I stumbled upon this web site . I think this can be glorified as the standing example for “Democracy of science”

http://www.intechopen.com/subjects/cardiology-and-cardiovascular-medicine
I stumbled upon this web site . I think this can be glorified as the standing example for “Democracy of science”
http://www.intechopen.com/subjects/cardiology-and-cardiovascular-medicine
Posted in cardiology innovation, cardiology journal club, Cardiology journal links, cardiology journals, Cardiology teaching websites, Cardiology-Land mark studies, Great websites in cardiology | Tagged great learning websites, INTECH open science open mind, OPEN ACCESS JOURNALS, SCIENTIFIC DEMOCRACY | Leave a Comment »
Doctor , I am getting sudden compressing type of pain which starts in the centre of the chest and soon transmits to the left shoulder and gradually reach the inner aspect of the hand up to the little finger . And occasionally it is very severe and some times i feel like sweating as well ! I am unable to predict when it comes doctor !
Final message
Pain is a feeling . It can be perceived at multiple levels . The site of origin , spill over on transit and at the level of brain . A patient with multiple potential source for pain can either summate , deduct , reflect or cancel out .This can confuse the clinician in a dramatic fashion as it did to us ! . To complicate the matters further , gastric pain can trigger a cervical pain and vice versa . (Spill over effect)
Posted in cardaic physiology, cardiac physiology, Cardiology - Clinical, Clinical cardiology | Tagged atypical chest pain angina, classical angina, clinical cardiology, differential diagnosis for chest pain, gastrits and cervical spondylosis equals angian | Leave a Comment »
Only fools will manage unstable angina medically !That was exactly the statement , one popular Interventional cardiologist told a small gathering in one of the weekly meet . Do you agree ? Answer We can’t make a blanket statement like that . We have clear guidelines (Of course as licensed and certified cardiology practitioner you have every right to violate it !) . UA is risk stratified in Low , Intermediate and High risk categories .Only high risk group require emergency Intervention .Even in high risk group there are some reservation.(ICTUS study ) There are some very mild forms of UA (High grade stable angina precipitated by an emotional stress will exactly mimic UA. Similarly most secondary UA due to tachyardia , Anemia etc should not cause an alarm .) *Please note , currently coronary angiogram is included in medical investigation in most patients with UA . The confusion in interpreting such statements is partly because many physicians/ cardiologists consider doing a coronary angiogram by itself an Interventional management Reference
Posted in Cardiology -Interventional -PCI, cardiology- coronary care | Tagged ictus study unstable angina, pci for unstbale angina, risk stratification of nstemi, unstable angina nstemi medical management | Leave a Comment »
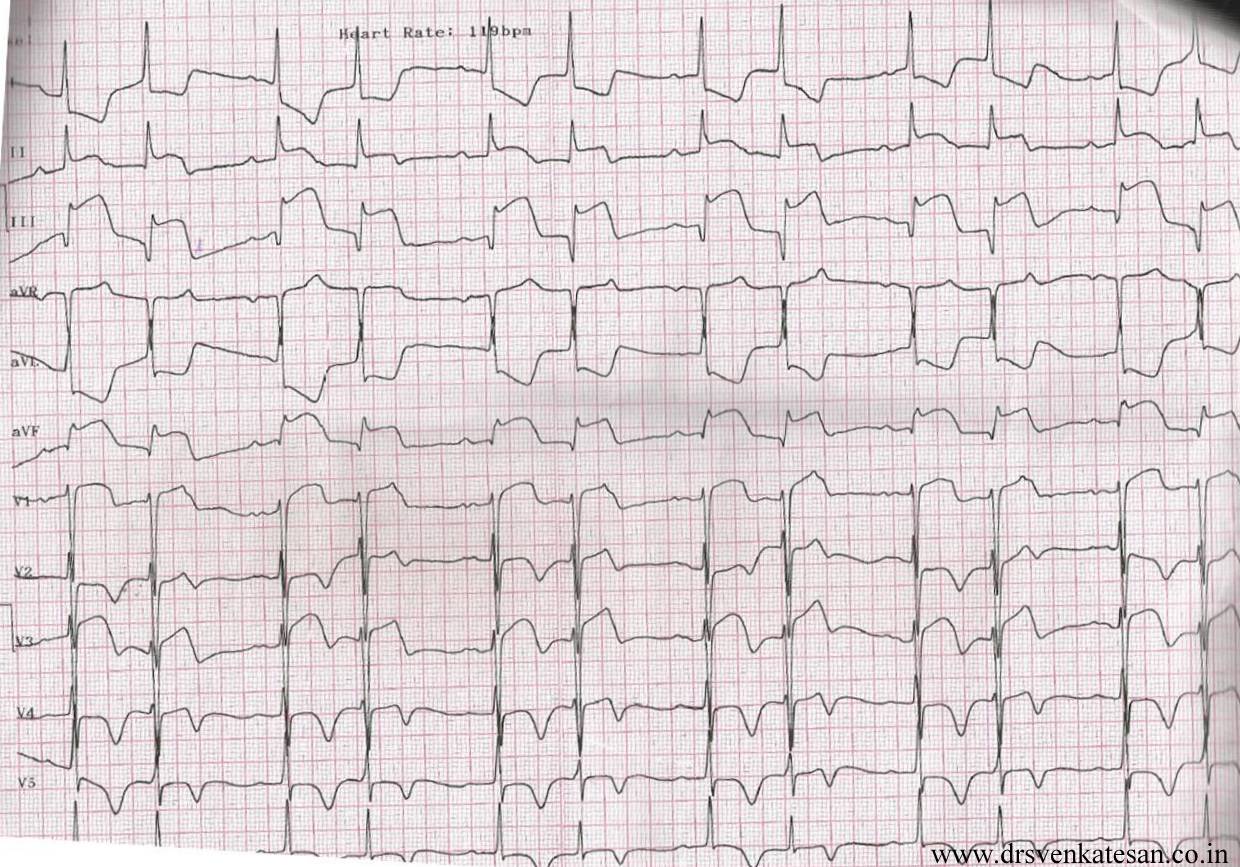
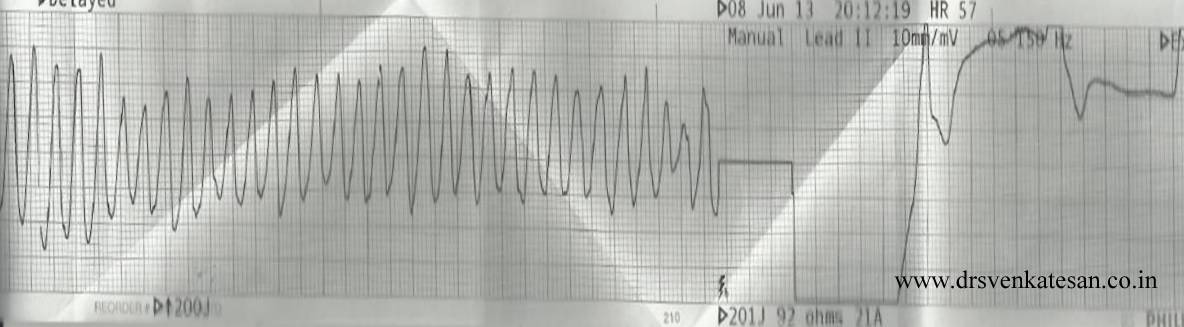
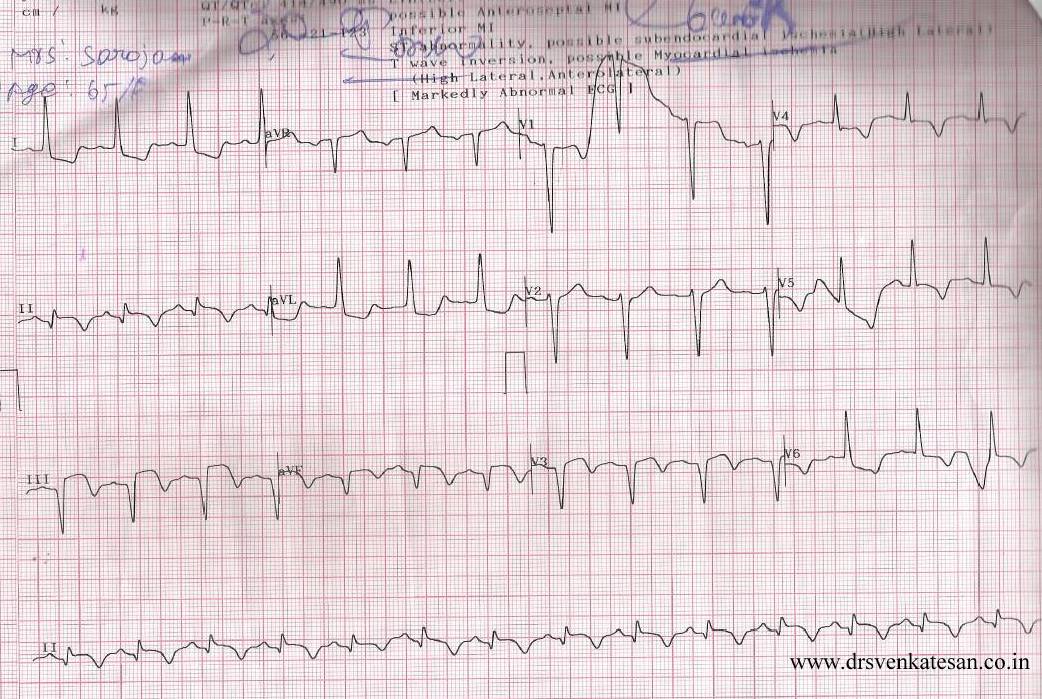
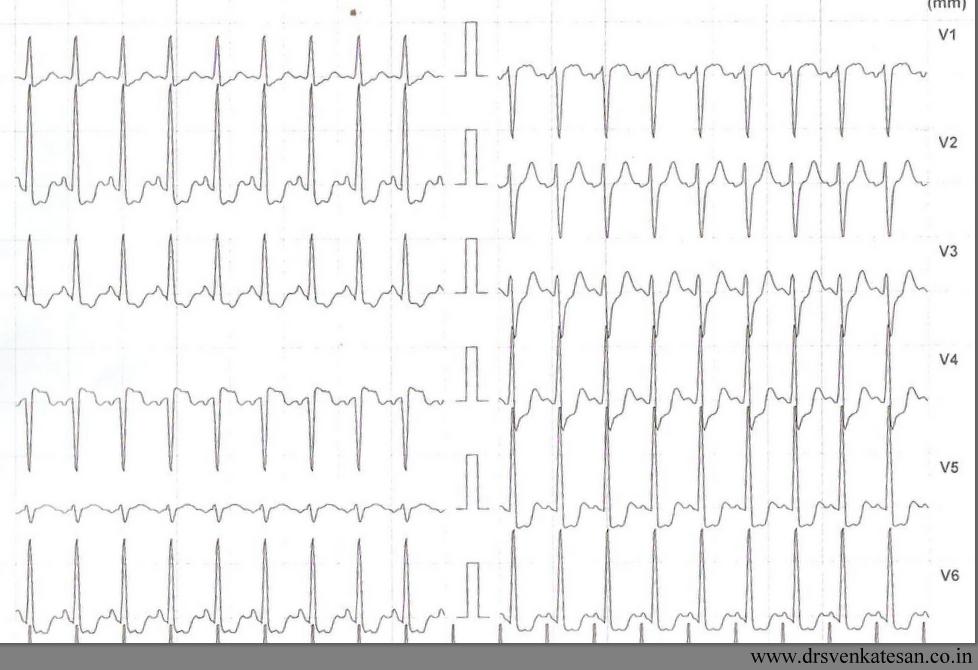
This is the story of a 55 year old women , who was received in our CCU with a dramatic STEMI (ECG looked like an action potential ) , LV S 3 and hypotension. It was impending cardiogenic shock.Since we do not have full fledged primary PCI program , thrombolysis was planned. She had cardiac arrest immediately after starting streptokinase infusion . She was promptly shocked and revived . The ECG changes rapidly reversed(ECG -3) . Every other hemodynamic parameter got stabilised as well . To our surprise ( few hours later ) this patient was so comfortable , sat up on her bed , demanded a discharge . (Which was refused of course !) One week later coronary angiogram was done, a near complete recannalisation of RCA was documented.
ECG 1 on arrival

ECG -2 Developed cardiac arrest 10 minutes after starting the Streptokinase Infusion
ECG -3 .Taken few minutes following the VF
Acute myocardial infarction (STEMI) kills more than a million life every year . Majority of death happens within an hour of onset of symptoms. Ventricular fibrillation is the arrhythmia of death. Why this occurs only in few , while many are immune to it ?
God keeps this secret close to his chest , how and why he selects candidates for this arrhythmia !
Scientists are still far away in finding the truth . But , one thing is obvious .The moment coronary artery is totally occluded , the heart begins a fight and try to get rid of this obstruction . In the process , it goes into convulsion (VF) with a foolish belief , it can shrug of the thrombotic insult . Death often ensues if not intervened . (Very rarely VF can be a non sustained one and patient survives cardiac arrest !)
VF as a electrical response to reperfusion injury .
Often times , we witness patients to go for VF very early following thrombolysis . The thrombus in situ is an irritant , it triggers the inherent fibrinolytic system (Natural TPA included) If it is successful it opens the occlusion ( atleast partially ) and salvages the myocardium .If the fate is against the patient , very early reperfusion of IRA triggers VF . If this occurs at home survival is low .If the VF occur at hospital the probability of survival is near 100 % .
The intensity of natural lytic mechanism is the major determinant of early reperfusion . Ironically the same factor determines occurrence of the deadly VF .
I would believe , the STEMI patients who die early (even before reaching the hospital ) are (un) blessed with a fighting heart ! Ironically , the lazy hearts reach the hospital alive ! (slow & steady win the race !) . Of course , reperfusion injury is not the only mechanism of VF . Other common suspect is left main STEMI .
Link to related video “Ignorance based cardiology ”
https://www.youtube.com/watch?v=J9DH6Vr04es
Final message
While , VF is referred to as arrhythmia of death , it may in-fact , represent a common form of reperfusion arrhythmia in the setting of STEMI ! . . . Hence , it can Initiate a new lease of life in many lucky ones ! I hope the title of this article makes sense !
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, STEMI-Primary PCI | Tagged arrhythmia of life and death are same, primary ventricular fibrillation, reperfusion arrhythmia | Leave a Comment »
//
Posted in cardiac physiology, Cardiology -Interventional -PCI, Cardiology -unresolved questions, excercise stress test .EST, Hardware techniques tips, Infrequently asked questions in cardiology (iFAQs), PCI PTCA Hardware | Tagged fame 1 fame 2 study, ffr vs oct vs ivus vs NIR, fractional flow reserve, functioanl syntax, physiological impact of anatomical lesion | 1 Comment »
Do not ever under estimate the importance of TIMI 1 flow . It can save a major chunk of myocardium ! A late TIMI 3 flow . . . is far inferior . . . to an early TIMI 1 flow . * Even a trickle of flow (Ooze ) can keep the myocardium alive . This point we have realised very late. Thus came the pharmaco Invasive strategy for all STEMI who have no immediate access to cath lab ! (please note 90 % of STEMI belong to this group )
For a high resolution Image click below

Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics | Tagged failed thrombolysis, pharmaco Invasive strategy, rescue pci, stemi maangement, time window for pci | Leave a Comment »

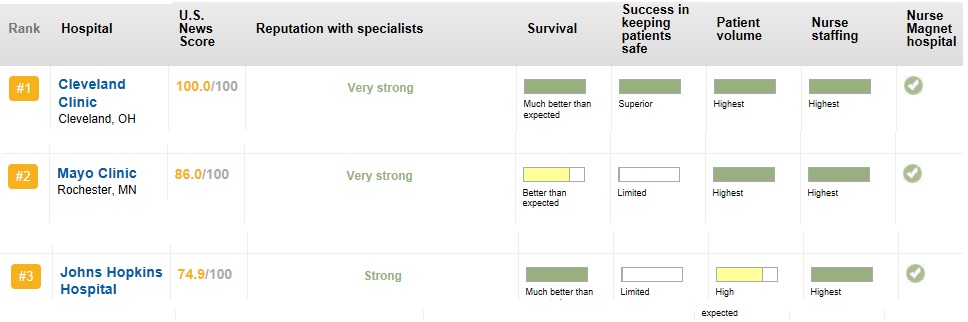
The top 3 cardiac care hospitals for the year 2012-2013
//
Posted in Top ten in cardiology | Tagged America's top hospital, cleavland clinic mayo clinic jhon hopkins, us news and world report top hospital 2012 2013 | 1 Comment »
Click on the file to download the presentation
Note : The contents are prepared in 2006 .Recent input are to be added .
//
Posted in Cardiology -Interventional -PCI, My presentations | Tagged follow up of pci patients, management of post pci patients, pci ptca, ptca ppt | 1 Comment »
Thrombus laden plaque is sine qua-non of UA/NSTEMI . That’s what we have been taught ! right ? It may be true in many situations , but please remember there is another concept called demand ischemia , where in there is no active thrombus , still resting angina may occur due to increasing heart rate etc.
I just wanted to test how far this concept is understood , by the fellows in our coronary care unit . Following is story of a patient who arrived at CCU with angina at rest . I showed this ECG asked them the management .
History was purposefully blinded . 5/6 cardiologists wanted to admit the patient either in CCU or rush to cath lab. Heparin/ Fondaparuinux was prescribed by all. Tirofiabn was suggested by few.It is a high risk UA with left main disease some one mumbled .
I silently listened to them and revealed the history . This patient has just finished the exercise stress test , it was terminated as he had angina at peak exercise. and was reported as positive . A date was fixed for elective coronary angiogram. 10 minutes later ECG totally normalised , and the patient went home (Boarding a crowded Chennai city bus )
The fellows realised the importance of history . In fact no body asked for it ? I felt bad as all my fellows failed in this test That reflects bad teaching on my part !
What is the mechanism of ST depression here ?
(Severe forms of stable angina can occur at rest . So do not equate all rest angina as true unstable angina !)
Final message
Do not label an ECG straightaway as acute coronary syndrome when there is baseline tachycardia and ST depression . Spare few minutes and apply your mind !
If a combination of ST depression and angina can be taken synonyms with UA every EST positive fellow should be labeled as UA and admitted in CCU. Please remember any tachycardia with a fixed tight lesion will mimic UA . Further , since there is no thrombus here and there is absolutely no role for heparin.
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions | Tagged demand ischemia and unstable angina, mechansim of unstable angina, secondary unstable angina, thrombus less unstable angina, unstable angian without thrombus | Leave a Comment »
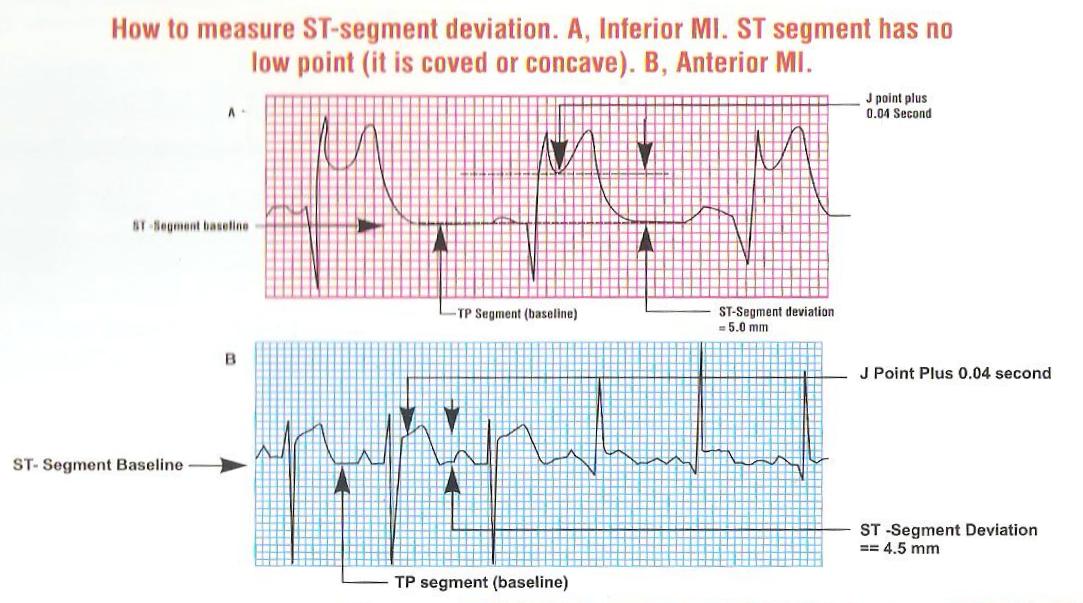
ST segment elevation is the key parameter on which the fate of millions of infarct patients are recognised and managed. It is ironical we do not have standardised reference point for measuring the quantum of SR elevation .
This is especially difficult when ST segment blends with forward limb of T waves.
While we have reference point for measuring ST depression (Like during EST ). . . why we do not have one for ST elevation ?
Now we have adopted a rough criteria .Read below .


Posted in Cardiology - Clinical, cardiology -ECG, Cardiology -Interventional -PCI, Cardiology -unresolved questions, Cardiology-Coronary artery disese, Clinical cardiology | Tagged ECG, how to measure st segment elevation | 1 Comment »