STEMI is the commonest cardiac emergency . Many believe , we are close to conquering it . It is hardly the truth .
- The mortality is up to 30 % out of hospital and another 6-8 % within CCU and another 2 % at 30 days due to recurrent ACS .This is followed by an annual attrition rate OF 25 due to progressive LV failure .
- The commonest mode of death is electrical, ie primary VF.
- Mechanical deaths are also equally important. Free wall rupture carries 100% mortality . Ischemic MR, Ventricular septal rupture (VSR ) may also result in deaths.
Here is a case history and ECG of a patient with STEMI .
 After thrombolysis , the paradox happened . ST elevation increased by 4mm and soon the patient became restless with worsening pain and became silent instantaneously , with monitor showing EMD and asystole .A diagnosis of free wall rupture was made.
After thrombolysis , the paradox happened . ST elevation increased by 4mm and soon the patient became restless with worsening pain and became silent instantaneously , with monitor showing EMD and asystole .A diagnosis of free wall rupture was made.

What we used refer in our CCU (Madras medical college Chennai .One of the oldest CCU in South Asia )
as “Action pontentialisation” of surface ECG . This ECG finding has great clinical significance .
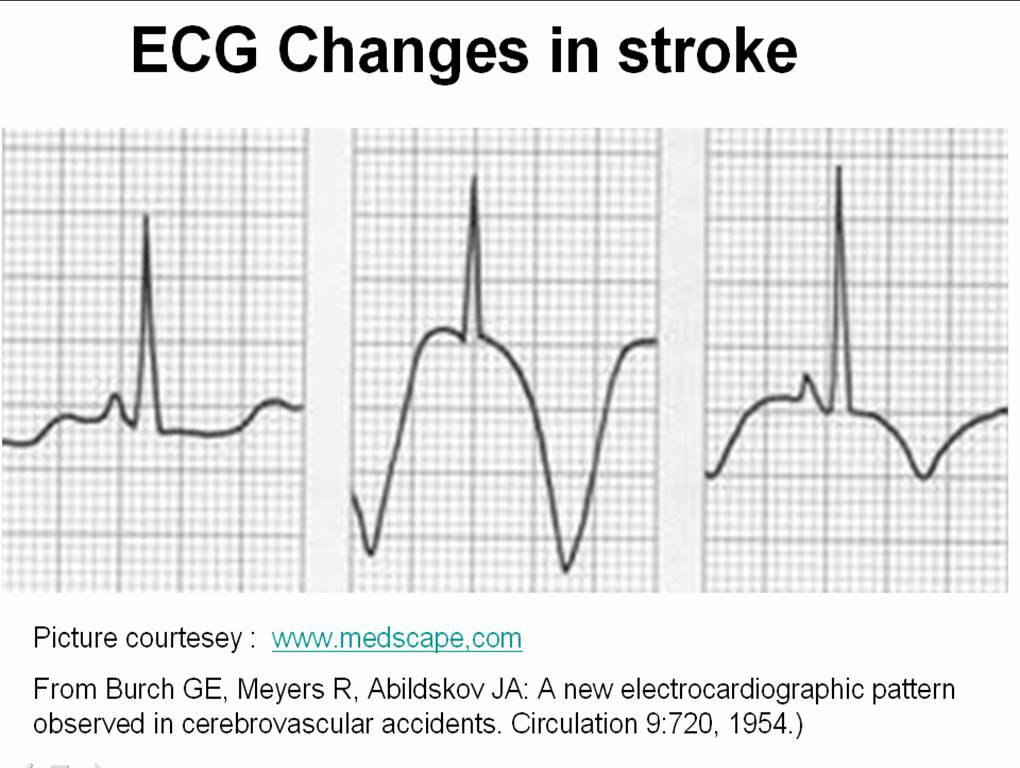
Here is a zoomed up view of a qrs complex of the patient , which is very
closely resembles an action potential

 Picture courtesey http://ocw.tufts.edu/Content/50/lecturenotes/634488/634591
Picture courtesey http://ocw.tufts.edu/Content/50/lecturenotes/634488/634591
Pathological basis of “Action potenial” Like ECG
- When the ST elevation is huge and wide it mimics an action potential .
- Myocyte action potentials are normally recorded epicardially in physiology lab where a micro electrode with glass pipettes directly enter the myocyte.
- A giant ST elevation and a sustained dome indicate , the quantum of electrical injury is very large and the ECG electrodes is picking up the myocyte electrical events like that of a intra cellular electrode.
- It is to be recognised , ST elevation in chest leads is substantially taller than limb leads because the exploring electrode is located just above the myocardium . But, when a huge ST elevation is recorded over a limb lead (as in this patient ) one can imagine , how intense the electrical charge of the myocardium should have been !
This heavy downpour of electrical energy that emanate from the myocardium means two things
- The area of infarct is very substantial
- The tissue in question is very unstable .
Clinical correlates of action potential ECG
- Damage is transmural , the infarcted area is soft, friable and often hemorrhagic .
- The pericardium is also likely to get involved in the injury process .
- The myocardium is rupture prone or already torn .
- Even minor hemodynamic stress can be fatal in these patients
- An episode of vomiting, a fall in blood pressure, an episode of LVF or a short run of VT is suffice to result in a fatality.
The death happens by a sudden rupture , EMD and asystole .
Can a life be saved by the much fancied Emergency PCI ?
Not really. The PCI can not reverse the myocardial damage , so it’s role is little . But , any way it should be done and . . . it will be done in most institutions to give the benefit of doubt (Of course , with a definite the risk of doubting !)
What is the risk of PCI in these situation ?
The infarct related artery * if opened up can convert a bland infarct into a “angry red” hemorrhagic infarct .This is as good as giving the patient , a farewell party for his journey to heaven !
Note : Primary PCI definitely saves life in STMI . The * is applicable only in persistent ST elevation , late after an acute MI.
How could have the above death prevented ?
As one of the comments to this article suggested, we need to have methods to identify impending rupture early and accurately .This should followed by a prophylactic surgical intervention (Reinforcing the friable myocardium – with a patch or mesh ) .This is again not a easy decision to make .
Final message
When the ECG assumes a shape of an action potential , it is often a sign of imminent death . Even though it may sound a pessimistic view it is often the truth . Of course , an emrgency PCI or CABG are the only options available , we have to be remember the above truth , as we play those sophisticated games within their coronary arteries.














{kind=link}