Top 5 conditions that closely mimic and often mistaken for STEMI !
- Early repolarisation syndrome
- Left bundle branch block(LBBB)/ Left ventricular hypertrophy(LVH)
- Hyperkalemia
- Pericarditis
- Brugada syndrome
ERS
The repolarisation is due to K + efflux . The K channel porosity is subjected to high degree of genetic variations .If the repolarisation starts even by 10 milli- second earlier, it would have early take off from descending limb of R wave and the J point ST segment appear elevated.
- Common in young males . Especially in vago-tonic persons with relative baseline bradycardia
- The ST elevation in ERS is often global .
- Concavity is upwards .
- ST elevation can be dynamic ( Further confusing the picture ! )
- On EST it is expected to the touch the baseline .
- Benign entity in most . ( False alarm of STEMI is the major risk !)
- There is some evidence ERS may confer a risk of primary VF , if they experience a true STEMI (Michel Haïssaguerre 2008 NEJM )
* STEMI in ERS : The issue becomes too delicate , if a patient with ERS develops a true ACS . ERS being a common ECG pattern in general population , it is not wise to label every chest pain in ERS patient as benign . Suspicious ones demand observation in step down units , at least !
LBBB
“Any patient with LBBB & chest pain . . . suspect MI” .
Unfortunately, this rule is too reverently followed by physician community. In fact , ACC/AHA guidelines reinforced this behavior , as it added a key word in their STEMI guidelines “New onset” or “presumably new onset ” LBBB is an indication for PCI/Thrombolysis .( Physician presumption is a too delicate thread to hang our concepts ! )
Every LBBB is new onset unless you have a documented proof otherwise . . . it seems to suggest !
Probably , this is the reason many of the LBBBs are thrombolysed when they present to ER in an acute fashion . Of course , we can apply criteria of Sgarbossa to differentiate ! however flimsy it may appear . It help us to exclude few benign LBBBs. Still , Sgarbossa will struggle to differentiate an acute STEMI in Chronic LBBB from an acute LBBB in old AWMI .
Simply put . . . even old MIs are at risk of acute intervention if they have LBBB and vague chest pain !
How to overcome this ? Always rely on clinical features . If STEMI is causing the LBBB , it should be a large extensive one and you can not expect the patient to be comfortable .(Logic would suggest necrosis of large parts of IVS is necessary to cause LBBB ) Chronic LBBBs are relatively comfortable .
Of course , there is one another issue to comprehend ie transient ischemic LBBB .We do not know the true incidence and long-term significance of this entity . Here , LBBB is not due to necrosis of the bundle but due to ischemia . (Almost impossible to differentiate it from rate dependent LBBB with aberrancy )
Role of enzymes and Echocardiogram in LBBB and suspected STEMI .
You can always ask for Troponin T / CPK MB .(They are helpful only if 3 hours have elapsed , can we afford to wait ? ) . LBBB due to STEMI will purge a large quantum of cardiac enzymes from the infarcted zone . (So a marginal elevation is not going to help!)
Unfortunately, LBBB can induce wall motion defect in septum that may awkwardly simulate an ischemic wall motion. Even experts have erred in this . One clue is, the motion defects can not extend into anterior wall . It is confined to septum ,the second clue is a little delayed post QRS thickening of IVS (Septal beaking sign will vouch for benign LBBB with fair degree of success )
LVH
- LVH can mimic a STEMI due to secondary ST/T changes . (Secondary to tall R wave )
- LVH with incomplete LBBB – A very common association that can further elevate ST segment in v1 to v3 .
- Left ventricular hypertrophy mimics old MI as poor R wave progression in V1 to V3.
- Contrary to our belief even Inferior leads can show q waves due to inferior septal hypertrophy.
Hyperkalemia.
With aging population and rampant acute and chronic renal disorders it is becoming a daily affair to get calls from medical units for ECG changes .We know the rapidity of efflux potassium is responsible for ventricular re-polarisation .Phase 2, and 3 are K + exit zones. This is the same phase ST segment and T wave are inscribed.In hyperkalemia K + accumulates inside the cell and keep ST/T segment elevated .T wave also becomes tall . It can mimic both as hyper acute STEMI .
Read a related article (Dialyisable current of Injury )
Pericarditis
- ST elevation is not confined to an arterial territory
- Can be global .(Regional ST elevation does not exclude pericarditis)
- ST elevation is concave upwards as in ERS
Link to Read regional pericarditis
Brugada syndrome
Brugada syndrome is an ECG -Clinical complex in which ST elevation in pre-cardial leads is associated with ventricular arrhythmia. The defect lies in sodium channel . It reflects a mis -match between RV and LV epicardial repolarisation forces .It keeps the RV epi-cardial current afloat and the pre-cardial leads facing the RV records ST elevation that mimics STEMI. It often shows a RBBB pattern and varying patterns of ST morphology . The ST segment is also subjected to dynamism , due to change in autonomic tone and myocardial temperature .(Febrile VTs)
After thoughts
Other close contenders for the top 5 slots
Myocarditis
Acute pulmonary embolism
Dissection of aorta
More
- Acute stroke (Neurogenic ST elevation )
- Stress cardiomyopathy (Takot Subo )
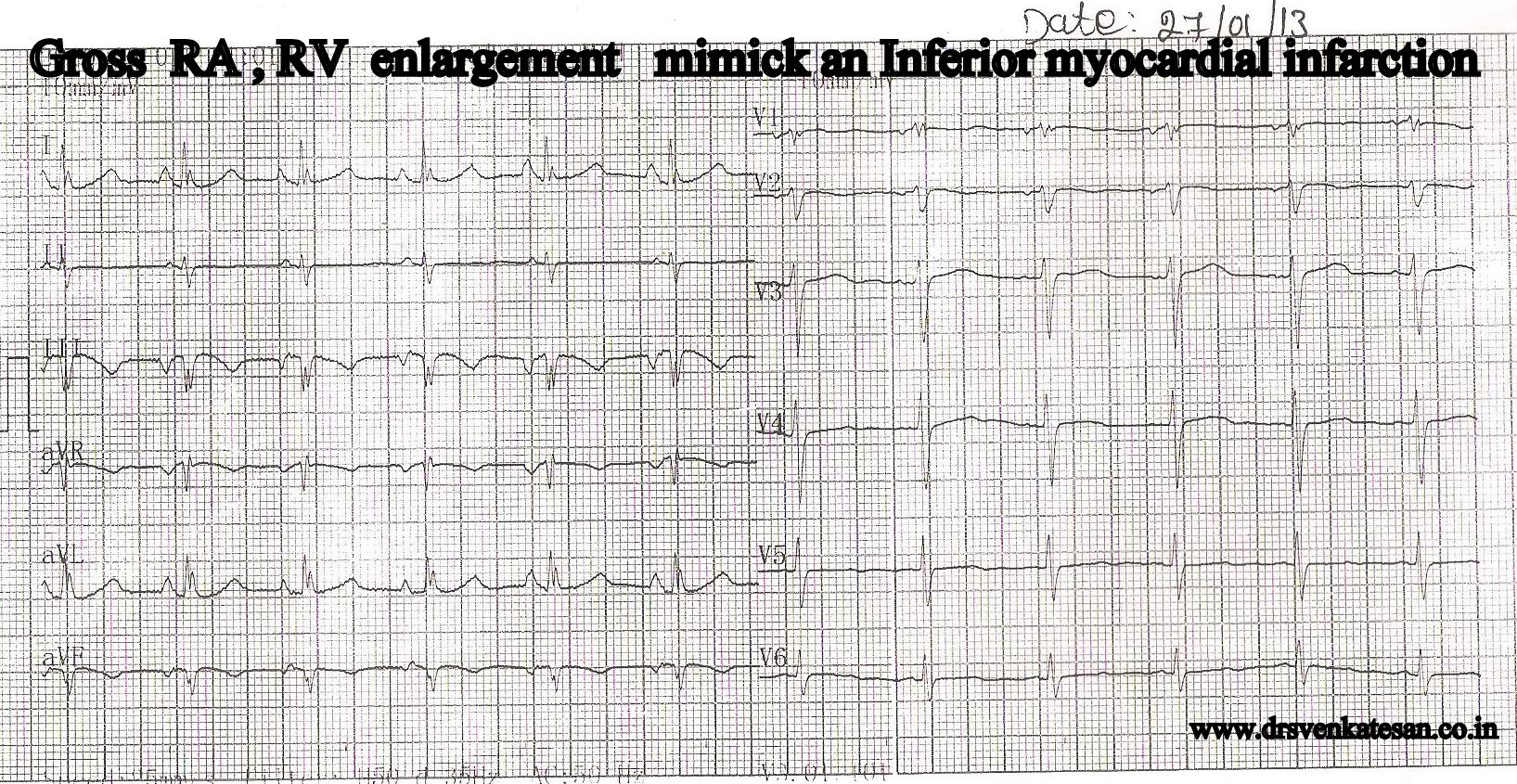
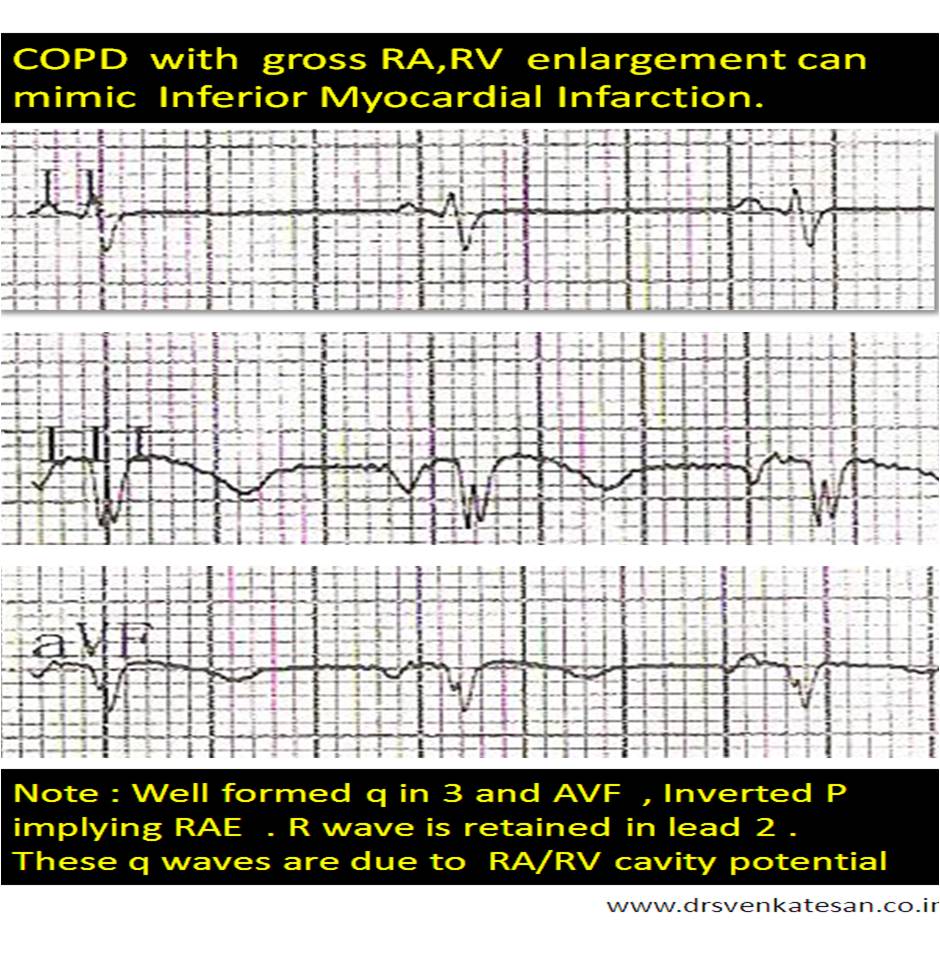
- Acute abdominal conditions mimicking inferior STEMI.
- Panic attacks /Anxiety states / chronic anti psychotic medications which are known to elevate ST segments.
- Contusion chest
(Cocaine hearts / Coronary arterial spasm / LV dyskinetic segments and LV aneurysms were not nominees ! )
Read Full Post »