Human myocardium does not read hospital sign boards . It simply doesn’t bother whether thrombolysis is done in a moving van or a stationary room . When confronted with a life threatening emergency , all that it demands is quickness with which it is administered. Yet, in modern interventional cardiology, a same thrombolytic drug transforms from a life-saver into a forbidden clinical error, depending on whether it was injected in an moving ambulance or in the emergency Department.
This is the comical, yet tragic, irony of modern STEMI care.
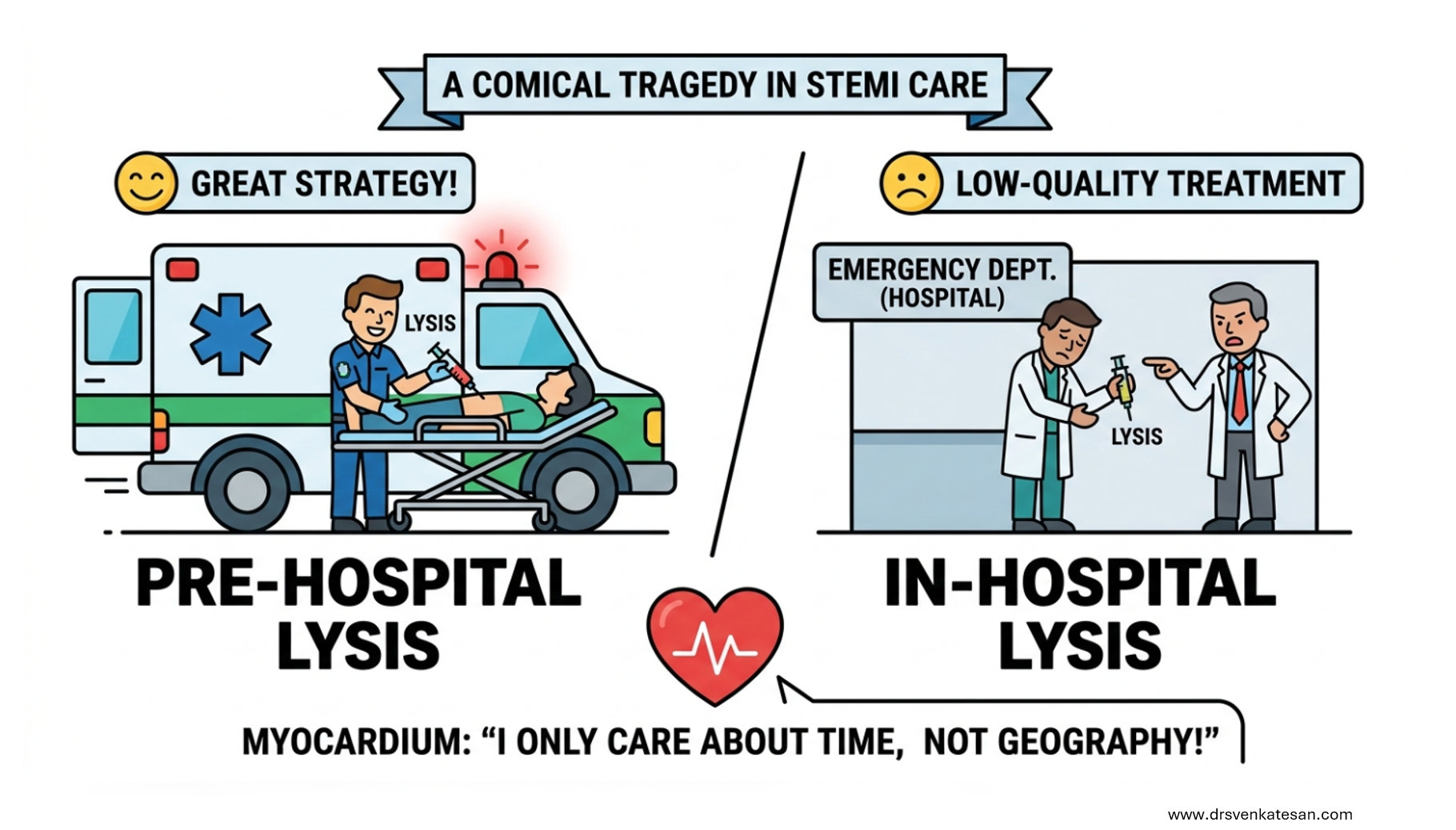
Pre-hospital lysis is celebrated as a great strategy , while ultra fast in hospital lysis even within the “golden hour” is frowned upon as low-quality treatment.
At the heart of this paradox lies , the cult like status of primary PCI .It is true, pPCI has been etched as the gold standard of ACS care. However, most of the experienced cardiologist* know its perceived supremacy is not absolute ,largely attributed to the seductive power cath lab . (* Few have the courage to admit it )
Respect the myocardium not the cath lab
The efficacy thrombolysis is strictly a function of time, not geography. Landmark data from the CAPTIM trial explicitly demonstrated that when thrombolysis is administered within this early window, mortality rates are equivalent, and in some subsets superior, to immediate pPCI.
The current system of care willingly accepts this when a paramedic administers the drug but reprimands a physical if he does the same in his CCU .Why ? We seem to suffer from a misplaced academic arrogance that demands , fate of every coronary event must be decided only in cath lab. Any thing else is considered as deviation from the standard of care
Final message
It is time to change how we use the terms “pre-hospital” and “in-hospital” thrombolysis and replace them with a simple terminology . Symptom to Reperfusion Time. If a patient presents to a pPCI-capable center within the first hour standalone, ultra-fast ER lysis should be made an established, protocol equivalent to pre-hospital care, which is at equipoise with (un)disputed gold standard of pPCI as per the landmark study of CAPTIM.
Postamble
It is heartening to note In-hospital thrombolysis continues to be dominate mode of reperfusion at any point of time, inspite of the negativity surrounding it. Can we take this as a proof of real mettle of pPCI ?
References
- Gersh BJ, Antman EM. Selection of the optimal reperfusion strategy for STEMI: does time matter? Eur Heart J. 2006;27(7):761-763.
- Steg PG, Bonnefoy E, Chabaud S, Lapostolle F, Dubien PY, Cristofini P, et al. Impact of time to treatment on mortality after prehospital fibrinolysis or primary percutaneous coronary intervention: data from the CAPTIM randomized clinical trial. Circulation. 2003;108(23):2851-2856.
- Terkelsen CJ, Lassen JF, Nørgaard BL, Gerdes JC, Jensen T, Giebels V, et al. System delay and mortality in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Circulation. 2010;121(11):1307-1315.
- Armstrong PW, Sinnaeve P, Goldstein P, Lambert Y, Miroshinnychenko O, Danays T, et al. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. Circulation. 2023;148(9):753-764.










{kind=link}