Thrombolytic therapy was a mini revolution when it was introduced two decades ago .It has since evolved , not only in the molecular structure but also in it’s usage pattern.
The first generation streptokinase is continued to be used even today . While the latest generation thrombolytic agent TNKTPA(Tenekteplase) is threatening to push the old warrior out of CCU.

(Of course the American Physician & Pharma community never gave the due respect to streptokinase !)
The two common indications for thrombolytic therapy are
- STEMI
- Acute pulmonary embolism
Uncommon indications
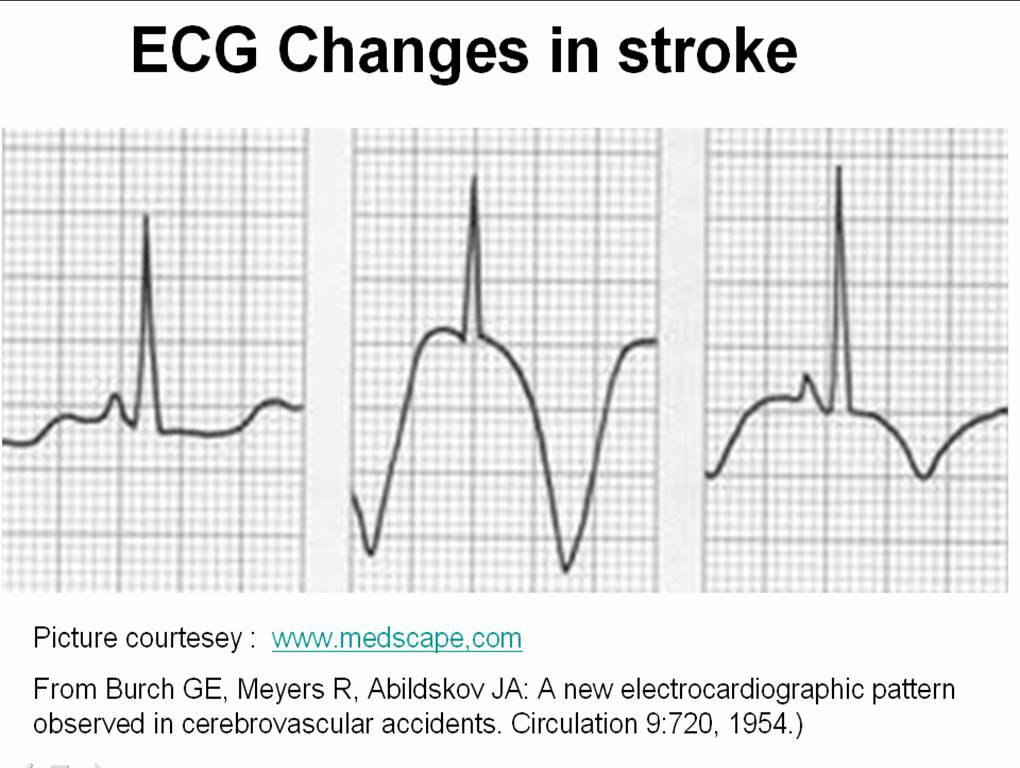
- Stroke( Can be common in few institutions)
- Prosthetic valve thrombosis
- Rarely DVT
From the beginning , there has been a controversy about the thrombolytic dosage and the speed with which it is to be administered .Let us recall , streptokinase was initially used in various regimes ( 5-30lakh units between a 10 -3hr infusion ) Later ,we arrived at a consensus at 15L units in 1 hr infusion . TPA also experienced the same . Which settled for front loaded regimen(35 + 65mg) . The confusion reappeared when we developed bolus thrombolytic agents( TNKTPA) .
In STEMI thrombus formation is often a one time process while thrombolysis is a continuous process. In pulmonary embolism both thrombus formation and lysis is often continuous process .
The success of thrombolysis depends on the sustained drug concentration , the pressure at which the drug interacts the thrombus.
Many times it is prudent to administer intensive heparin after thrombolysis to prevent recurrent thrombosis. Further , most of the pulmonary embolisms will require long term anticoagulants.
How to maximize the success of thrombolytic agents ?
- Local catheter based thrombolysis can be tried within the coronary ostium (Largely unpopular)
- Within the pulmonary artery for pulmonary embolism (Still considered an useful option )
It makes sense , to administer these thrombolytic agents over a prolonged period of time so that the lytic process gets wider recruitment of the natural lytic mechanisms.

When a drug is infused continuously , the drug reach the thrombus in a pulsatile manner , which facilitates thrombus dessication (Like drip irrigation ) . A long acting drug even with a high concentration may not be very effective , since the drug is required to produce a mechanical effect here . (Unlike say a long acting antibiotics !)
TPA in Pulmonary embolism
The inadequacies of 2 hour infusion of TPA is glaring in acute pulmonary embolism .We believe a 48-72 hour streptokinase infusion has a definte edge over a short and brief TPA infusion.
Issues need answer
It is yet , not understood why we can’ t infuse TPA as a long term infusion like streptokinase .
Advantage of bolus TNK TPA in pre-hospital phase of STEMI
The argument in favor of bolus dose thrombolytic agent is the ease of administration .
The other the major advantage claimed is , a 10 second TNK TPA in STEMI can substantially reduce the time window and facilitate early completion of thrombolysis .
Counter point
But , the later concept is hard to prove . . .
In fact , there are no controlled studies available for assessing the efficacy of TNK-TPA vs Streptokinase with reference to various time windows. We presume so many things. An incomplete early thrombolysis may not be better than a more successful but slightly delayed TIMI3 flow .
As scientists, when we try to answer these question we ask for data . Are we getting it any way ? Are the existing data reflect fact ? We wonder, will we may never get an hourly angiographic data base about the IRA patency in TPA bolus vs streptokinase infusion .
It is most unfortunate, with many of the critical questions still to be answered , the cardiology community believes , they have reached the summit of knowledge about thrombolytic therapy . Current perception is , the research on existing thrombolytic drugs is deemed to have been complete .
In this hyped era of interventional coronary care , it is a remote possibility to have any further comparative studies on thrombolytic agents .
The greatest threat faced by us today is the destiny of modern medicine is often decided in few corporate board rooms and hence research questions rarely emanate from bed side !
In this scenario, where we are not likely to generate genuine clinical data , the only way to move forward is to go by our experience – ” Genuine experience to be precise . . .”
Final message
Ease of administration should never be the criteria in choosing a thrombolytic agent . It can severely compromise the quality of thrombolysis ! especially in pulmonary embolism and to a certain extent in STEMI. Success rarely comes with ease . . .

Many believe , the choice between streptokinase & TPA goes much beyond it’s academic reasons. TNK TPA (Tenektepalse) has come in a big way to replace streptokinase even in developing countries. Ofcourse it is backed by a huge study ! (ASSENT) .
The cost effectiveness and worthiness of TPA over streptokinase was never proved comprehensively.
Note of caution :
The observation made above is based on personal opinion in about 20 patients . Readers are argued to do their own analysis on this issue and come to a conclusion .










{kind=link}