Note :This is a copy of my earlier blog on coronary micro-circulation published few years ago.Recently this got numerous hits .Hence I have just reposted it with slight modification.
Human coronary circulation stands unique among others as it is a life-sustaining circulation.It is indeed a great medical achievement to visualise the right and left coronary artery system by coronary angiogram. Actually, what we see is only a fraction of the surface area of coronary circulation .The surface area of epicardial coronary arteries constitutes less than 5 % of entire coronary vascular tree .
This is the reason normal coronary angiogram can never mean normal coronary circulation !
This huge gap in our perception is the single important factor that explains the vagaries of modern coronary care .
This also make any clinical coronary scenario a reality .
“A patient with normal coronary angiogram getting a myocardial infarction , the next day and a severe triple vessel disease living comfortably for decades with medical management”
So , it is essentially a false sense of scientific accomplishment by the cardiac scientists at least in the of coronary circulatory physiology.
What determines the extent of these invisible coronary micro circulation ?
There are innumerable channels of micro vessels traversing across the heart, sharing , bridging , branching, penetrating and perfusing the muscle mass.They can be anatomically patent , physiologically non patent .They can be recruited by hemodynamic stress .These are never visualized by current imaging modalities..It is also influenzed by favorable growth milieu and hormonal and neural stimuli.
Ignorance based cardiology
What is the mechanism of primary VF following acute STEMI ?
The quantum of coronary micro circulation is like the vast cerebral neuronal net work .We have every reasons to believe they are have unique genetic imprint.How else you can explain a man with full blown STEMI come 24 hours later comfortably to the OPD while another loses his life with a stormy primary VF before even boarding the ambulance !
Why many cardiologists do not give due credit the coronary collateral circulation ?
It has been our traditional teaching ( without much evidence of course !) coronary collateral circulation is not effective to support blood flow during exercise . This fact has been disproved many times . Coronary collateral circulation was indeed useful in limiting damage in ACS and relieve symptoms in stable angina.It helps in reverse remodeling and provided electrical stabilty as well in post MI population.
Still , the concept was alienated and made totally irrelevant in the interventional era . Many cardiologists found well-developed collateral’s as an interference to their expertise and ego since it has a potential to alter the indication of PCI.They continue to have strong scientific conviction (Pseudo ?) that man made collaterals must always been superior to God made collaterals !
Whenever some credible reports emerge about collateral circulation being equivalent to revascularisation procedure , these concepts were prematurely buried for some reason.
In the last decade there was a concern about performing PCI in patients with well-developed collaterals .The argument was , they tend to develop early stent occlusion and restenosis . It was a genuine query raised by few thought leaders in the field as collateralised vessels suffer from low flow after PCI , if the pre -existing collateral continue to function.
But then , few studies countered this , and PCI was shown to be safe and in fact may fare well in patients with extensive collaterals .
In these studies interventionist’s argument looked amusing ! as they seem to define a successful PCI as not only to open the occluded vessel but also make sure to close all functioning collaterals .(What a a pity for our natural biological angiogenic forces which had worked and grown meticulously for months!)
Cardiac science in the current format, makes the future look bleak for coronary a collateral circulation .With early PCI becoming a norm we will never ever allow the natural collaterals to grow , and even the established collaterals will have to face a stiff fight for survival with sophisticated coronary interventions .
Competing interest in the filed of coronary collateral research
While the basic scientists want to grow collaterals with angiogenesis , stem cells etc interventionists continue to indulge in rampant angioplasties which will suppress collateral growth.
This implies we will struggle to establish the true importance of coronary collateral circulation .
Final message
Can it be an effective form of revascularisation ?
My personal inference is coronary collateral circulation “would and should” have a definite role in at- least some of the subsets with chronic coronary syndromes. If we think otherwise . . . it’s against the principle of natural biological science .
A good collateral system with optimal medical management can save not only our patient’s lives but also their hard earned currencies !
Reference
Here is a rare article in European heart journal that discuses coronary collateral circulation . Let us welcome such wonderful reviews which keep the interest alive on the filed.
Left main ostial lesion remains a challenging task .A new stent design is proposed here.
The lesion
The hardware
The technique
Final message
This thought came when I recently encountered a patient with a left main ostial stent which was projecting well into aortic root .It is an open access patency ,whoever is capable of converting this idea to a clinically applicable technique is welcome to proceed !
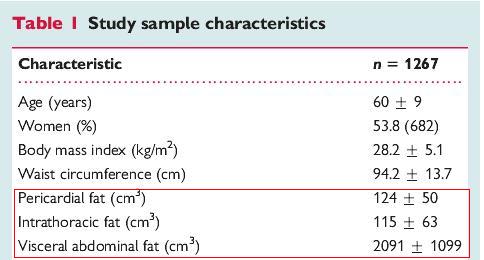
Epicardial fat is increasingly recognised to be a coronary risk factor.
Methods to measure and quantify epicardial fat has not been standardised.
Nomenclature issues
There is some confusion in the literature regarding the definition epicardial, pericardial , paracardiac fat etc.
Epicardial fat is the true visceral fat located in proximity with myocardium .Epicardial fat shares the same blood supply as adjacent myocardium and also show para-crine functions.This is the risky fat that is metabolically active.
Paracardiac fat is the fat deposited outside the parietal pericardium .It is also referred to as thoracic fat .They carry less risk and behave more like somatic non visceral fat.
Pericardial fat is a loose terminology .Many use epicardial and pericardial fat interchangibly .It is to be realised , fat either deposit inside the visceral pericardium or outside the parietal pericardium. It almost never deposits within the pericardial space.
* Currently it is better to use only two terms .Epicardial fat and thoracic fat .Other terminology should be avoided.
How to measure and quantify epicardial fat ?
Distribution of fat over heart is not uniform .Though it appears a random distribution there app eras to be a pattern to it .It is largely loaded anterior surface of the heart, over the AV grooves, invariably hugging the coronary arteries and great vessel origins.Fat deposition posterior to heart occurs in gross obesity.
There is no accurate way to quantify it . A rough estimate can be arrived . The following investigations are useful.
Echo
Multi-slice CT Scan
MRI
Epicardial fat pad thickness by M-Mode /2D is simplest, but considered crudest modality to quantify. .Still , it is a useful screening test. In our experience , if there is distinct anterior fat pad > 5mm it is likely to be significant.
However, epicardial fat volume is ideal method to quantify it.(Read below)
Which part of cardiac cycle it is measured ?
Since epicardial fat is a compressible structure , in diastole the myocardial mass encroaches the epicardium any imaging modality the distinction between epicardial and para-cardiac fat tends to attenuated.
Even MRI images obtained with diastolic gating , may not be reliable .End systolic frames are now considered ideal.
Estimation of epicardial fat volume is largely a research tool.In grossly obese patients it may have some clinical utility.Increased anterior fat pad in routine 2D echo is an useful screening test. However, it requires MRI/CT imaging for accurate quantification.
CHB with CAD is a common combination especially in the elderly.
Which will you Intervene first ? Is the AV block related to CAD ?
How to differentiate Ischemic from degenerative AV block ?
Differentiating is often difficult.Even coronary angiogram may not answer the query unless it is totally normal . For AV block to occur usually LCX / RCA lesion is required. LAD lesion in isolation are rare to cause CHB .
How often re-vascularisation reverses ischemic CHB ?
Logically you expect more reversals.In real world it rarely happens.
Therapeutic options in combined CAD and CHB
PCI and pace maker in the same sitting .
PCI first followed by pace-maker at a later date.
Pace maker first followed by PCI at a later date if required.
CABG and epicardial pacemaker ( best option In all critical TVD and CHB)
Pace maker followed by CABG later
Pacemaker followed by medical management (CHB with Insignificant CAD)
Can worsening of ischemia occur after pacemaker ?
Very much possible . Since the patient has been benefited by low heart rate in terms of MVO2 consumption .(Inserting a pacemaker is like sudden withdrawal of beta blocker !)
Rate adoptive pacing can confer chronotropic competence which may bring back the angina.So,what was a insignificant lesion can become hemodynamicaly relevant and may require angioplasty later.
*The above clinical issue is applicable for sinus node dysfunction and CAD as well.
Final message
There is no fixed rule in the management strategy in combined CHB and CAD .
Generally , electrical therapy should be given preference .Symptom guided approach may be practical.
In this scientific era , one may argue to deal both issues together by simultaneous PCI and pacemaker , still option 3 and 6 remain clear favorites !
If angina occurs even in baseline bradycardia it is obvious the obstructive CAD is significant and needs immediate fixing .
Finally , though it looks an attractive concept , It is very rare for CHB to get reverted by PCI or CABG.
All left to right shunts are acyanotic heart disease to begin with. Cyanosis appears if there is progressive PHT and reversal of shunt .We know this happens late in ASD.(third decade)
It is important to remember some of the patients with large ASD can show significant desaturation without severe pulmonary HT. This should not be mistaken for Eisenmenger reaction.
How ?
In any large ASD ,
IVC blood can stream into LA by hitting preferentially the lower part of IAS.( It is the old fetal route that heart does not forget and indulges whenever the local hemo-dynamics permits !)
During straining , (Valsalva and equivalents) right atrial pressure can exceed LA and small amount of shunts occur across RA.
ASD is often (15%) associated with systemic venous anomaly. The common one is persistent LSVC. LSVC is usually connected to coronary sinus . If it has a communication with LA (Un-roofed CS) , there can be significant cyanosis .
Further , a large ASD can act as a single atrium and considerable mixing happens and cyanosis results.
Finally ,two conditions should always be considered
ASD if associated with VPS auguments R-L shunt .
TAPVC can be mistaken for Eisenmengerisation of ASD in bedside which presents as clinical signs of ASD + Cyanosis
* It is useful to recall ,even PFOs can shunt right to left at times of extreme RA pressures like during PEEP ventilation and orthostatic deoxia in sick ICU patients are reported (If PFO can shunt R-L , why not huge ASD ?)
Final message
Cyanosis in ASD is not always an ominous sign .There are few important causes other than Eisenmenger. Though it occurs intermittently , persistent mild desaturation is also possible.
Any new ST depression occurring during EST is sine qua non for inducible ischemia.But,this rule does not uni-formally apply in all 12 leads .ST depression occurring is certain leads is more important. While severe global ischemia can depress ST segment in most leads ,factually only the leads V 5 and V6 predict true Ischemia.This because , bulk of LV muscle mass faces these two leads.
Isolated ST depression in inferior leadsduring exercise
Is a frequent issue occurring at the peak exercise.
Is least predictive of significant CAD.
The exact mechanism is not clear.
Some continue to believe it is indeed significant .
We have observed isolated ST depression > 2mm in inferior leads with significant CAD.
What really matters is the quantum of ST depression , symptoms, and exercise time and preexisting CAD .
Probable mechanism
Apart from true ischemia ,ST depression may indicate relative sub endocardial strain rather than ischemia.(By the way can simple stretch can cause ST depression ?)
The Infero posterior surface of heart represent right ventricle .RV volume overlooked peaks exercise.Some think it represents acute raise in RV load during peak exercise.
How to report such EST ?
You can report it as such, what you have observed.
ST depression noted in Inferior leads at peak exercise.
Mention whether it was angina free,
At what METS,
Total exercise time .
If you are statistically inclined you can also mention the likely hood of CAD by positive predictive value (PPV) of the test (Low with isolated Inferior ST depression )
If you are really confused , and do not want to scratch your brain we have the most convenient terminology invented by cardiac physicians ie Borderline EST, or Mildly positive EST “
Should we do Angiogram for such patients ?
In this era of catching normal people who attend master health check ups for a day care CAG . . . it is not all a crime to do angiogram in a patient who shows suspicious ST depression in three of his leads (2,3,AVF) especially if he also complains of vague chest pain.
Alternate investigation
Of course , we always have the luxury of using MDCT that can stunningly photograph the coronary arteries.
It is a mystery investigation, if it comes entirely normal every one is happy.Even slightest defects in the photography has a potential to confuse both physician and the patient .
What I do ?
I hesitate to do routine CAG if ST depression occur exclusively at peak exercise beyond 10-12 METS , which disappear fast.(Many times we can apply this rule to classical ischemic ST depression of lead V4 as well !)
ST depression in any leads (with any degree) following an episode of ACS seems to be important.
The WordPress.com prepared a official 2013 annual report for this blog.
Here’s an excerpt:
The Louvre Museum has 8.5 million visitors per year. This blog was viewed about 540,000 times in 2013. If it were an exhibit at the Louvre Museum, it would take about 23 days for that many people to see it.
It all started in 2008. This is 6th year of my attempt to share knowledge in cardiology.The followers of my blog is the only strength that sustain my writing .
Wishing you all a Happy , wonderful and a prosperous , New year 2014
But . . . please be reminded we don’t require a New year to bring a bout of happiness , it is sitting right in our minds every day !
On this day let me quote my most revered quote of Hemmingway.
Ernest Hemmingway the Nobel laureate who was born in USA, Lived in Paris , fought in world war 2 , lived in the deep forests of Africa with wild animals during the fag end of his life .He had a Intimate relationship with Cuba, made a passionate appeal to end the man made disaster called wars in this planet , before his life ended in 1961.
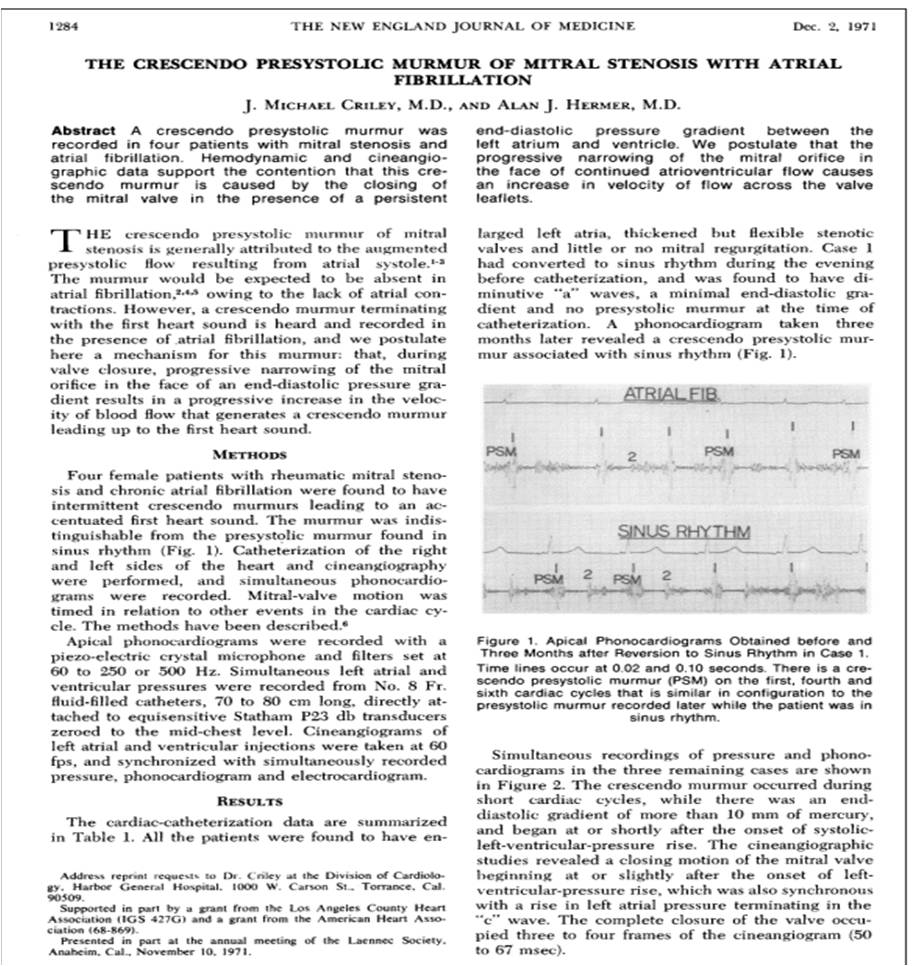
Auscultatory findings of mitral stenosis is the most common question asked in clinical cardiology right from first clinical year to higher specialty examinations . It should be answered in a systematic way.
What happens to the murmur and sounds in mitral stenosis after the onset of AF ? When I asked this question in my class , many struggled . Hence this post .
* Correction
The A2-OS interval in critical MS is relatively short and only is minimal variation is expected in spite of AF .This is because, A2-OS interval is primarily determined by instantaneous LA pressure at the beginning of MV opening which is always high and does not vary much with RR interval .
The contents of the this blog is being published as Kindle E book , as per the request of many of the readers. Every article will continue to be open source in this site. Again I shall reiterate the book format is not aimed at any commercial intent. It is only to facilitate learning in a single book format Here is the link to book https://amzn.in/d/euhL5vu
Click below to see who is watching this website live !
This site will never aim for profit. Still ,this donation link is added at the request of few visitors who wanted to contribute and of-course that will help make it sustainable .
Please Note
The author acknowledges all the queries posted by the readers and wishes to answer them .Due to logistic reasons only few could be responded. Inconvenience caused is regretted.