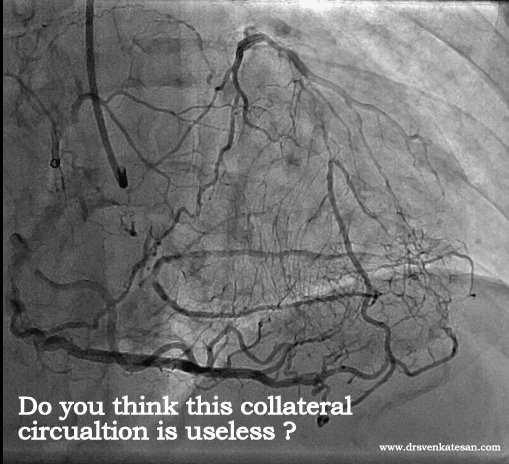
Thousands of coronary angiograms are done every day. Cardiologist no longer get excited to see exotic coronary lesions .Still , some images can be striking and dramatic. Here is an angiogram from a middle aged man with stable angina , who was one among the routine early morning diagnostic studies in our cath lab.

Who chopped the neck of this LAD ?
How this man was able to fill up the distal LAD almost completely? (With a complete cut off right in the neck of LAD )

Are you sure there is antegrade flow ?
Do you get any clue ?
- Can a trickle of ante grade flow sustain a TIMI 3 FLOW ?
- Or is it a very efficient instant collaterals from LCX ?
Yes . The first one is right . An almost invisible antegrade channel doing a exemplary job !
How is it possible ?
Realize an important fact . The distal flow beyond an obstruction is not primarily dependent on degree of obstruction but the status of the distal vascular bed . If it is normal even a hair-line patency can profusely perfuse the distal myocardial segment. This is what is happening to this man with a stable angina and perfectly normal micro vascular bed.
Lessens from this Image.
Do not get fooled by the lay man’s logic. Realise there is no simple relation between the degree of obstruction and degree of blood flow impediment.It can be linear , curvilinear , or even inverse depending upon the evolution and timing of obstruction , number of lesions , presence or absence of collateral support , finally and most importantly the integrity of microvascular bed .
The distal vascular bed drops its resistance drastically once it senses the problem in proximal segment . This is based on Bernoulli principle and is akin to how a garden hose pipe can simply increase the velocity by tightening the nozzle.*

* The garden hose analogy is a gross simplification of complex factors that determine coronary blood flow.But it effectively clarifies a point ie coronary blood flow is least dependent on coronary stenosis (until very late stages)
**Note further : This hemodynamic principle may not apply in acute occlusion as in STEMI , where acute obstruction often has a linear relationship with the quantum of blood flow.
By the way what happened to the above patient ?
Since he had significant angina there were no debates regarding management. He is posted for elective PCI this week-end .(We can’t get a stent just like that unless it is a real emergency .Ours is a Govt hospital !)
What is your take . Is it a going to be tough cross ?
I feel so , but my colleague Dr Gnanavelu strongly differs !
Let me post our experience during PCI shortly.
Read Full Post »
























{kind=link}