
Distribution of Left main disease.
- Ostial
- Ostio-proximal (Within 1 cm of origin )
- Shaft -Discrete mid left main
- Shaft -Diffuse
- Isolated distal shaft( 1.0.0)
- Bifurcation ( Medina 1.1.0 -LAD)*
- Bifurcation (Median 1.1.0-LCX)
- Bifurcation ( Median 1.1.1)*
- Trifurcation ( With ramus )
* These three locations account for nearly 75% of all left main lesions.
We know atherosclerosis is a branch point disease .Normal left main measures 1 mm to 20mm.The shorter the left main lesser is the the incidence of LMD. Short left main can not engage the atherosclerosis much (No left main = No left main disease ) However ,very short left mains may increase ostial lesions .
- The commonest left main lesion is distal left main with one of the branch involvement (1.1.0.LAD is more common )
- Least common entity is discrete mid shaft lesion.
Simple strategy.
First dictum : All complex looking LMDs should be referred to a good surgeon.
Final dictum : Remember medical management for left main disease is still an accepted strategy in stable , non flow limiting situations .
Interventional Cardiologists feel they have the exclusive rights to indulge between these two spectrum of LMD .May be true! But extreme caution is required as we are playing our game in the most critical coronary high way .
Some suggestions and thoughts.
- 50 % diameter stenosis is significant. But significance does not mean we should tackle the lesion by aggression.
- Symptomatic flow limiting lesion only to be intervened . (Flow limiting means both angiographic and a stress test .FFR <.8 is also an index for flow limiting .Symptom means Angina on exertion )
- IVUS, OCT, FFR,NIR ,SYNTAX are not path breaking tools .They essentially add more glamor to left main disease than anything .
- Most bifurcation LMDs are managed by single stent with stent jailing the major side branch (Yes side branch can be LCX !)
- However ,two stent strategies is not banished .It can be vastly superior in some selected cases .(Especially with huge plaque load at carina )But needs expertise .
- In very small vessels two stent strategies are risky .
Reference (2012 update)


Link to related articles in this site
Posted in Cardiology -Interventional -PCI, Cardiology -unresolved questions, Left main disease | Tagged classification of left main disease, left main artery imaging, left main disease, medina classification, short vs long left main | Leave a Comment »
We know Nitroglycerine(NTG) as a most powerful epicardial coronary dilator . We use it for instant relief during episodes of coronary arterial spasm in cath lab.
What will happen if we administer NTG over a stented segment ?
Does it dilate it with same vigor ? What will be the consequence ?
A perfect setting for stent migration isn’t ?
Let us bust the myth around NTG . NTG rarely show visible coronary dilating effect except in the setting of coronary spasm .

Does a LAD with 3 mm diameter become 3.1 or 3.2 and so on with NTG ?
No .It won’t .It is my belief. It is well known , NTG’s action varies significantly in normal and diseased endothelium . Again , there is an irony .It seems , it can act only in normal endothelium , but we need require it’s therapeutic action only in pathological segments.Further any stented segment would contain clusters of both normal and abnormal endothelium .
One more inference is that, stented segment exerts constant pressure on intima making any pharmacological vasodilatation irrelevant .
Importance of radial strength of a stent
This issue of vaso-dilator induced stent migration may not arise in self expanding wall stent with high radial force.But we do not know how long these metals will carry this metallic property .Balloon delivered stents ( currently used 99% of times ) do not have permanent radial strength .
Final message
I am yet to comprehend what nitrates are expected to do (and what it really does ?) in a patient post PCI ? (By the way . . . why we need to prescribe Nitrates it in the first place ? but In real world most continue to take this for many reasons .)
We need to analyse the micro-vasomotion at the stent -coronary intimal interface.The dynamism in this narrow space can be critical , and may make the difference between life and death !
After thought .
In the hind sight, this post appears quixotic for myself . But some one , some where , may generate a great idea out of it , that will help our patients.
Posted in Cardiology -Mechnisms of disease, Cardiology -unresolved questions, Cardiology research topics, Infrequently asked questions in cardiology (iFAQs) | Tagged coronary spasm and ntg, epicardial coronary vasodilation, factors determining stent migration, nitrate action in normal and diseased endothelium, nitrate action in stented segment, nitric oxide and ntg action, nitroglycerine, stent coronary artery interface, stent dislodgement by ntg ?, stent migration | 1 Comment »
Today , November 2nd 2013 is Deepawali , Nearly 1 billion people celebrate it

Wishing you all happy and Deepawali , Let goodness and wisdom prevail over evil and Ignorance !
Deepawali is an ancient festival of lights , millions of Hindus celebrate It with sanctity.
It is a war on darkness and ignorance .On this day goodness prevailed over evil (Asura)
Unfortunately , In the current versions , it would seem Asura’s also join Deepawali celebrations and enjoy it with more vigor ! which is supposed to eliminate them !
Please ensure , that doesn’t happen . . . at least in your domain !
God is supreme . . . he will never allow the evil to take over the world ! Be a soldier to God’s Army !
*For more about this great Hindu festival click on the Link here Deepawali
Posted in Quotes, Science and Religion, Venkat quotes | Tagged Deepawali, ethics in medicine, festival of lights, hippocrates | 1 Comment »
CAD is growing as an epidemic in most parts of the globe. It is a major determinant of health status of any country .Great strides in diagnostic, treatment modalities of CAD have been made in the last few decades. Still , the core principle of management of CAD resides in simple things like risk factor reduction / optimization , life style changes and few essential cardio-protective medications Aspirin, beta blockers and statins.
However , modern scientists have made a firm statement that knowing the coronary anatomy before starting the treatment is the only scientific approach . It is a huge assumption !
Is it practical ? or is it really required ?
CAD can be managed by means of medicines , interventions or surgery. Revascularisation is required only for those , who have critical , symptomatic lesions.
It is estimated , in only a fraction of CAD patients , we would require to know the anatomy . We have set criteria to choose patients for CAG , who are likely to have critical lesions.Physicians are trained for that elusive wisdom to choose such patients .Standard text books do mention clear-cut Indications for doing CAGs. Unfortunately , it is least respected and followed .
Cardiac physicians who would boast they can’t treat a CAD without knowing the coronary anatomy are clinically handicapped or poorly trained.
I am afraid such a class of cardiologists are rapidly breeding in the country side. They are encouraged to attend CME on clinical cardiology and basic principles of clinical decision-making .
We can’t keep on doing CAGs like ECG for every episode of angina . In fact treating CAD without knowing the anatomy remains (And it should be ) the dominant theme contemporary clinical practice . CAG is multi -edged sword
The most important side effect of routine coronary angiogram is , it ends up in infinite number of inappropriate interventions !
I think , we should pray in Hippocratic temples for sufficient wisdom to choose our patients. We can also learn it from Neurologists , they somehow manage most forms of cerebrovascular diseases (scientifically too ! ) without asking for angiogram of circle of Willis ! Mind you. . . brain is equally a vital organ !
Final message
It needn’t be a crime to treat CAD* without knowing the coronary anatomy. Rather . . . it would be so , to ask for CAG indiscriminately , in every episode of chest pain , without applying clinical sense !
* Emergencies included.
Posted in Cardiology -Interventional -PCI, cath lab tips and tricks, Infrequently asked questions in cardiology (iFAQs), Venkat quotes | Tagged acc/aha criteria for coronary angiogram, appropriate coronary angiogram, can we manage cad without coronary angiogram ?, cardiologist behaviour, coronary angiogram in chronic stable angina, ethics in cardiology, hippocrtes, inappropriate coronary angiogram, Indication for coronary angiogram, indications for coronary angiogram, waht is the indication for coronary angiogram ?, what is inappropriate coronary angiogram ?, when do you do coronary angiogram ? | Leave a Comment »
News : In any developed nation , 90 % of total health expenditure is exhausted in prolonging final few days of human life !
When cost of dying . . . exceeds cost of living . . . this world will go nuts !
The current real world experience from India’s five star hospitals indicate, many elderly rich men and women spend their last few days before being buried or burnt .They spent an average of 15 lakh Rs per death . This amounts to the entire “life time” cost of living of majority of Indians .
Image courtesy from Flicker/ Rachel sian photostream
When human organ donation is considered a greatest philanthropic act, there is one more excellent alternative for those who can’t do it .If only every super rich translate their cost of dying into cost of others living ! many new lives will bloom .
The exorbitant rise in cost of dying in India , is a recent development and reflects the affluence , honor , pride and of course lots of prejudice lack of wisdom ! Instead of filling the deep pockets of greedy corporates why not the rich add new lives ? !
Final message
Let all elders with irreversible conditions , who have finished their life , shall die peacefully at home .Why don’t we ( Affluent . . . would be cadavers !) cross sponsor their dying cost to a public health , nutrition or medical fund .
After thought
Oh America , . . . Am I right ,? Obama thought it and implementing it too ! I would believe , his health care policy is a small first step in this direction !
Posted in Cardiology classics, cardiology-ethics, Cardiology-Statistics, general medicine, Quotes, Social medicine, Venkat quotes, Wintage cardiology | Tagged affluent vs poor health care, cost of living, crude detah rate, do not resucitate dnr, ethics in medicine, health budget, health care priorities, health economics, health expenditure gdp, health insurance, health management, health policy for the future, hippocrates, inappropriate health care delivery, mercy killing, obamacare, primary health care, private vs public health care, sharing medical resources, terminal illness, tertiary health care, who world health organisation, withdrawl of life support, world food program wfo | Leave a Comment »
We know LVH and SHT go together . Mind you , this is not an Intimate relationship.
Widespread utilisation of echocardiography has revealed , definite LVH occurs only in about 20% (A guess !) of HT . (Do you know in the Famingham study the incidence of LVH after 12 year follow up was a paltry 3 % .Will you agree with that ? Mind you , It was in 1969 when Echo was not there )
What determines LVH ? The clear answer is elusive. It is easy to escape from the issue by calling it multi factorial !
Why don’t you try this question .
My guess would be , magnitude ( or even duration of HT !) is less important than genetic predisposition or associated diabetes , renal involvement.Our analysis from hypertension clinic reveals LVH is many fold common in secondary HT when compared to primary HT !
I often used to provoke the students by saying if the LVH is gross in HT it can not be primary , 9/10 times ! Invariably we find some other association or reason for the HT !
Link to related topic in this site
Why-lvh-does-not-occur-in-all-patients-with-systemic-hypertension ?
How-diabetes-modifies-lvh-due-to-hypertension ?

Next . . .
How does LVH regress with treatment ?
Posted in Cardiology -Mechnisms of disease, Cardiology -unresolved questions, Clinical cardiology, Hypertension, Infrequently asked questions in cardiology (iFAQs) | Tagged determinants of lvh in hypertension, genetic factors in LVH, left ventricular hypertrophy, lvh, mechanism of lvh in hypertension, sht, systemic hypertension | Leave a Comment »
The current fad called EBM has lots of lacunae. Though evidence based approach is considered the ultimate journey towards truth ,lot of non academic factors contaminate it .In it’s current form , it is difficult to comprehend it.
This is an attempt to decode the mystery of EBM expressed in a simplified lay person’s term .They are the ones from whom we learn medicine. They are our teachers in the true sense.
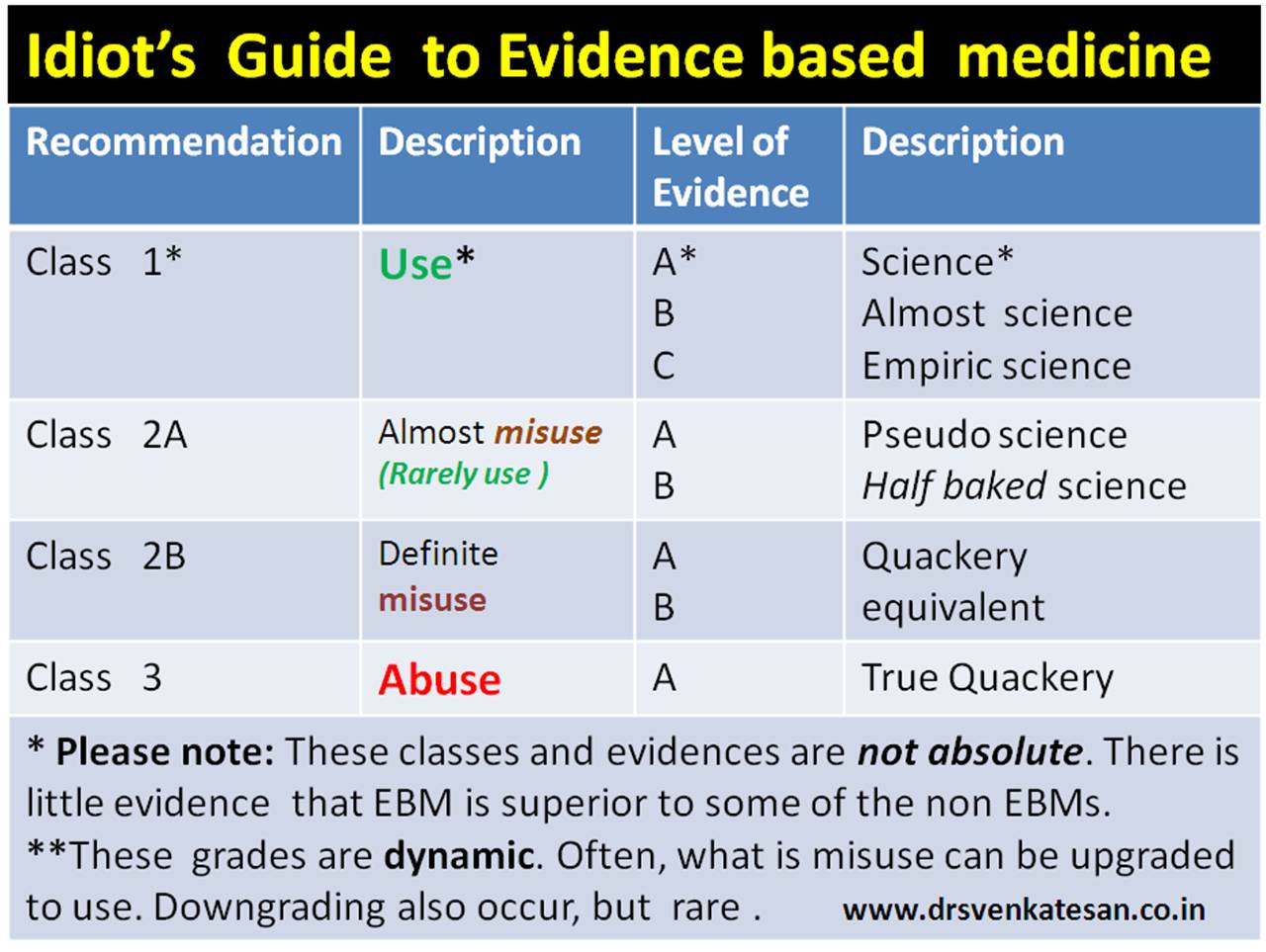 By the way ,it is also my approach to EBM .Sorry , if this post sounds arrogant ! It is not the intention .Truths often times appear brutal .
By the way ,it is also my approach to EBM .Sorry , if this post sounds arrogant ! It is not the intention .Truths often times appear brutal .
And . . . the Genius approach to EBM for comparison

Posted in bio ethics, cardiology journal club, Cardiology quotes | Tagged ethics in cardiology, ethics in medicine, evidence based cardiology, guidelines in cardiology, guidelines in medicine, principles of medicine | Leave a Comment »
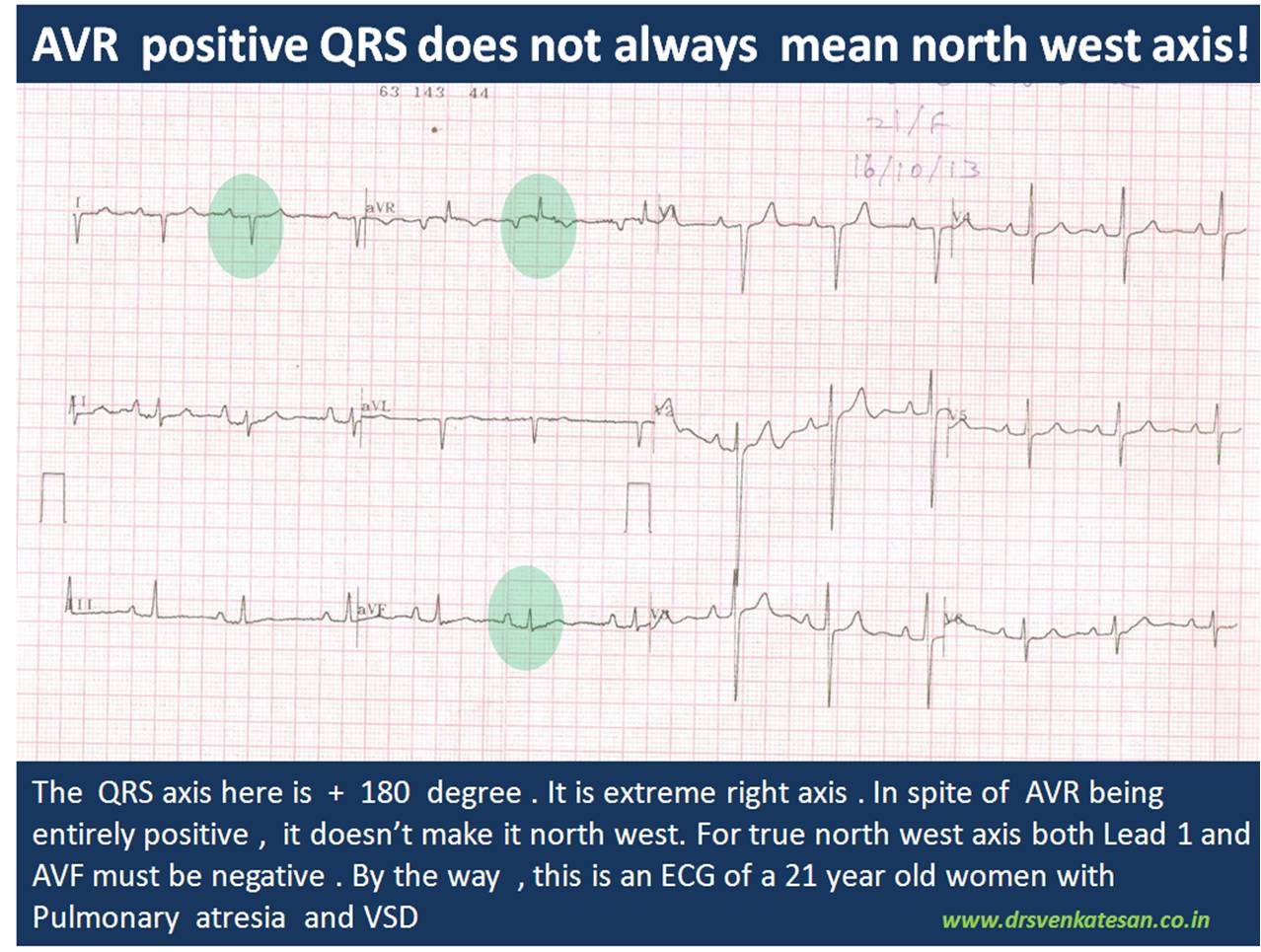
In one of my classes , this ECG was presented . Controversy erupted.It was about the basics .
What is the QRS axis of this ECG ?
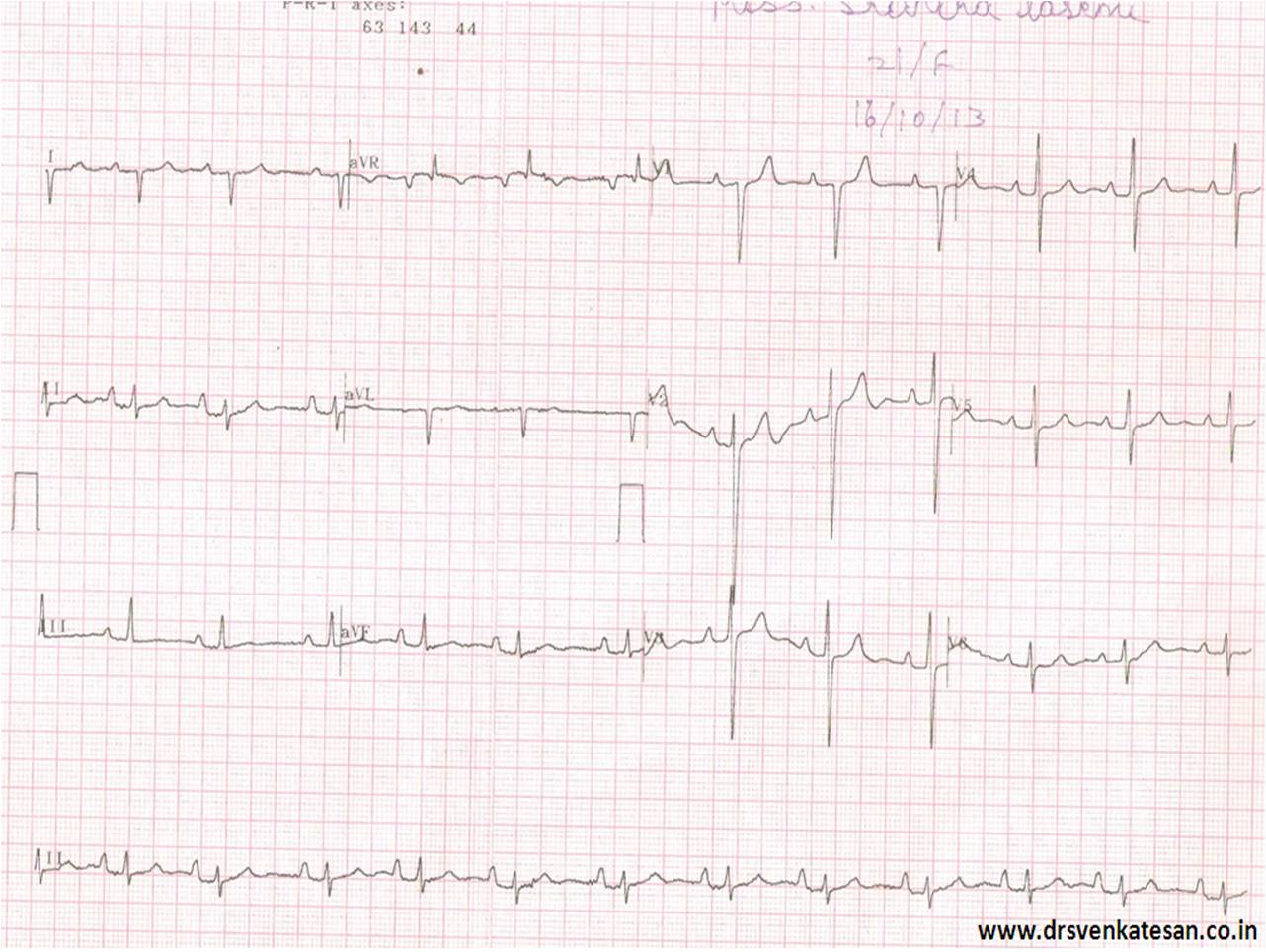
Not surprisingly there were handful of answers .
- North west Axis
- Indeterminate QRS
- +150
- +180
- 0 degrees
- Extreme Right axis
Which is correct ? My guess is , it should be closer to + 180 . Lead 2 is equiphasic and perpendicular lead is negative limb of AVL ie + 150 .If you plot Lead 1 and AVF in graph and calculate we get + 135 . (In the strict sense , we are not supposed to take one standard lead and an augmented lead for plotting ). Finally, the strongest argument was , since AVR shows only positive forces it would make north west axis more likely .
Causes of North west QRS axis
- Denova North west axis
- Extreme Left becoming NWA*
- Extreme Right becoming NWA
*Left becoming NWA is much more common than other types.
Chamber enlargement alone is not sufficient to shift the axis to NW corridor. There must be anatomical distortion of his bundle and it’s branches to shift the axis dramatically .This usually occur in complex congenital heart disease. In acquired heart disease the an apical VT is probably an important cause for NWA.
One word about indeterminate qrs axis .
By the way , Indeterminate QRS axis is not synonymous with north west axis. This term should ideally be used if qrs complex is equiphasic in all limb leads , when qrs axis can not be truly determined .This situation commonly occurs when we encounter very very low voltage qrs as in cardiac tamponade and severe hypothyroidism , constrictive pericardits, etc
If the QRS is in north west corrodor , How to differentiate , whether it came from extreme left axis or right axis ?
I am yet to find a correct answer for this.
- Pre-cardial pattern will help.
- A q in V5/V6 would suggest extreme left axis.
- May be we have to look the initial qrs vector in AVR lead for more clues
Traditionally , we talk about net qrs axis . We should realise net qrs axis is a combination of initial and late vectors .It can be dramatically different in different leads . QRS axis is a two dimensional representation of three or more (omni) dimensional electrical forces .That is the source for confusion. So, do not unduly worry about the complexity .Blame it on the limitations of surface ECG !
Expecting some comments .
Posted in cardiology -ECG, Infrequently asked questions in cardiology (iFAQs) | Tagged ecg in pulmoanry atresia, extreme left and right axis, indeterminate qrs axis north west axis, what is north west qrs axis ? | 1 Comment »
It is estimated nearly half a million PCIs are done all over the globe every year .Evaluating diagnostic angiogram is a critical vital step, but often times it is given less time and left to fellows .This is done mostly offline by Image processing software. Curiously , lesion assessment becomes a causality to the visual acuity .It ends up with lot of whims , intuition and bloated egos of senior cardiologists !
Technical issues
The fundamental flaw in the lesion assessment is ,there is a dissociation in choosing the “best view” for lesion morphology and length . Size need not be well assessed in the same view as morphology . For example , LAD is fore shortened in LAO caudal view , length measurement would be erroneous , still morphology may be well delineated .(Vice versa in RAO caudal view )
Other source of errors
Reference catheter may be far away in the Aorta , and confer a magnification error . This becomes important especially in ostial lesions and associated major branch lesions. The computer uses the edge detection algorithm which carries an inherent error .
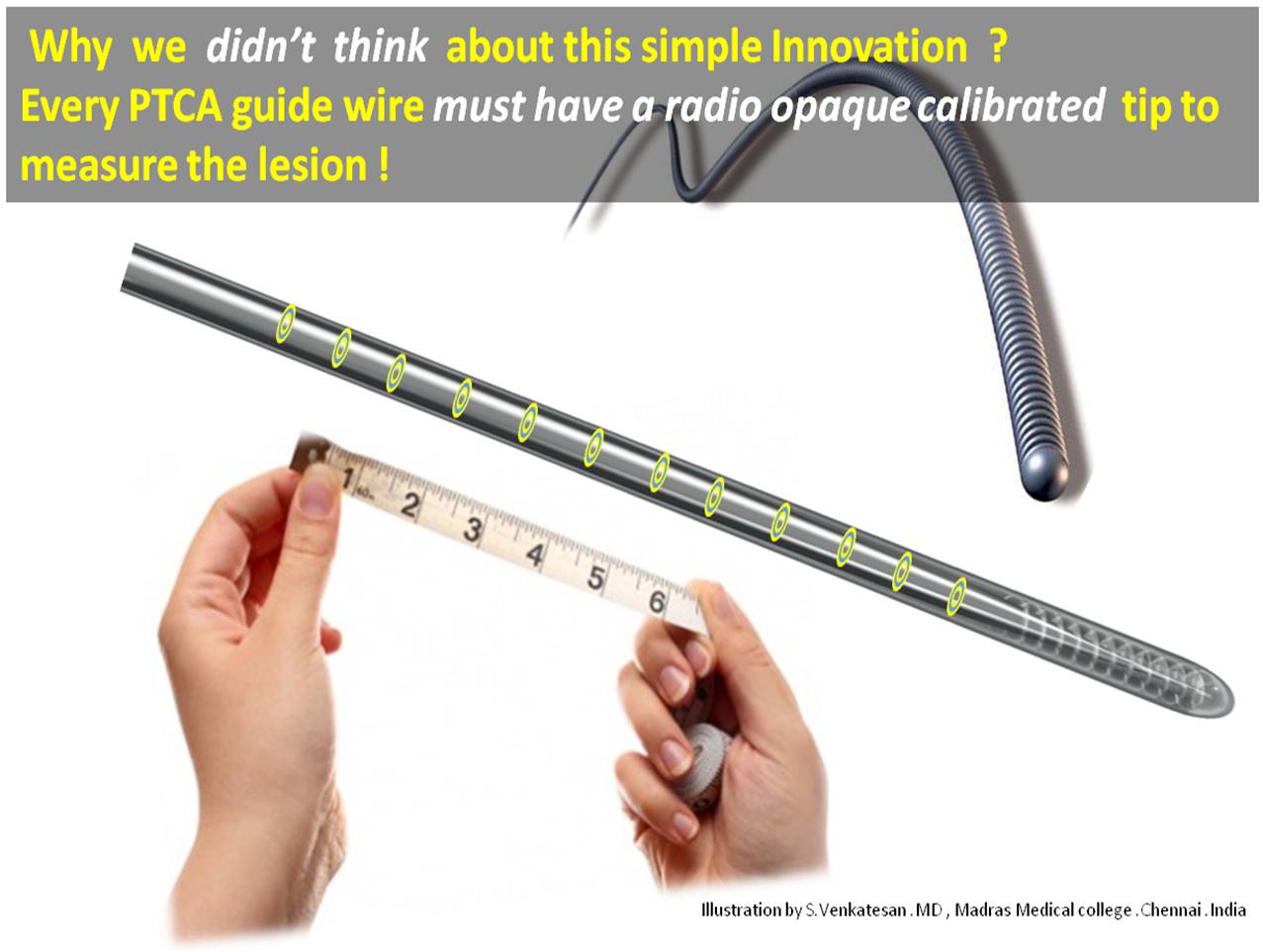
Advantage of guide wire as a scale
- Instant online measurement
- Always on . Repeatedly used in multiple views .
- You can’t ask for more accuracy .The scale is within the coronary artery hugging the lesion
- The end on view is effectively nullified .
- Magnification factor do not operate.
- Finally , and most importantly in complex tortuous , tandem lesions few mm errors can be disastrous .These calibrated guide wires will make our life lot easier.
Final message
Measuring a coronary lesion remains a delicate issue . If only we have radio opaque rings every 1mm or so in the distal end of the guide wire , we can measure the lesion instantly and most accurately.
This will definitely make our life not only simple but help our patients with accurate stent sizing and avoid costly geographical miss (or inappropriately long stent that increase metal load .)
After thought
I do not know whether any of the existing guide wires have this facility .(I guess it is not . . .then , let this idea be patented in my name !) After all , It is a mean task for all those mighty coronary hardware companies to add few radio opaque rings to all PTCA guide wires!
Medtronic, Abbot, Boston are you listening ?
And . . . your opinion please !
Posted in Cardiology -Interventional -PCI, carotid interventions | Tagged calibrated guidewires, coronary stenting, lesion length assessment, morphology of lesion in ptca | Leave a Comment »
Categories
-

-
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book
https://amzn.in/d/euhL5vu Archives
- June 2026 (1)
- May 2026 (6)
- April 2026 (11)
- March 2026 (10)
- February 2026 (8)
- January 2026 (8)
- December 2025 (11)
- November 2025 (7)
- October 2025 (8)
- September 2025 (7)
- August 2025 (9)
- July 2025 (10)
- June 2025 (8)
- May 2025 (9)
- April 2025 (7)
- March 2025 (10)
- February 2025 (4)
- January 2025 (9)
- December 2024 (11)
- November 2024 (8)
- October 2024 (10)
- September 2024 (5)
- August 2024 (5)
- July 2024 (6)
- June 2024 (5)
- May 2024 (4)
- April 2024 (7)
- March 2024 (4)
- February 2024 (8)
- January 2024 (6)
- December 2023 (8)
- November 2023 (13)
- October 2023 (14)
- September 2023 (5)
- August 2023 (6)
- July 2023 (10)
- June 2023 (5)
- May 2023 (5)
- April 2023 (4)
- March 2023 (5)
- February 2023 (2)
- January 2023 (7)
- December 2022 (3)
- November 2022 (5)
- October 2022 (5)
- September 2022 (4)
- August 2022 (3)
- July 2022 (9)
- June 2022 (2)
- May 2022 (1)
- April 2022 (2)
- March 2022 (1)
- February 2022 (3)
- January 2022 (7)
- December 2021 (3)
- November 2021 (5)
- October 2021 (8)
- September 2021 (4)
- August 2021 (6)
- July 2021 (6)
- June 2021 (7)
- May 2021 (5)
- April 2021 (4)
- March 2021 (3)
- February 2021 (6)
- January 2021 (8)
- December 2020 (4)
- November 2020 (5)
- October 2020 (7)
- September 2020 (7)
- August 2020 (10)
- July 2020 (6)
- June 2020 (9)
- May 2020 (9)
- April 2020 (5)
- March 2020 (7)
- February 2020 (3)
- January 2020 (4)
- December 2019 (4)
- November 2019 (6)
- October 2019 (3)
- September 2019 (6)
- August 2019 (3)
- July 2019 (1)
- June 2019 (3)
- May 2019 (2)
- April 2019 (2)
- March 2019 (2)
- February 2019 (4)
- January 2019 (2)
- December 2018 (2)
- November 2018 (2)
- October 2018 (2)
- September 2018 (1)
- August 2018 (2)
- July 2018 (3)
- June 2018 (1)
- May 2018 (3)
- April 2018 (1)
- March 2018 (3)
- February 2018 (3)
- January 2018 (1)
- December 2017 (3)
- November 2017 (3)
- October 2017 (3)
- September 2017 (2)
- August 2017 (2)
- July 2017 (2)
- June 2017 (2)
- May 2017 (4)
- April 2017 (3)
- March 2017 (3)
- February 2017 (5)
- January 2017 (3)
- December 2016 (2)
- November 2016 (5)
- October 2016 (4)
- September 2016 (3)
- August 2016 (5)
- July 2016 (3)
- June 2016 (4)
- May 2016 (3)
- April 2016 (6)
- March 2016 (4)
- February 2016 (3)
- January 2016 (5)
- December 2015 (6)
- November 2015 (5)
- October 2015 (8)
- September 2015 (2)
- August 2015 (5)
- July 2015 (7)
- June 2015 (4)
- May 2015 (6)
- April 2015 (5)
- March 2015 (7)
- February 2015 (15)
- January 2015 (8)
- December 2014 (5)
- November 2014 (9)
- October 2014 (7)
- September 2014 (9)
- August 2014 (5)
- July 2014 (11)
- June 2014 (5)
- May 2014 (4)
- April 2014 (5)
- March 2014 (8)
- February 2014 (8)
- January 2014 (5)
- December 2013 (7)
- November 2013 (7)
- October 2013 (14)
- September 2013 (12)
- August 2013 (15)
- July 2013 (15)
- June 2013 (15)
- May 2013 (15)
- April 2013 (15)
- March 2013 (15)
- February 2013 (15)
- January 2013 (15)
- December 2012 (15)
- November 2012 (15)
- October 2012 (15)
- September 2012 (15)
- August 2012 (15)
- July 2012 (15)
- June 2012 (15)
- May 2012 (15)
- April 2012 (15)
- March 2012 (15)
- February 2012 (15)
- January 2012 (15)
- December 2011 (15)
- November 2011 (17)
- October 2011 (17)
- September 2011 (17)
- August 2011 (21)
- July 2011 (20)
- June 2011 (17)
- May 2011 (15)
- April 2011 (17)
- March 2011 (25)
- February 2011 (20)
- January 2011 (20)
- December 2010 (18)
- November 2010 (21)
- October 2010 (21)
- September 2010 (25)
- August 2010 (20)
- July 2010 (10)
- June 2010 (11)
- May 2010 (19)
- April 2010 (16)
- March 2010 (14)
- February 2010 (22)
- January 2010 (18)
- December 2009 (20)
- November 2009 (20)
- October 2009 (3)
- September 2009 (21)
- August 2009 (19)
- July 2009 (12)
- June 2009 (12)
- May 2009 (11)
- April 2009 (15)
- March 2009 (21)
- February 2009 (4)
- January 2009 (12)
- December 2008 (13)
- November 2008 (9)
- October 2008 (22)
- September 2008 (20)
- August 2008 (16)
- July 2008 (14)
- June 2008 (7)
Blog Stats
- 6,681,990 hits
Please give your feed back .
Click below to see who is watching this website live !

- This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .

Please Note

