When half a dozen guidelines from extremely evidence based “Esteemed cardiac societies” decide to confront an Incomprehensive cardiologist , there is no other way , but to create a personalised i-Guidelines on STEMI !
*(i-Idiotic)
When half a dozen guidelines from extremely evidence based “Esteemed cardiac societies” decide to confront an Incomprehensive cardiologist , there is no other way , but to create a personalised i-Guidelines on STEMI !
*(i-Idiotic)
Posted in acute coronary syndrome, Cardiology -Interventional -PCI, Cardiology -Therapeutic dilemma, cardiology -Therapeutics, STEMI -Managment | Tagged acc esc aha guidelines scai on pci, culprit vs non culprit pci, decision cto, deferred pci, deferred ptca, delayed stemi, dilemma in stemi late presentation, how to manage 48 hour old stemi, ira pci, late presentation of stemi, late stemi, non culprit pci in stemi, Primary oci, stemi beyond 48 hours approach | Leave a Comment »
Conquering left main disease is considered as crowning glory for the Interventional cardiologists. For over three decades , CABG has remained the undisputed modality which is being challenged today. Fortunately, the Incidence of true isolated left main disease is low .(If Medina bifurcation subset is excluded)
With growing expertise , advanced hardware and Imaging ( like a 360 degree OCT fly through view ) one can virtually sit inside the left main and complete a PCI .
Still , coronary care is much . . . much . . . more than a technology in transit !
Most importantly, these complex PCIs require rigorous maintenance protocol with meticulous platelet knockout drugs , patient compliance and the genetic fate of drug efficacy . (Clopidogrel has since entered the final laps of inefficiency while Ticagrelor has some more time I guess !)
What is the current thinking about unprotected left main PCI ? Let us know it from real life experts !
For those answered , yes to the above question please leave this page , as the following question might trouble you much !
While competent surgeons are waiting to tackle left main by surgical means ,there are many centers which are Inclined towards PCI though we lack long-term outcome (At least 10 years like CABG )
Why do you think this is happening ? Are you ready for another crooked poll ?!
What exactly is left main disease ?
Some of us also suffer from a knowledge gap and tend to think Bifurcation lesions and left main disease are two distinct entities .The fact of the matter is , significant subset of bifurcation lesions are Indeed either left main equivalents or true left mains ( Medina 1,1,1 would constitute > 50 % all bifurc lesions ) If you include Invisible left main lesions in Medina ( 0,1,1 or 0,0,1 ) detected by IVUS/OCT it might reach easily cross 90% (Scientific guess !) Does that mean we have to think CABG even for all complex bifurcation lesions ? and reserve left main disease for isolated discrete mid shaft or ostial left main ?
Final message
My observation (Sincere to my limited conscience !) at least in this part of the world is : Left main Interventions are “perceived as pride” and its more related to “show of expertise” and is little to do with patient outcome.Unfortunately , cardiologists should not be blamed for it in isolation as the studies they follow are conflicted.
Forget SYNTAX/PRECOMBAT trials, the two famous studies EXCEL (Favor PCI) and NOBLE were published in 2016 made our life tough .One suggested PCI is acceptable /on par with CABG, while the other one put CABG superior , ensuring clarity replaced with confusion ! When we have a dispute , logic would suggest we should fall back on the status quo ie “CABG is superior” unless proved convincingly. Many sections of cardiology society failed to appreciate this.
Post PCI thoughts
*It may not be that hard to do a complex PCI . But, it’s never easier to understand current cardiology literature that is supposed to raise our intellect , which has a direct relevance to patient welfare. Note, many crucial , high stake studies tend to play academic deceit games with linguistic and statistical hyperboles like Non Inferior , likely superiority , Never inferior , near equipoise , regression of hazards, virtual follow-up in real vs trial world etc , etc !
I can only hope for a better scientific world !
Reference
Posted in CABG Indications, cardiac surgery, Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology wisdom, cath lab tips and tricks | Tagged best option for left main disease, left main disease, left main pci or cabg, precombat syntax nobel excel study | Leave a Comment »
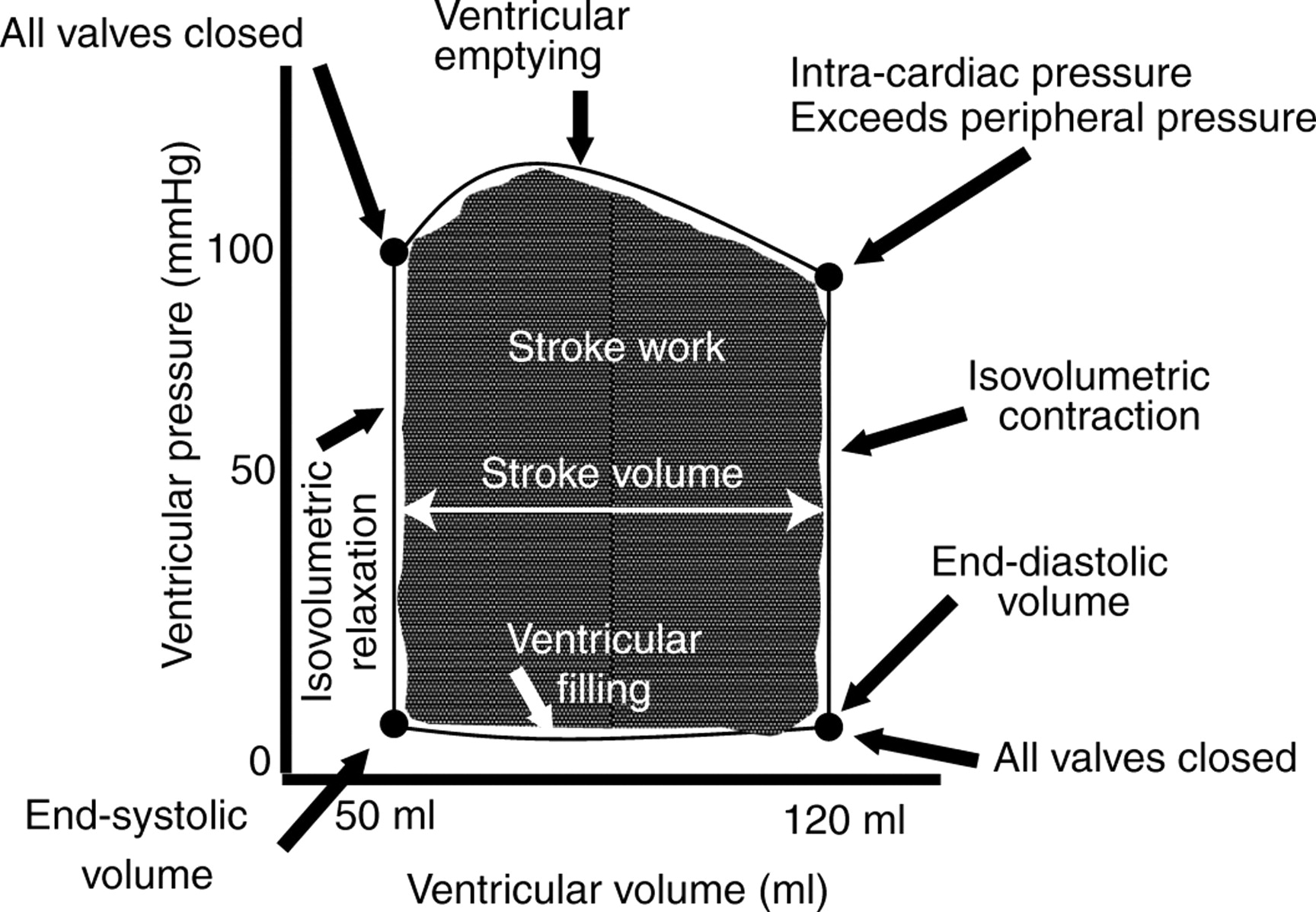
Ventricular pressure volume loop is an Important concept (often fearsome !) to learn for cardiology fellows . . . I would say , It is not that hard to understand !
These loops tell us the secret hemodynamic story of heart. Made with 300 grams of mystery muscle, the heart handles about 100 ml of blood every beat, and successfully ejects around 70 ml into Aorta and Pulmonary artery * ·
 ’
’
While doing this life sustaining job , It would seem the heart muscle conducts a perfect, non stop, hemodynamic orchestra with 4 electro-mechanically coupled phases which is depicted as classical ventricular pressure volume loop. Mind you, this loop is plotted from pressure volume data from a single heart beat and it can’t be time correlated with heart sounds or ECG as the two parameters loop around in the same time cycle.
Watch this animation , carefully and read the appearing annotation that come along with each phase.That should suffice to understand the basic. (For Audio version go the video link in the reference )
*Note: When we say PV loop it means about by LV by default . We do have seperate RV ,LA (even RA?) PV loops.
Is there clinical application for PV loops ?
It may not have any direct use , but understanding how a ventricle works in normal conditions or at distress especially during acute decompensations or after surgery is vital. With modern gadgets like LV assist devices, Impella used widely and to assess hemodynamic efficiency of transplanted (Very soon total artificial hearts) , PV loop analysis of both RV/LV will be critical.
Is there any simple Lab modality that can draw this Loop curve instantaneously ?

Very few companies make it . AdInstruments that make power lab monitors, enable us to visualise PV loops invasively .
Can we get PV loops non invasively by Echocardiography ?
Echocardiography provide us both volume and pressure data.With improving accuracy of data it should be possible to plot the loop manually with some effort. (Still , we can’t get pressure in all points of cardiac cycle )
I guess, sooner 3D volumetric machines with automated online doppler pressure data across the valves can help us draw the ultimate LV functional curve live on real time.If that happens cardiologists will be further enriched and hemodynamically enlightened !
Final message
The shape , size , timing and the slopes of this loop givs us vital info about the functional aspects of ventricle. First one should understand the normal loop , then , we can dwell on the effects of acute and chronic lesions like regurgitations, cardiomyopathy ,cardiogenic shock etc.
An excellent knwoledge base on the topic with a video
Dr. Richard E. Klabunde, PhD
Posted in Cardiology - Animations, cardiology physiology | Tagged phases of cardiac cycle, physiology of heart contraction, pressure volume loop normal, wiggers cardiac cycle | Leave a Comment »
Bernoulli principle states that , when a high pressure jet (Air, Water, blood etc ) moves over a conduit, the pressure exerted by the jet on its sides (Lateral wall) reduces . The velocity gain is equal to pressure drop .This is why we take velocity as a rough guide to pressure gradient and the sacred formula in doppler echocardiography 4V2 came in to vogue . (Incidentally, Bernoulli principle shares the same principle when aircrafts lifts from runway at its peak speed as the pressure above the wings drops to zero or negative and the plane lifts up.)
Please note , the pressure should drop both above and below the aircraft by Bernoulli principle .But, the engine and wings are arranged in such a way , the air speed below the aircraft is slower and hence the pressure is high below and low above and the lift occurs promptly at take of velocity. Imagine , how the valve leaflets in heart is subjected to lift and drag forces every time the blood gushes with high velocity flows.This is also the reason for the Pulsus bisferiens, SAM in HOCM, Coanda effect in supra valvular stenosis, and any post stenotic dilatation.
In Echocardiography the Bernoulli equation is modified.
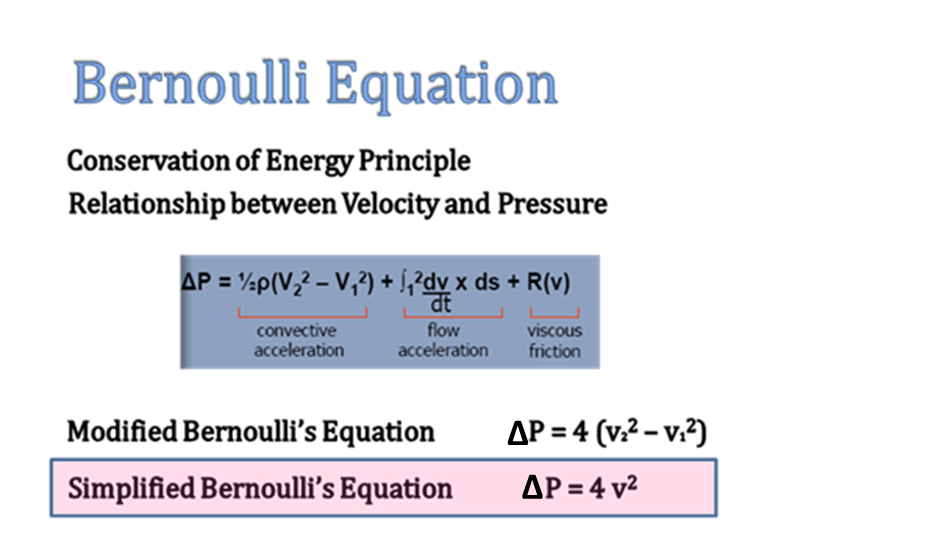
In clinical doppler echocardiography, we have liberally simplified the original Bernoulli equation by ignoring the the proximal sub valvular velocity V1 . Further , two more components in the equation is also amputated for our convenience ! (Flow acceleration and the viscous friction) .This is the reason we tend to err many times especially in outflow tract gradients and prosthetic valve gradients .
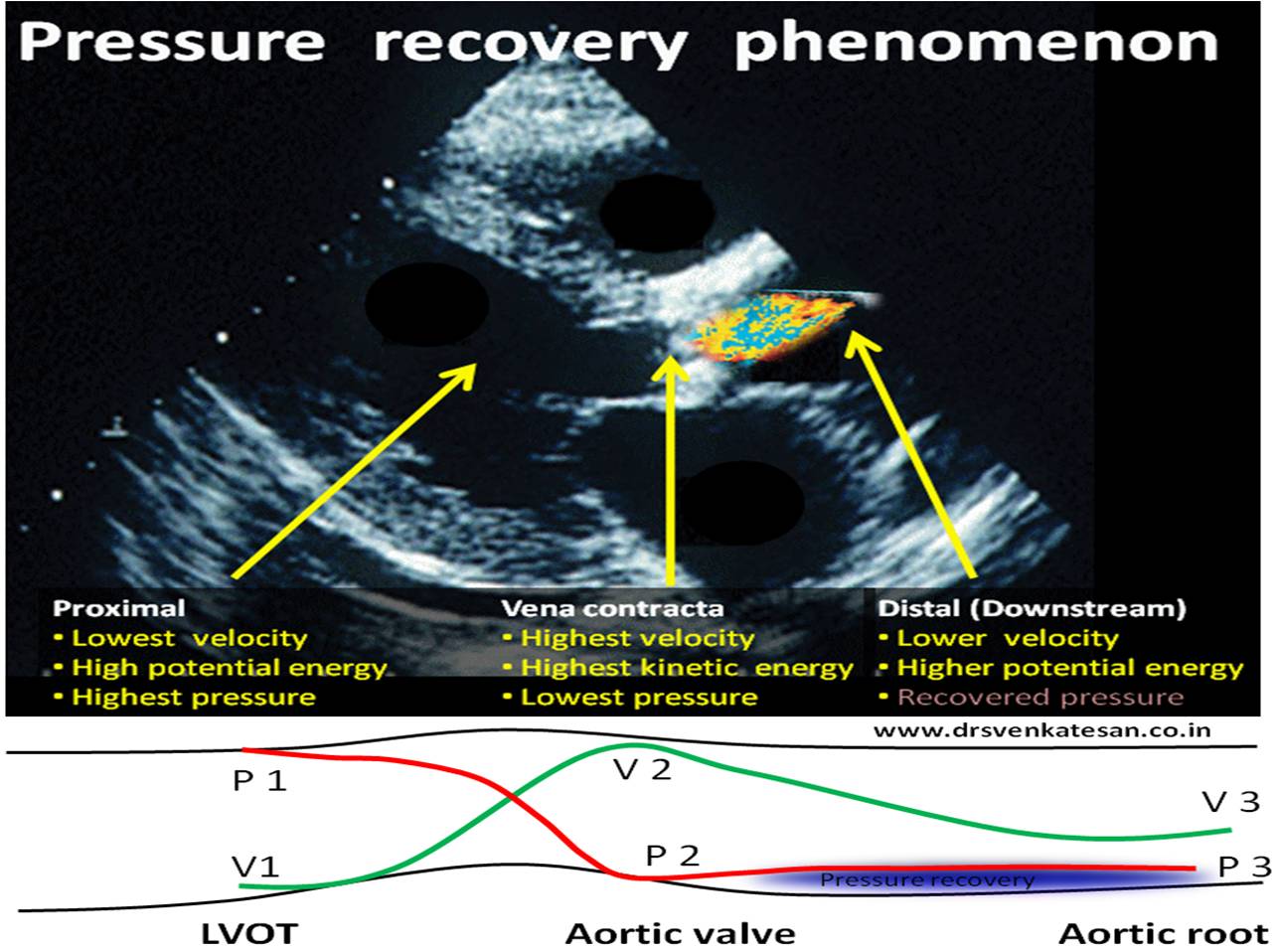
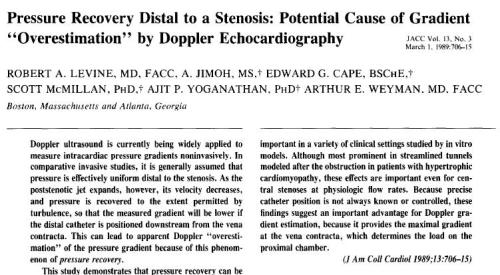
Pressure recovery phenomenon.
This is another hemodynamic lacunae in clinical echocardiography. We know, thepeak velocity of blood is attained just distal to site of obstruction. As the distal velocity beyond the obstruction begins to fall, the pressure tends to recover corresponding to the loss of velocity. This happens to certain distance beyond the obstruction. Since continuous wave doppler measures the pressure in its entire axis of alignment , it is likely to pick more pressure samples from the recovered areas and net result is, it measures more than the true difference in gradient across the valve.The phenomenon is most relevant in assessment of Aortic stenosis and results in over estimation of severity of stenosis.
Importance of Aortic root dimension
Pressure recovery is more likely to occur with small Aortic root. A stiff so be careful when interpreting echo gradients in small aorta. Relationship between size of aorta and pressure recovery is complex .(Niederberger of pressure recovery for the assessment of aortic stenosis by Doppler ultrasound. Role of aortic size, aortic valve area and direction of the stenotic jet in vitro. Circulation 1996; 94:1934–40)
How much can be the overestimation ?
It can be up to 30 % or even more.Especially in prosthetic Aortic valves.
How to recognise it and overcome it ?
Does this phenomenon happen with cath gradient ?(Generally it’s more pronounced in doppler echo )
Yes, It does happen in cath lab also , as its related to physics of flow. It can be minimised if we can use two simultaneous catheters ,one in LV and the other Aortic catheter placed very close to the leaflets.
Click below for an Animated version
Note the pressure recovers from P 2 to P3
Reference
Posted in Cardiology -unresolved questions, Cardiology-Echocardiography, Infrequently asked questions in cardiology (iFAQs) | Tagged bernoulli equation, doppler echocardiography, doppler principles, overestimation of doppler gradient by pressure recovery, pressure recovery phenomenon | 3 Comments »
Pre-op cardiac evaluation prior to non cardiac surgery is an important area for cardiology consultation . Unlike other clinical consults this one primarily involves in the delicate and tricky job of predicting future events !
 Peri-operative cardiac evaluation is done for what ?
Peri-operative cardiac evaluation is done for what ?
1.To evaluate and assess established CAD or other heart disease and get a proper pre-operative work up , drug adjustment and risk reduction for a possible peri-operative event.
2.To screen for any significant CAD or other heart diseases which is hiding and asymptomatic.
3.To treat those conditions that are detected prior to surgery .(Or simply assess & mark the risk and send them for surgery)
4.Finally and most importantly it is often done as a routine “legal point of view” or ” perceived anxiety “as litigation for missed cardiac condition looms large on the surgeon !
Risk stratifying established heart disease is relatively easy task as we know what we are talking about .The term “cardiac fitness” is used in some institution which should probably be discouraged .No patient’s cardiovascular system is deemed to be fit or unfit at any point of time.It all goes with the nature and aim of surgery .An apparently fit person can develop more complications than a potential unfit person as cardiac events are dynamic and directly influenced by the stress of surgery .
It’s about the probability of occurring possible events , and of course one should add to this , all those invincible random or remote events of Heisenberg .
How do you rule out CAD ?
A middle aged man or women with diabetes with a T wave inversion and non specific ST segment is being planned for ca-prostate or breast surgery .Both of them couldn’t do stress test due to associated OA knee.
If coronary atherosclerosis is defined as CAD , there is no way you can rule out CAD.In fact near 100% of elderly population will have evidence for CAD ( at least some degree) in the walls of the coronary .All that is required is just few minutes of heightened adrenergic drive or prolonged fall in blood pressure to trigger acute coronary syndrome in any person who may have shown even a normal coronary angiogram. How does it happen ? We have sufficient technological jargons to use in such situations endothelial dysfunction, plaque erosion erosion ,micro or macro vascular spasm coronary auto circulation failure etc ..
Is exercise stress test , Doubtamine stress , or CAG must for all persons suspected to harbor CAD ?
This could be the key question that makes most cardiologist tentative in their office .suspicion is relative and subjective term .So we have the guidelines .Guidelines are simply guidelines. It may give you comfort if you follow that either academically or legally .
Iam not convinced .Iam new gen cardiologist. Iam unable to rule out CAD without CAG , my cardiology training over a decade has never taught me to r/o CAD clinically
I will go ahead with a screening coronary angiogram in all persons in whom I suspect CAD strongly .If the patient is not willing for CAG I will do a doubtamine stress echo.
What if you detect a positive Doubtamine test or a significant multi-vessel CAD in an other asymptomatic person ?
Now you are stuck again !
How guilty are we ? If we fail to predict a cardiac event during non cardiac surgery ?
We need not feel guilty at all as long as you have done the basic tests and given your learnt opinion.I would think no court of law can plead guilty for that. (But your local reputation may be at stake !)
Final message
It is very important to realise , pre-op screening should not be a “hunting ground for CAD”.What we refer to as cardiac fitness is actually is a logical guess considering all risk factors and comorbid conditions and make a learnt decision depending upon the aim of surgery and the urgency of surgery .(Read at least once the meticulously prepared ACC guidelines of 2014)
Forbidden thoughts
In real world , it appears the task of risk stratification and pre-op evaluation is mainly driven by the fear of litigation rather than true concern about the impact of surgery on the ultimate outcome.In this gentle world of noble professionals one can’t question the true Indication of a surgery however dubious it may appear as it considered serious violation of Hippocrates oath* (Not respecting or suspecting your colleagues’s credentials !) But , I earnestly believe a genuine review of decision about surgery or procedure is to me made.
In my humble opinion , if surgery can be postponed or( if could be altogether avoided in few !) till complete cardiac stability is achieved is the most desirable option in high risk patients .
* Am I misquoting Hippocrates ?
Consider this true story . Recently a elderly women came for cardiac clearance for laproscopic Cholecystectomy . As I was doing echocardiogram the patient asked me with real concern , “Is the surgery really necessary doctor ? my doctor says its urgent “ . I casually told her since its a incidentally detected small gall stone , if its not troubling you surgery may be not be urgent , rather may be avoided. Few days went past. I don’t know whatever happened to that women , she opted out of the scheduled surgery .
Next week, , there was huge uproar from the surgeon , who called my associate and censured my behavior.He went on to add , as a cardiologist I have no business to comment about the gall bladder condition. Even if what I uttered could be truth , as a doctor you don’t have a right to breach other doctors opinion.
After few days of self deliberation , I agreed with him and realised in harsh way , freedom of expression can never be taken as granted especially in dealing with others patients !
My colleagues ridiculed my Ignorance , aren’t you aware every patient is a registered property of some doctor ? An Anesthetist friend of mine working in a corporate hospital, said If I start scrutinising the indication of surgeries I assist, I cant win my bread for my family beyond few days !
I simply couldn’t comprehend .” A patient is a patient “ What is the demarcation between my and your patient. She asked me a question I answered it to my conscience , that’s it. Should I behave like a deaf mute ?after 30 years in to medical practice !
I was still restless over the week .Finally, I decided to get the answer from Horse’s mouth and mailed the query direct to father of medicine,
To query@hippocrates.heaven
Dear Mr Hippocrates ,
Here is a story of “Fit gall bladder and an unfit surgeon” . Did I really err on that day or was my behavior unprofessional in any way as others thought ?
Yours greatly
S.Venkatesan.Physician,Chennai .India
I got a surprisingly shocking reply ,
From query@hippocrates.heaven to drvenkatesans@yahoo.co.in
Dear Dr.Venkatesan
I could feel your inner fight about the things happen in medical profession . However genuine your thoughts are, I am sorry , I say this with pain , you are largely unfit to practice medicine in the planet earth. Please try to change yourself or try changing the planet !
Learn to take things easy in life !
With regards.
Hippocrates. (Digitally signed )
Posted in perioperative risk assessment: Non cardiac surgery, Preoperative evaluation | Tagged acc aha guidelines peri operative pre operative risk fitness, cardiac fitness prior to surgery, peri operative cardiac risk assesment, preop cardiac evaluation | 4 Comments »
We know, The Mysterious Alibaba cave opens with a voice password . . . legend tell us it had unlimited hidden treasures. It would appear , CTOs mimic the cave in several ways. What is inside ? Should we open it ? Can we come out safely ? Do we have any magical password in cath lab to get across the complex tissue boulders ?, every cardiologist would love to have one !
Dear CTO,Open Sesame . . . I have come with all the wires you love ! Please let me in !
Indication
“CTOs are never an emergency . . .but please realise we can very easily create one while resuscitating a dead snake !
Don’t think hard on evidence , then , you may not do a single case of CTO in your life .Forget all those pessimistic trials like OAT,COAT, etc and the recent ones DECISION-CTO. Ignore all guidelines. Ask your patient, and his insurance company , if they are willing , reserve the cath lab and get ready.
Pre-procedure planning
Spend at least a hour to analyse the CTO Imagery one day prior and create n action plan.
Keep knowledgeable staff for assisting , but never ask for fellow colleagues help because it hurts our ego ! Cardiac surgeon’s back up is a welcome addition even if it’s on paper.
If possible , try to ask the patient genuinely ,what is his symptom at least once ! before starting the procedure.
Timing of the procedure.
Don’t post a CTO patient either on a busy Monday morning or lazy Friday afternoon.
Hardware Inventory
The wires ,catheters, the balloons form the essential tool box .There is more than a handful of coronary automobile companies manufacture this .It is all about metallurgy , knowledge of wires, catheters , and tip thickness, (Bullet shaped as in Asahi ) , slipping , hydrophophic or philic, polymer coating , trackability, pushability , memory etc etc.
Guide wire tip morphology is as Important as the Lesion characteristics !
Analysis of the lesion (Probably most important)
Unlike conventional PCI we have no initial target.We need to poke first and find the target next ! Distal vessel status is most important ( Careful review of retrograde filling through collaterals could give more information than CT angiograms .Calcification, diffuse disease can be a real hurdle)
Lesion morphology
Softness of lesion has to be felt (Requires good wire which has sensor (Paccinian corpuscles and Merckle disc ideal ?) I guess the cortical tactile feel is as vital as the intervention expertise .I know at least one diabetic colleague of mine who finds it difficult to cross a CTO and admits he never found it easy to feel the lesion through the wires . Autonomic dysfunction ?)
Operator expertise
(Note: These are like reading swimming guidelines , you can’t learn in the shores reading books ! you have to plunge !)
Many techniques are proposed .Sequential approach (Ironically experts are licensed to use specialized wired wires directly .Beginners are advised to go with non specialized hardware and escalate step by step) Some centers are blessed with new age weapons like cross Boss and sting ray that confront the lesions in multiple frontiers. (Carpet bombing?)
CTO playground. : Its essentially a coronary contact sport with expert septal surfing , tunnelling, knuckling , kneeling , bending . Of course , It can end up in a gratifying win in few , still most of us tend to play this game without a goal (post !) Source of the Image : Unknown Due credits to the creator.
They are basically about poking the head of the lesion and trying to cross an occluded vessel millimeter by mm towards the presumed distal vessel in an Imaginary trajectory. Proximal cap, central core ,the blind tunnel , distal capsule and exit points each must be successfully conquered.
CTO crossing is the ultimate capacity of the operator to realise and feel the position of the wires in true lumen and their confidence levels in their conviction!
Multiple wires up to three are used some times to poke the lesion two of them are used to shut the false tracks and the other one is expected to enter the true lumen (Looks too good on theory !) . These are referred to in as many terms like parallel wire see-saw , CART ,Reverse CART etc .Retrograde techniques do help us but has no magic solutions.The lumen contrast , guide wire tip movement and its side branch entry would help.
Tacking complication :Always anticipate , it’s not negative mind set to look for it !
Keep pericardiocentesis kit , covered stents , micro snares and other retrieval devices ready in cart. Your support staff should be well versed with what is happening around them. Some of the dye leaks and stains are safe .They imply minor perforations that form sealed hematomas (The plane of perforations also matters. myocardial (ab-pericardial ) leaks are well tolerated .Distal perforations are also safe as long as CTO is not opened ) Online echocardiography should be readily available to monitor pericardial space leak.
When bleed into pericardial space is life threatening , A comical, but life saving option is to close the artery and restore the CTO its original state and come out of the lab quietly !
Newer Imaging guidance : Can be useful , still may not matter much when considering the interventional acumen .
CTO PCI : Time as therapeutic end point.
CTO is not an endless game with out time frame .In my opinion it shouldn’t cross 45 minutes each as in a soccer game with a brief strategic time out and of course with liberal use of ,yellow and red cards
Future directions
Japanese are the ones who pioneered CTO Interventions . We expect more Innovations ! Is it the forward looking IVUS ? It is akin to tunneling for underground metro train with GPS guiding .If you can mark the proximal and distal points , rest will be be taken care by mortised self tunneling catheters from Robotic arms steered by sophisticated algorithms.
Final message
CTO PCI remains a real Interventional challenge. We are often double blinded in both directions (antegrade as well as retrograde ). Needs much effort ,time, hardware and most importantly a non fatigued mind and body. The benefits we get may vary between gratifying to outright mediocre .Of course , it surely satisfies operator ego and express pride and courage !
Is crossing and stenting a CTO synonymous with true success ?
Yes it is , for the cardiologist and the hospital . . . I’m not sure about it for the patient !
In this sense , CTOs mimic the mysterious Alibaba cave that tempts us with Imaginary treasures but can trap us with a wrong password !
Post-Ample
* Who should CTO PCI ?
I have seen young , enthusiastic cardiologists with Immature support staff attempting CTO in remote sub- urban settings ! Though patience and expertise are essential ingredients, some amount of organised training and hardwares make CTO PCI safe and effective. Enthusiasm and affordability alone can’t be an Indication for this complex set of coronary lesions.
Reference

I still wonder why this vital paper was never published , it was just presented in the Annual ACC conference March 2017
Posted in cardiology -Therapeutics, Cath lab Hardware, cath lab tips and tricks, cto chronic total occlusion | Tagged absolute refractory period, Best guideline on cto pci, cart reverse cart, chronic total occlsuion, cross boss sting ray, cto club, CTO club euro, cto euro club, cto japan club, cto mmc chennai madras medical college, decision cto trial drsvenkatesan, dr s venkatesan, ethical guidelines in cardiology, ethical issues in cto, management strategies in chronic total occlusion, see saw technique, tips and tricks for cto opening | Leave a Comment »
One big hypertension trial called SPRINT was published in 2015, has caused major delayed aftershocks in the hypertensive world now in 2017.
The new guidelines by 2017 AHA/ACC is based primarily on SPRINT data which in my opinion has so much flaws it shouldn’t have been accepted for publication in the first place. !(Intentions and Aim of a study can never be questioned even by most prestigious journals you know !)
The ultimate spoiler in SPRINT
The modality of BP measurement in SPRINT trial can be termed as as a single fit case for rejecting the study in the world hemodynamic court !
We know BP is a continuous variable, between machines , timing of measurement, persons who measure , hand to hand , beat to beat variation etc etc. The SPRINT BP data was accrued high-profile “Research standard BP” measured by oscillometry method. Please hold your breath , . . these machines never measure either systolic or diastolic BP.It detects the peak oscillations from brachial artery when the cuff is deflated and ask the vendor dependent fuzzy logic algorithm to do a guess work of SBP and DBP , which proudly flashes them in various LED colors.
The jury is still out whether the methodology is validated or not. SPRINT data should be thoroughly sanitized with a true clinic BP which would virtually mean , recall of this (de) famed study !
Final message
How can such a flawed study be taken as reference for creating major revision of Hypertension guidelines?
This question is to be asked in chorus by all respectable physicians and cardiologists.The World health organisation -WHO , custodian of human health and the silent watch “puppy” has more work to do ! . . please WHO , wake up and bark !

Reference
2.http://www.acc.org/latest-in-cardiology/articles/2015/12/01/10/04/the-sprint-trial-cons
3.http://www.cardiobrief.org/2017/02/08/new-questions-raised-about-sprint/
Posted in Ethics in Medicine, hyperlipidemia, wisdom in cardiology | Tagged acc aha 2017 american hypertension society, SPRINT trial | 2 Comments »
Posted in Cardiology -guidelines, cardiology -Therapeutics, cardiology journals | Tagged EARLY MYO trial circulation, ppci vs thrombolysis, primary PCI vs thrombolysis, stream trial | 3 Comments »
The age old statistics , 30 % of deaths following STEMI happen even before patients reach the hospital may still be true. But ,there is an untold story that happen regularly in the rehabilitation phase .Its ironical many apparently stabilised STEMI patients still lose their life just before they get discharged or within 30 days .More often than not this happens in the toilet when they strain for defecation. At least a dozen deaths I have witnessed in the last few years. Of course we have resuscitated many near deaths as well.
What exactly happens to these ill-fated patients inside the toilet ?
Straining is often an isometric exercise and prolonged strain ends up in valsalva maneuver , a prolonged valsalva strain realistically shuts both vena cava due to raised intrathoracic pressure .Vena caval shutdown is equivalent to asystole and imagine the chaos in the delicately recannalised LAD when the coronary perfusion pressure nose dives (Even the stented segment in IRA is vulnerable as distal flow restoration may take time !)
The sudden systemic hypotension leads to fall in coronary arterial pressure proximal to the lesion. The normal physiological response to proximal fall would be corresponding distal fall maintaining the flow gradient . If the microvascular bed is damaged( loss of capacity to vasodilate ) this distal fall may not happen promptly .So its acute standstill of flow across IRA ( or even Non IRA if it has a lesion ) triggering events that rapidly destabilise unless intervened.
.
Other modes of sudden toilet deaths
*The opposite process , ie sudden spikes of blood pressure (In contrast to hypotension of Valsalva strain ) can occur as straining is equivalent to Isometric exercise which increase afterload .This can either cause LV failure, another episode of ACS, myocardial stretching, even tear it and result in mechanical complication.
How to anticipate and prevent these deaths ?
Has primary PCI has reduced the sudden deaths in Post MI period in current era ?
I’m afraid , I can’t say a dogmatic yes . May be ,to a certain extent , However, it has created a new subset of perfectly stented still prone for ACS.A physiologically or pharmacologically recannlised IRA generally heals by themself. A Stented IRA hands over the responsiblity of healing the injured IRA to us .Ofcourse ,we try to do it with lot of difficulty .(Different versions of confused DAPT regimens !)
Final message
Please note , “discharge to 30 day mortality” following STEMI which is upto 2 % .It is the most neglected and mismanaged phase in coronary care .Toilets are definitely not a benign place for them and all the good work done by you in cath lab and CCU can be nullified in few Innocuous looking seconds !
Postamble
Is Toilet room death amounts to negligence / mis-management inside hospital ?
May be there is a reason for this argument. When to ambulate in complicated STEMI is a big question. ? Though we have guidelines some of the patients are reluctant to use assisted service.
I think its a calculated risk , and there is trade off between the benefits of early ambulation and potential exertion related risk.
One such argument by a cardiologist in a medicolegal situation goes like this. “I thought my patient’s heart is stable enough to use toilet , it misfired , hence it is just an error of judgment. I can’t be faulted. Though this argument appear logical , many times it can’t hold water in court of law !”
Further reading
Cardiac rehabilitation NICE guidelines : Myocardial infarction: cardiac rehabilitation and prevention of further cardiovascular disease 2013
Posted in acute coroanry syndrome, Cardiology -Interventional -PCI, cardiology -Preventive, Cardiology -unresolved questions | Tagged acs, hemodynamics in LAD following valsalva, predischarge stress test, primary pci, stemi, Sudden cardaic deaths in bath room toilet, valsalva vs squatting | 1 Comment »
If human coronary artery is comparable to live wire , attempting bifurcation (BFL) stenting is akin to tame a live snake .True BFL (with Medina 1, 1, 1) being the most complex of all .The fact is ,we have atleast a dozen strategies for BFL with varying loads of metal abutting the ostia ,side branch and carina.This would essentially Imply we are still struggling with these lesions .
Who should do complex PCI ?
Obviously, not every interventional cardiologist can. Confidence is one thing , but , falling short of minimum standard of care is rampant in India. Newer Imaging tools, techniques are promising , unfortunately still the gap between, knowledge , science and reality continue to widen.
* Its true ,some expert Interventionists do a good job !
This was posted almost 10 years ago , much of it might hold good even today. https://drsvenkatesan.com/2008/09/06/what-is-the-simple-approach-to-bifurcation-pci/
Final message
We have come a long way in BFL. Still , some of the lesions can sting like a snake ! I am sure, everyone of us would have lost sleep after a complex BFL PCI !( Praying the humble heparin and DAPT to do the rescue act ! )
How to escape this double headed threat ?
A meticulous assessment of patient & lesion , mindfulness in choosing the hardware & Imaging , diligent usage of anticoagulants & DAPT and . . . finally willingness to listen to your own conscience , will ensure a gratifying result that includes abandoning the procedure !
Reference
Posted in bifurcation pci, Cardiology -Interventional -PCI, Cardiology -unresolved questions, Tips and tricks in cath lab | Tagged bbc 2 study, bifurcation lesion, dapt after bifurcation stenting, european bifurcation club, Proximal optimisation pot, single vs double stent strategy, SKS DK CRUSH, strategies for bifurcation lesions, v y t stenting medina classification, what is pot technique | Leave a Comment »




{kind=link}