It is estimated nearly half a million PCIs are done all over the globe every year .Evaluating diagnostic angiogram is a critical vital step, but often times it is given less time and left to fellows .This is done mostly offline by Image processing software. Curiously , lesion assessment becomes a causality to the visual acuity .It ends up with lot of whims , intuition and bloated egos of senior cardiologists !
Technical issues
The fundamental flaw in the lesion assessment is ,there is a dissociation in choosing the “best view” for lesion morphology and length . Size need not be well assessed in the same view as morphology . For example , LAD is fore shortened in LAO caudal view , length measurement would be erroneous , still morphology may be well delineated .(Vice versa in RAO caudal view )
Other source of errors
Reference catheter may be far away in the Aorta , and confer a magnification error . This becomes important especially in ostial lesions and associated major branch lesions. The computer uses the edge detection algorithm which carries an inherent error .
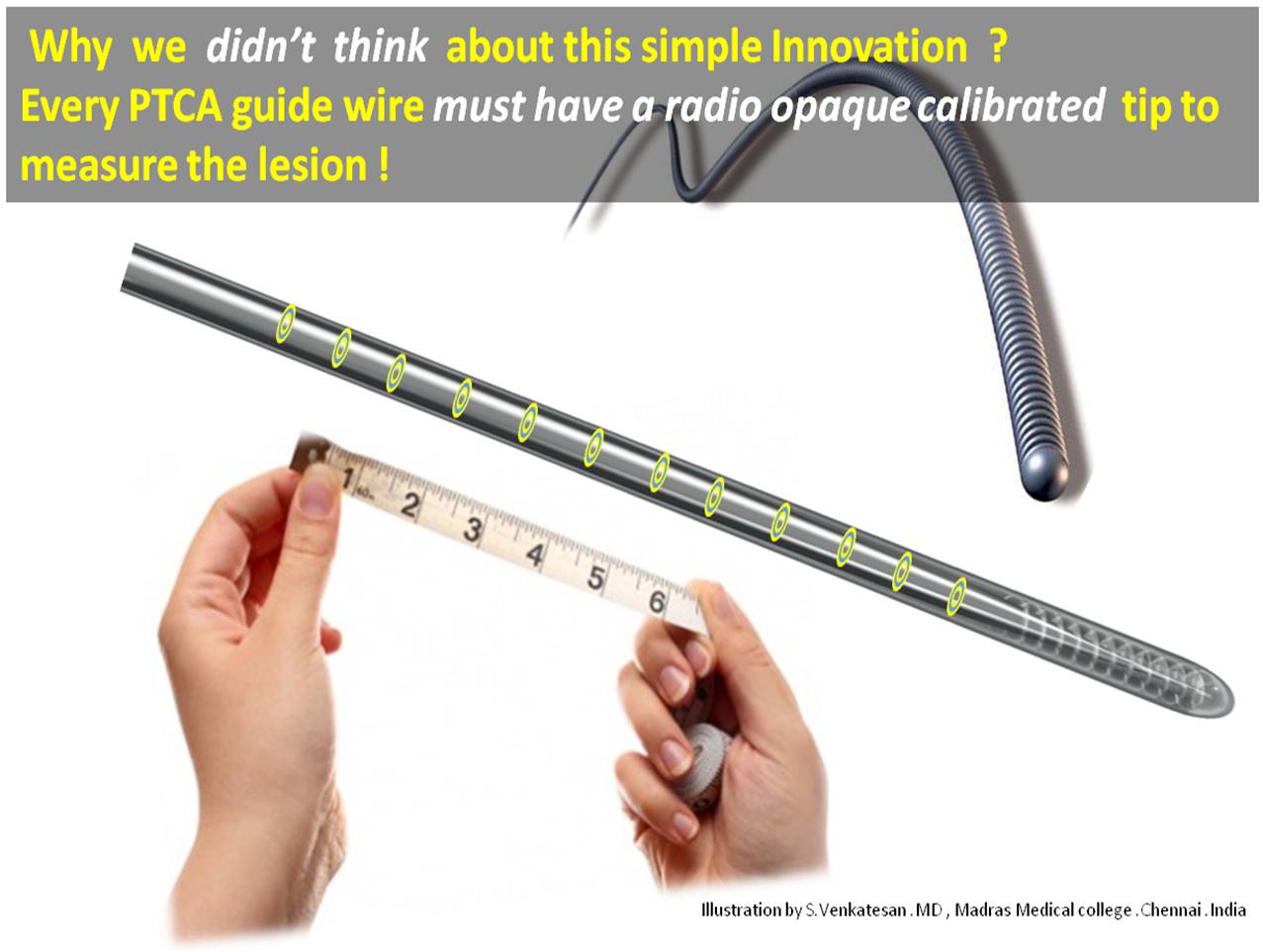
Advantage of guide wire as a scale
- Instant online measurement
- Always on . Repeatedly used in multiple views .
- You can’t ask for more accuracy .The scale is within the coronary artery hugging the lesion
- The end on view is effectively nullified .
- Magnification factor do not operate.
- Finally , and most importantly in complex tortuous , tandem lesions few mm errors can be disastrous .These calibrated guide wires will make our life lot easier.
Final message
Measuring a coronary lesion remains a delicate issue . If only we have radio opaque rings every 1mm or so in the distal end of the guide wire , we can measure the lesion instantly and most accurately.
This will definitely make our life not only simple but help our patients with accurate stent sizing and avoid costly geographical miss (or inappropriately long stent that increase metal load .)
After thought
I do not know whether any of the existing guide wires have this facility .(I guess it is not . . .then , let this idea be patented in my name !) After all , It is a mean task for all those mighty coronary hardware companies to add few radio opaque rings to all PTCA guide wires!
Medtronic, Abbot, Boston are you listening ?
And . . . your opinion please !