate of diagnosing ACS stands at an astonishing 58%. This may seem odd , but this is what this land mark article in NEJM tell us (Data from Boston , Milwaukee etc).
Out of 10500 patients with suspected ACS. Only 17 % had real ACS. 55% were admitted initially as ACS later turned out to be non cardiac .This may seem acceptable for many even if it is an act of unnecessary admission and investigation. It gives us , a sense of satisfaction for not missing a diagnosis of ACS. But it has it’s own risk of complication arising out of unnecessary investigations.It is a chain reaction of suspicion that may end up in a coronary angiogram in many ! .It is also a well recognised fact these patients spend atleast an average of 2 days to get rid of the ACS tag over their necks .
Experience has taught us simple presence of a human being as a patient within an ICU ( however short the stay may be ) can be a health hazard and risk . This 55 % error , which does exactly this to our patients with chest pain who reach the ER never bothers us This is because we feel credited both academically as well as financially .
In the same study 2.3 % (About 25 patients) with true ACS were sent home after a missed diagnosis . Paradoxically this 2.3% has worried the medical professionals too much . . . This happens , even as we do not have proper data on how many of them had a real adverse event after a missed ACS.

So the message here is even in best centres both missed and wrong diagnosis are rampant. while wrong diagnosis (25 fold more here ) is easily accepted by the medical community .We can justify this as a screening camp for ACS , akin to arresting a group of suspected criminals in a preventive raid , later releasing for want of evidence.
In the morals of criminal judiciary , it is often said one can afford to lose a real offender from the clutches of law , but a innocent should never be punished in any circumstance .
In medical parlance this goes something like this . . . Thousand patients shall die because of his or her illness but not even a single healthy person should die due to unnecessary treatment.
The above thoughts were in response to the excellent original article on missed diagnosis of ACS from NEJM. http://content.nejm.org/cgi/content/full/342/16/1163?ijkey=652d8337709a8bf84c813f4c9d685863ee053162
Final message : (Sorry for the lengthy message !)
Can we afford to miss an ACS in emergency room ?
“Definitely not” . . .but do we succeed in that ? The answer is same “definitely not “
When we are able to accept with pride every time we make a wrong diagnosis of ACS in perfectly normal people , It may to provocative to say we can also afford to do the same when we occasionally miss a diagnosis of ACS as well . Law of statistics dictates for every correct diagnosis made there is many fold number of wrong or missed diagnosis takes place. May be , reducing that is the only aim of medicine.
We need to realise with even with a 55% of false positive initial diagnosis 2% real ACS escape net !The only fool proof method for not missing , even a single case of ACS is to label every patient with chest pain as ACS .
In this vexing issue , we should realise , in field of medical decision making , errors due to acts of commission ( Making an inappropriate drug/procedure /surgery is easily accepted by medical professionals as well as the court of law !) . But acts of omission , like missing a diagnosis or failure to prescribe a drug or perform a procedure is rarely accepted and is considered a great negligence and bring intense guilty feeling among the physicians .
This perception is definitely not warranted in this greatest profession of glorious uncertainties ! Both acts of commission and omission cause significant damage to patients . In this modern era , we have clear statistics that reveal , acts of commission leads far ahead over it’ s counterpart in injuring our people .
Hippocrates got it right over 2000 years ago . First let us do no harm . . .
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- March 2026 (5)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,630,221 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note


{kind=link}