Click over the Image for animation

Posted in Cardiology - Animations, Cardiology -Non coronary Interventions -PTMC, cath lab tips and tricks, PTMC -Tips and tricks | Tagged difficult ptmc, how to cross a crtical mitral stenosis, inoue balloon, mitral valve crossing, mitral valvotomy, percutaneous mitral commissurotmy, ptca balloon during ptmc, ptmc, subvalvular fusion in ptmc, tough ptmc | Leave a Comment »
Regurgitant lesions of cardiac valves are often tricky for the heart . Myocardium shows “love- hate” relationship with these leaky valves. Some of them are “sort of” stress relievers for LV . A mild MR will make the LV comfortable in terms of wall stress. When the wall stress is reduced the contractility increases and LV EF may raise a little.Hence EF is never going to help us to assess true LV function in MR .
LV end diastolic dimension(LVEDD) is a preload dependent parameter .A patient with 6.5cm LV EDD may still have good contractility and he may reach even a 40mm LV ESD, implying an intact LV function.
LV function should be best assessed in systole .(After all , systole is the prime function of heart) .Further , it should be assessed when the LV is free from influence of the all loading conditions of heart . (Note : The initial part of systole depends on after load. As the systole progresses the influence of after-load lessens .In the pressure volume loop* , the point at which loading conditions are least operative is end systole.)
* Please realise , heart is a dynamic organ there is no true load independent point in cardiac cycle as pressure and volume are eternally coupled.
What happens in AR ?
The same rule applies for Aortic regurgitation, but the parameters worsen little later than that of MR. For same degree of regurgitant fraction MR will require early surgery than AR.The reason for better tolerablity of AR is due to largely intact LA function and compliance till very late stages of AR.(In AR- it’s single chamber volume overload , while in MR it’s two chambers !)
Final message
LVEDD is not used in assessing MR as it is a pre-load dependent parameter that will not reflect true myocardial function /dysfunction. LV ESD is fairly accurate measure of LV systolic function minus all loading factors .
Watch out for next topic
Vasodilator therapy in MR and AR : How is it different ?
Posted in Cardiology -unresolved questions, Infrequently asked questions in cardiology (iFAQs), Mitral regurgitation, rheumatic heart disease, valvular heart disease | Tagged cut off for lv esd 55 mm in mr ar, lvedd vs lvesd, mitral reguritation when to operate, mr vs ar operability, pressure volume loop in mitral regurgitation, why we take lv end ssytolic dimension for assessing lv function ? | Leave a Comment »
Medical research often ventures into a directionless and meaningless exercise with or without intention .The reason is simple , unlike other fields, scientists enjoy the ultimate freedom of expression.
How to find genuine treasures from this chaos ?
We need people like Valentine Fuster ,
Here is link to the article in circulation 2011 which I consider a must read for all cardiologists !

Posted in cardiology journals, Cardiology research topics, Cardiology Risk assesment, Great Men in cardiology, Great websites in cardiology, history of cardiology, Land mark articles in cardiology, Top ten in cardiology | Tagged epidemic of cad, future of cardiology, global cardiology issues, land mark articles in cardiology, preventive cardiology, promoting global cardiovascular health, top articles in cardiology, valentine fuster | Leave a Comment »
Many modern day cardiologists consider doing echo , a mean job and leave it to technicians and fellows . Final report often ends up with a cursory glance. The culture of reporting an important aspect of LV function is reaching a new low. It is common to find the following terminologies in the echo reports in many parts of the country* (Guess it is not used elsewhere ! )

Among these , the term adequate LV function has caught the imagination of young cardiologists ! Especially , this description often appear in pre- operative screening echo for non cardiac surgeries .
Recently ,one of my patient asked me what do we mean by adequate LV function . I told him it means nothing . . . it’s all fancy words ! but , generally it is used to imply normal LV function . . . I clarified .
Think over for few minutes . . . what do we want to convey by calling LV function as adequate ?
Does it mean normal ? or Just less than normal ?
If adequate LV function is accepted , what is inadequate ?
Adequate for whom ? For the patient ? or for the physician ?
Adequate for daily activity ? or Adequate to with-stand the proposed surgery ?
Final message
Even learned cardiologists indulge in this term frequently . This is rather a fancy and unprofessional way reporting LV function . They pass this style to their residents as well para medics .Adjectives in medical science are not banished . . . but should be judiciously used . In my opinion the term adequate LV function should be removed from all echo labs . Youngsters please watch out.
Related links in this site .
Posted in Cardiology -unresolved questions, echocardiography, LV function | Tagged LV ejection fraction, lv function parmeters, what do we mean by adequate lv function ? | Leave a Comment »
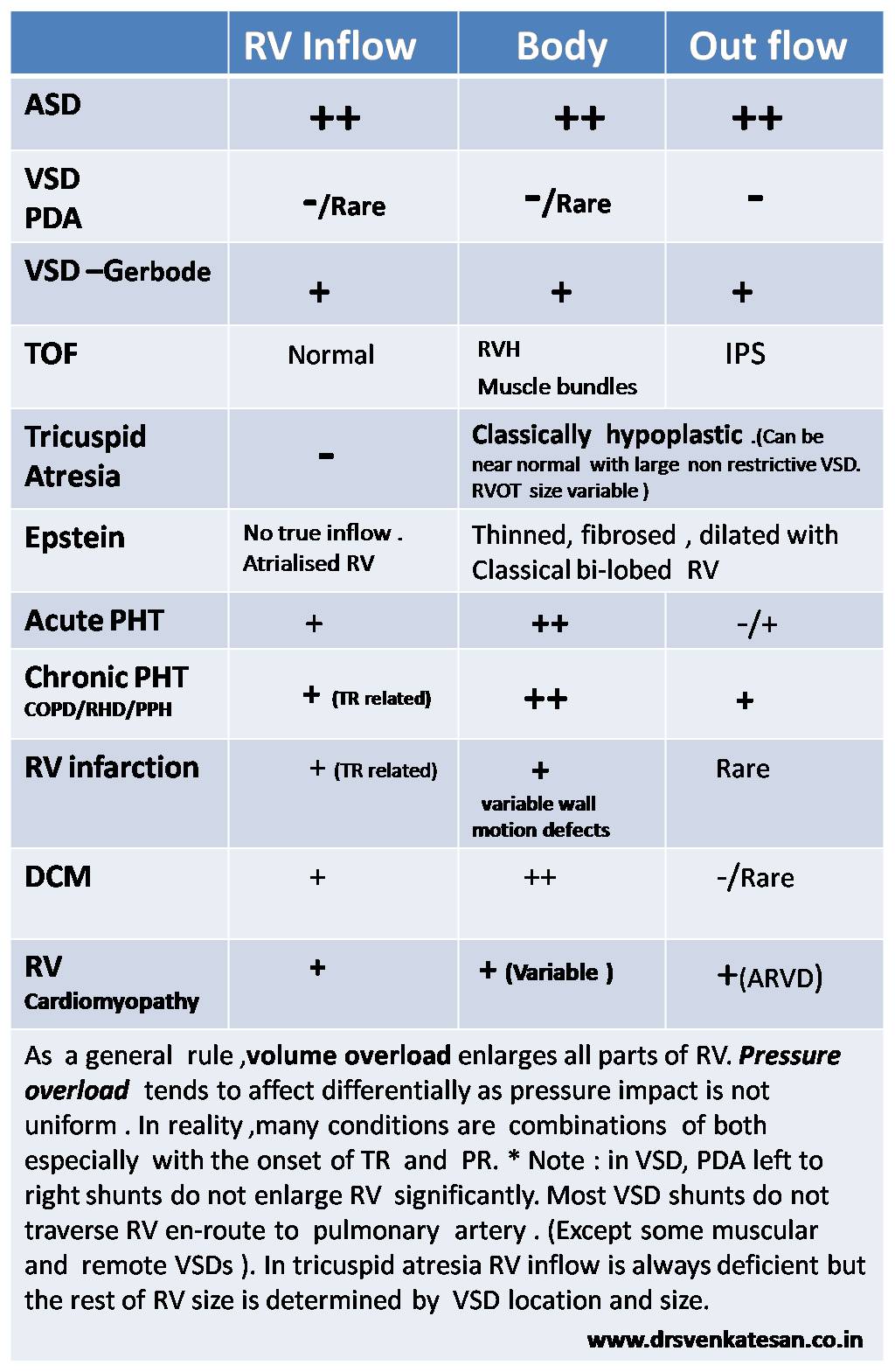
Right ventricle is a passive venous component of the heart .It simply acts a transit pump for blood to reach the lungs.
It is true , RV is dispensable in many complex congenital heart disease as we can connect the great veins directly into the pulmonary artery by Fontan , Glean and it’s clones bye passing this chamber . Still , by no means the importance of this chamber is to be underestimated. RV dysfunction and failure is the key to survival many disorders.RV shock is is cause of sudden cardiac death in acute pulmonary embolism and RV infarction .
RV is an unique muscular chamber .It is more of a triangular shape. It has three different parts connected by three different angle .There is no true apex for RV , it is connected to Inflow and outflow in peculiar fashion .
In the following table I have tired to describe of how different parts of RV behave in various disorders.
Posted in cardiology congenital heart disese, Clinical cardiology, myocardial disease, Right ventricle | Tagged arvd, ebstein anomaly, epigastric pulsation with rvh, how is rv in various heart disease, infundibular dilatation, para sternal lift, parts of right ventricle, right ventricle, right ventricle in tof, rv in tricuspid atresia, rv inflow body out flow, rv morphology in various congenital heart disease, rvot dilatation | Leave a Comment »
 Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Reference
Clark EB. Mechanisms in the pathogenesis of congenital heart defects. In: Pierpont ME, Moller J, editors. The Genetics of Cardiovascular Disease. Boston, MA: Martinus-Nijoff; 1986. pp. 3–11.
Posted in cardiology -congenital heart disease | Tagged clark classification of congenital heart disease, classification of cono truncal defects anomaly | Leave a Comment »
Normal left atrial (LA) volume is about 22ml/sq.meter body surfacearea at all ages.Maximum LA volume in physiology is about 46ml in females and 56 ml in males( Average 35 ml)
LV stroke volume for each beat is about 70 ml . . . so where does the remaining 35ml come from ?
Answer .
It is logical to assume about 35 ml of fresh blood from 4 pulmonary vein* rushes into LV with every diastolic cycle .It never stays in LA .It just uses LA as a transit route ,
*In diastole the four PVs,LA and LV all act like one single chamber .
Is this reasoning correct ?.
If we believe the continuity equation this explanation is correct . However still what we need to know the fate of residual LV volume (End systolic LV volume which is also about 35 ml that would be in queue for ejection into Aorta for the next beat !)
Further , we know the LV end systolic volume is not constant .During exertion it can reach negligible levels (<10 ml) .At times of vigorous contractions it can touch near zero as well . Then , It become vital for the pulmonary venous reservoir to be act as a major donor for LV blood volume for every ensuing beat.
If the hemodynamics of pulmonary vein LA interface is tricky even in physiology , one can imagine the complexities if the LV diastolic function and left atrial compliance is affected
Debit and credits of LV end -diastolic volume .
Let us assume LVEDV is about 1o5 ml .LA blood volume is roughly one third of LV volume .For every beat equal amounts of fresh blood from pulmonary vein . These two (LA+PV) adds to the residual blood in LV to make LVEDV 105 ml . From this 70 ml is ejected as stroke volume leaving behind 35 ml.

Image template from http://www.cvphysiology.com
Further questions
LA Chamber volume and blood volume need not be same .What I struggle to understand is , total anatomical LA volume measures 35ml , while the amount of blood it is supposed to hold is also about the same .Does it mean the LA is completely filled with blood . . . air tight !
Will the LA compliance make it accommodate twice or thrice the blood volume during exercise ?
What is quantum of residual end diastolic LA volume ?
Reference.(Normal LV and LA volumes )
![]()
Posted in cardiac cycle, cardiac physiology, cardiac volume, Cardiology -Hemodynamics, Cardiology -unresolved questions | Tagged cardiac cycle, componets of LV stroke volume, end systolic lv volume, la volume vs lv volume, relationship between la volume and lv volume | Leave a Comment »
Obesity is a major cardio vascular risk factor.We earnestly believe this by evidence from Framingham and other studies.However , epidemiological truths can be dissociated from individuals .
We now understand some of the obese patients fare better in CHF outcomes apparently because of the obesity ! Even patients who undergo PCI show some benefits.This concept is being proved in large data base of > 200,00 patients.
Possible mechanisms
The lay man’s logic may apply (Science hidden somewhere !) Obese persons have basically a large heart with better cardiac reserve and muscle mass .These hearts are pre-conditioned to extra burden of MVO2 in it’s life time . So it is able to tackle hypoxia better, takes more time to get fully exhausted .After all heart can consume fatty acids for it’s energy requirement.
Adipose tissue may also secrete favorable anti-inflammatory chemicals , though majority of adipocytokines are detrimental except adiponectin .Paradoxically the tumor necrosis factor TNF (Same as cachectin or Interleukin 6) is less in obese patients .
Reference




Reference
The landmark Lancet article that first raised the question of obesity paradox
http://www.ncbi.nlm.nih.gov/pubmed/16920472
http://care.diabetesjournals.org/content/36/Supplement_2/S282.full.pdf+html
Counter to the concept

http://science.howstuffworks.com/life/human-biology/obesity-paradox.htm/printable
Obesity paradox applies in stroke too ! This study (TEMPIS) from Berlin Germany suggest controversially though
Posted in cardiac failure, cardiac physiology | Tagged adipoctokines, adiponectin, Gross obesity, lipids and heart, obesity and tumor necrois factor, obesity paradox, paradox in cardiology, smokers paradox | Leave a Comment »
Cardiologists are not single organ specialists . They are supposed to be sincere guardians of the the entire vascular system .Sexual dysfunction in males is almost synonymous with erectile dysfunction(ED) .The male sex organ is equally dynamic organ like the heart . It demands a sudden gush of blood to the tune of 500 ml during complete erection .This conveys an important message . The penile macro and micro vasculature is as important as coronary mIcrovascular bed. Atherosclerois of LAD can be as common as atherosclerosis of pudendal artery .It can precede or follow the coronary lesion. Penile insufficiency is a early marker of endothelial dysfunction. All patients with CAD should be screened for ED and vice versa.
This is not a sexual intrusion in academics , but I am sure , a sustained erection that completes a normal sexual act may very well rule out a proximal LAD lesion 99 % of times .
Do you know , > 7 Mets on a tread mill will rule out a significant left main disease with high degree of accuracy ! Sexual acts require more than that (One may do a study on this !)
There has been some interesting guidelines for managing issue of sexual dysfunction in CAD. .Princeton consensus conference is the famous one.
References



Posted in cardiology -Sexual health, Cardiology -unresolved questions, Infrequently asked questions in cardiology (iFAQs) | Tagged erectile dysfunction in cad, princeton consenus conference 2 3, sexual dysfunction in cardiolgy | Leave a Comment »
While many of us are preoccupied with wires and balloons ,( coronary myopia ! ) , our radiology colleagues are making rapid strides . Let us spend some time to understand how the myocardial segments are inflicted the final insult . We need to realize , there is a pattern to this myocardial end game of scarring and fibrosis.
MRI is the gold standard to assess the myocardial architecture . It has a role in both assessing the anatomy , function , perfusion and viability .

Why is scar localisation and Quantification important ?
Apart from differentiating various cardiomyopathies it has few clinical implication .

Posted in Cardiac MRI, Cardiology -unresolved questions, myocardial disease | Tagged cardiac mri, demri, epicardial scars, how to differentiate ischemic from non ischemic dcm, late gadolinium enhancement, lge gadolinium, mid myocardial scar, myocardial scar Imaging, scar location within myocardium, subendocardial scars | Leave a Comment »



