Here is a case report from Dr. Brugada’s group. What is your diagnosis? 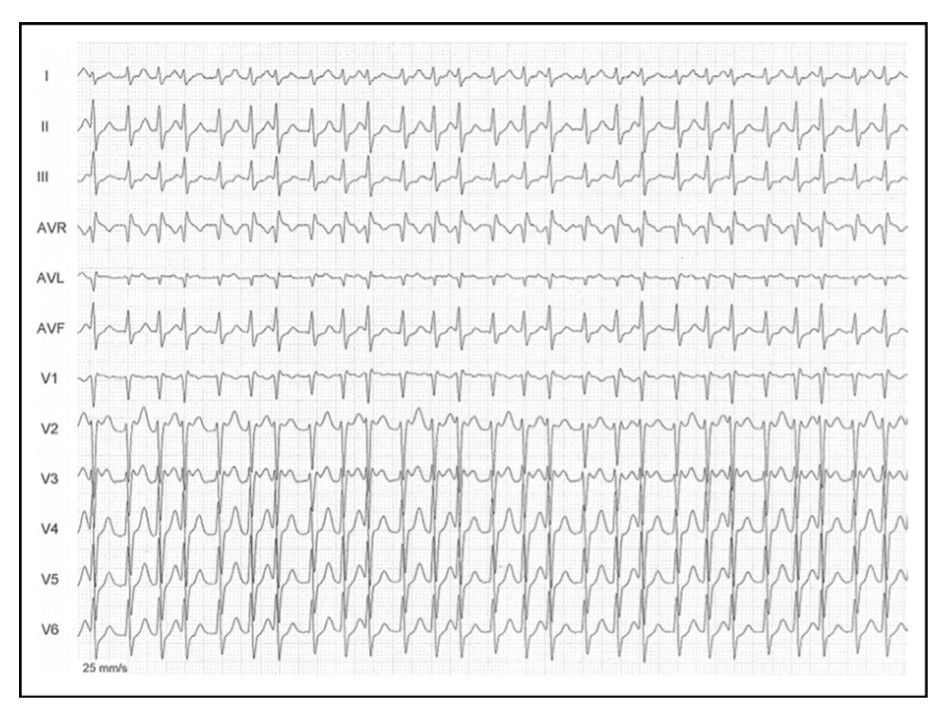
Source & Courtesy Sergio Richter, Joseph Brugada et all , 100(1), 154–156. doi:10.1016/j.amjcard.2007.02.067
Whoever diagnosed AF in the above ECG need not feel bad. The rhythm is not AF, though it mimics very closely. In cardiology, especially in electrophysiology, we can get surprises on a daily basis. (Read below)
Why the ventricular rate is irregular in AF?
Atrial fibrillation (AF) may sound like a simple clinical arrhythmia until we ask this delicate question. The traditional and fairly accepted answer is that, AV node with all its collective decremental property filters the incoming atrial impulses (Which varies 400-600/mt) in a random fashion and allows only about 1/3rd of impulses. So, technically it is AV block of various degrees that makes the ventricular response irregular.
Any other explanation possible?
How about AV node playing out a silent game with Atria, deciding to block everything and start its own fast escape rhythm, rather than leaking out selectively atrial impulses. Some think this is fictional, some others feel it can be real too. When this happens it can be referred to as irregular junctional tachycardia or AF with varying AV blocks. It has been tough, to prove it is only the atrial impulses penetrating through the AV node complex and exiting on the ventricular side unscathed?
Understanding AV node is not easy
AV node morphology and function still remain a mystery.( Katritsis DG. Arrhythm Electrophysiol Rev. 2020)The AV node shows huge variation in its size, shape, orientation with LV long axis and AV plane in short axis. The approach to slow pathways with multiple inferior nodal extensions makes a dual (or even poly ) AV pathway in any human being real. How common is dualism or multilateralism within the AV node in the general population? (More than 30-40 % ?) . Let us also mind the traffic in this busy & complex AV flyover can change on a moment-to-moment basis based on neurohormonal and autonomic tone.
Any tachycardia can become irregular if the AV node wishes so !
Though rare ,multiple physiological splits in the AV node make it possible for a single atrial impulse can generate 2 or 3, even more, ventricular impulses. (1: 2 or 3 AV conduction) Since these pathways are dynamic they can make the ventricular response irregular as well (Unlike the regularly coupled Echo beats in classical AVNRT substrate ). Hence, any supraventricular tachycardia can masquerade as AF if AV nodal pathways decide to split and share the impulses this way. It is also interesting to note there has been a documented link between AVNRT and AF (.Ref 2) . Also, adenosine-induced AF is known (James E. Ip et al Circulation: Arrhythmia and Electrophysiology. 2013;6:e34–e37)
Final message
Irregular RR interval with absent/or invisible P waves is not always AF. It can be due to the aberrant behavior of the AV node.( anatomical or functional) It is termed Pseudo Atrial fibrillation as in the above case report. Why do we need to be aware of this entity? We need to be cautious, as any overzealous efforts to ablate the pulmonary veins in such patients will go in vain.
Reference