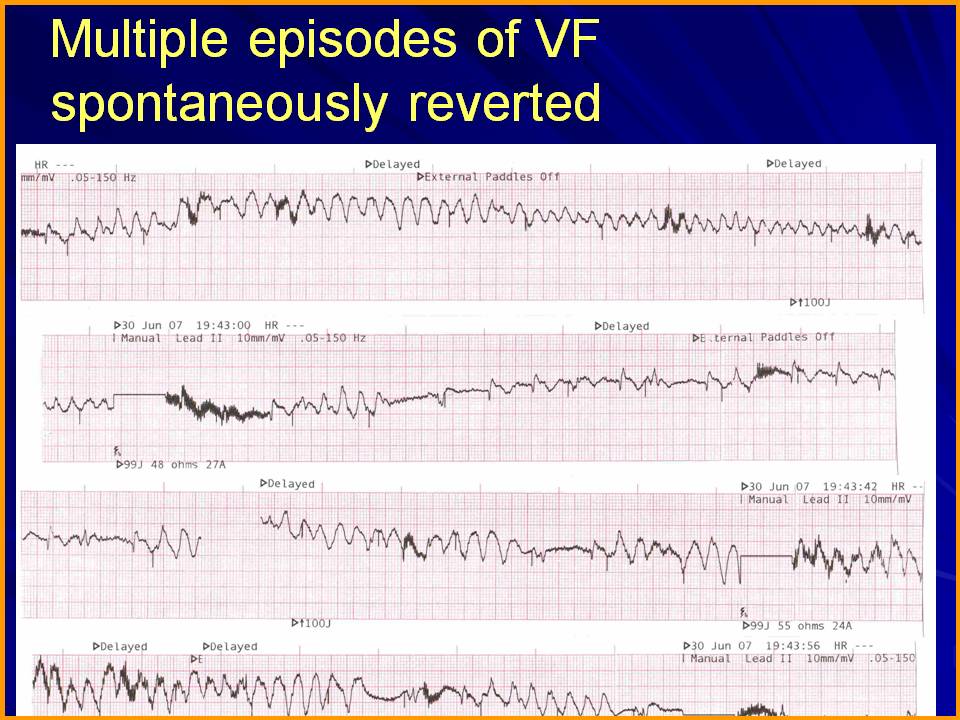
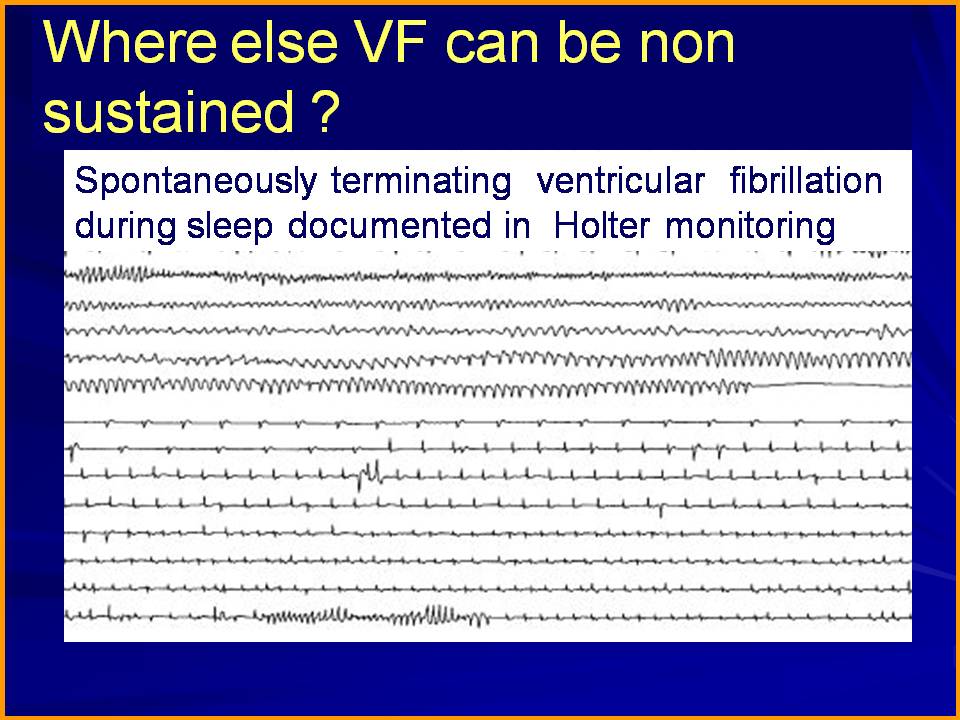
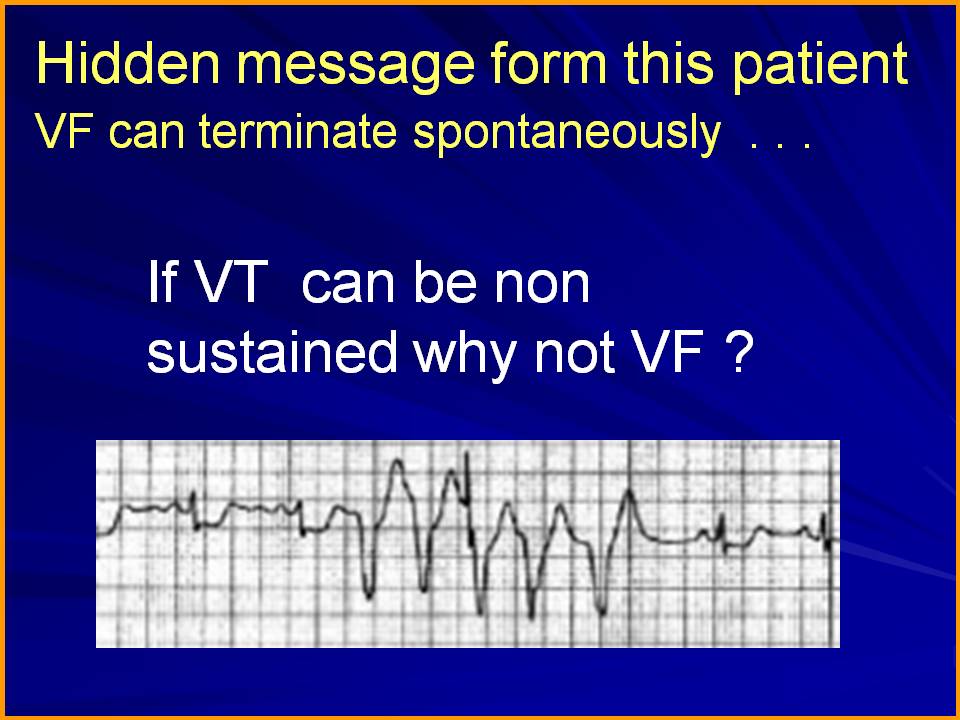
Can VF be a non sustained arrhythmia ? This question was raised and a single case report was presented
in the annual scientific sessions of Cardiological society of India Meet in year 2008 in Chennai.
I am just reposting it from my archives .

Can VF be a non sustained arrhythmia ? This question was raised and a single case report was presented
in the annual scientific sessions of Cardiological society of India Meet in year 2008 in Chennai.
I am just reposting it from my archives .
Posted in cardaic physiology, cardiac physiology, Cardiology - Electrophysiology -Pacemaker, Cardiology -unresolved questions, My presentations | Tagged mechansim of ventricular fibrillation, non sustained ventricular fibrillation | Leave a Comment »
Myocardial salvage is like coronary fire fighting.When fire is fought very early after the accident , benefits are accrued more . Text book primary angioplasty is . . . fire engine arriving at the scene when the house is on fire .
Rescue angioplasty is asking for more force , when the initial fire fighting was inefficient to control the fire. So , it is obvious the rescue efforts should be fast and brisk.In fact the pace should me more than the primary (The the second engine should reach the ground zero faster than the first ! – Read as door -balloon time ! )
But what happens in real world ? We would tell time window for primary angioplasty even in sleep ! but will struggle to come with clear cut answer for the same in rescue angioplasty even in a fully awake state !
It is an overwhelming fact , we have not taken enough efforts to define strict time limit for rescue .( Even though guidelines say it should not be beyond 24 hours , common sense will tell us rescue PCI should not go beyond 12-15 hour window ! .One more definition for rescue PCI could be within 3 hours after diagnosing failed thrombolysis. In real world it is a race against time in a different perspective .In many centers rescue angioplasty “enjoys time less windows “
I was funny witness in a big private hospital when a colleague of mine has posted a case for “elective rescue angioplasty” and was waiting in the side cabin for his turn !
Coming back to the title question
Why we often follow a reckless time window for rescue Angioplasty ?
The reason is simple
Time is not only muscle . . . time is money too !
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care | Tagged concepts in primary pci, ethics in cath lab, indication for rescue angioplasty, rescue angioplasty, salvaging myocardium, time window for rescue angioplasty | Leave a Comment »
An elderly man with past H/o CAD was admitted with ischemic LVF and hypotension .Blood pressure was 90/60 mmhg and pulse rate was 140 . Urine urine output in the immediate past hour was 50 ml . Saturation was 95 % .He had fairly extensive crackles in both lung fields.
A bed side echo showed moderate LV dysfunction , with wall motion defect in LCX territory and mild MR .A dignosis of post MI -ischemic LVF was made .
He was put on intensive anti failure protocol. I asked my fellow to administer IV NTG and left the ward .
On my next visit after few hours . . . the patient was in much bad shape , and when I enquired , I learnt NTG was never administered . I was curious to know why the fellow dis- obeyed my instruction .
He felt sorry . . . But he earnestly told me , he could not comprehend the principle of administering NTG in a patient with shock ! . I was happy to note his genuine concern for the patient ! But . . . I had to take a brief lecture to convince the importance of NTG in some forms of shock !
What is the cause for hypotension in ischemic LVF ?
Lungs are flooded due to very high LVEDP . Blood not only struggles to enter the LV but also finds difficult to leave the LV , former due to defective relaxation later due to poor pumping.
The extremely high pre-load actually stuns the left ventricle in diastole . (Primarily diastolic stunning ) . Here is a hemodynamic paradox . Excess pre-load occurs in terms of pressure , but in terms of volume there is miniscule amount blood that traverses LV .
This is pre-load mismatch at play .Empty ventricles with high wall stress and that is reflected in aortic afterword as well .
We have to some how reduce the very high levels of LVEDP . IV NTG can dramatically reduce the pre load ( and reduce the LVEDP .) The other major benefit is , NTG can reduce the MVO2 by improving sub endocardium coronary perfusion and de-stress the heart.
Once LVEDP is lowered , the ventricle will tend to recover and gain at least some original elasticity ( Frank starling forces) . Of course it will be defective due to ongoing ischemia . Even slight fall of LVEDP (say from 25 to 18 mmhg can have significant benefits as the LV function curve labors on the steep shoulder region !) .
This is one situation where NTG can increase the blood pressure once the hemodynamics is favorably altered.
*Yes . . . heavy doses of Frusemide injection can do the same job but it largely depends the kindey’s cooperation to flush out fluids .In a shock like situation one can trust the kidney perfusion !
Additional benefits of NTG
Mitral regurgitation is a serious destabilizer of LV function .NTG can reduce the regurgitant fraction in acute MR effectively .
Caution
NTG may worsen the hypotension of RV infarction . Make it very sure , you are not dealing with this unique pre-load dependent circulation.
What happened to this patient ?
He did show improvement with IV NTG . Of course it was not dramatic as I have projected in this article .Still it was really helped him .He required simultaneous dobutamine infusion as well .The BP did not fall further and lung congestion was relieved .He went on to recover fully by 48 hours and was posted for elective cath study .
Final message
We tend to worry more about falling blood pressure when administering NTG. . .It is a wonderfully effective drug especially in the setting of ischemia and cardiac failure even if the blood pressure is low !
Acute cardiac hemodynamics is complex phenomenon .No one has mastered it .Paradoxes are common . Hypotension in the back ground of acute pulmonary edema especially due to ischemic LVF can be corrected by NTG . Of course physicians need some courage to administer NTG in patients with a systolic pressure of 80-90mmhg.
This should ideally be done with intra arterial line in place and a simultaneous inotropic line (Doubtamine /Nor-epinephrine ) back up in case of worsening perfusion pressure .
Posted in cardiology -Therapeutics, Cardiology -unresolved questions, cardiology- coronary care, critical care ccu | Tagged 90mmhg and ntg infusion, balanced vasodilatation with inotropic support, ischemic lvf and ntg infusion, iv nitroglycerine in acute pulmonary edema and shock, nitroglycerine, shock and vasodilators | Leave a Comment »
Acute MI kills a few million people world-wide every year .It does not differentiate rich from poor. Logic would tell us , principles of management should not differentiate the people when dealing with a myocardium in distress .
Unfortunately , we scientists do it with passion !
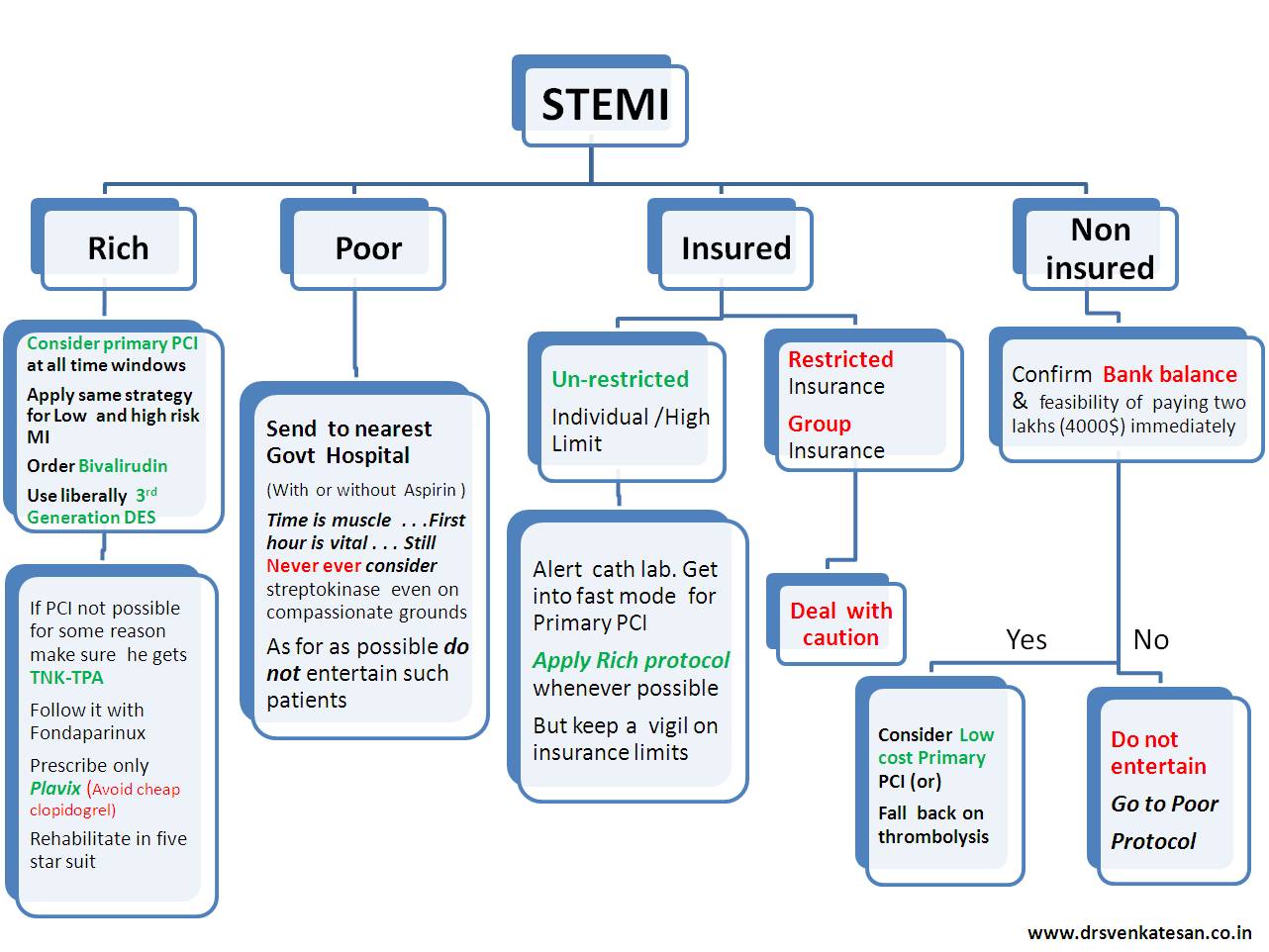
The problem is enormous . . . the rich is suffering from too much* care and the poor is suffering from want of care !
The following flow chart is a result of my observation from close quarters about the management strategies in corporate as well as Govt hospitals .
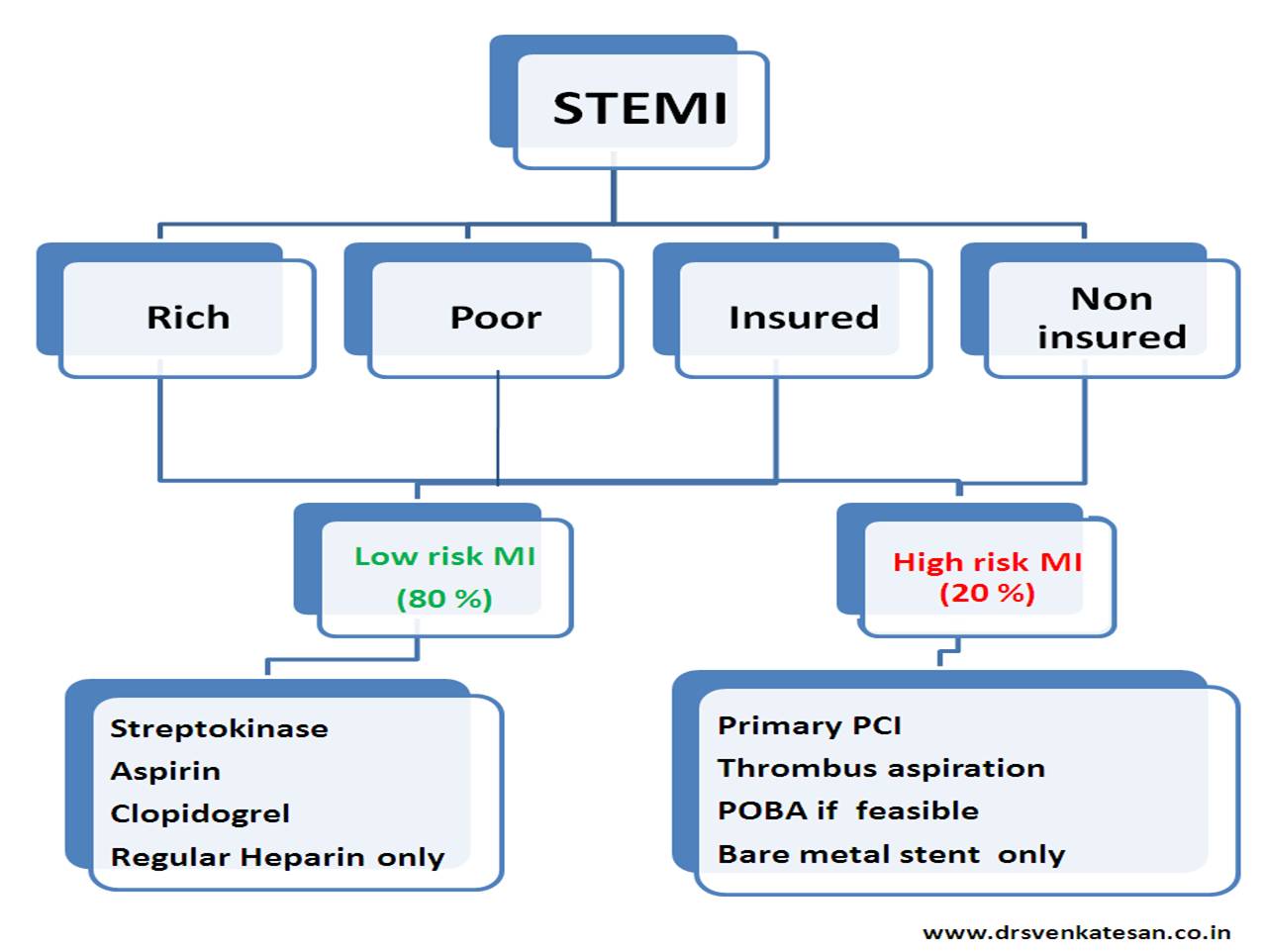
The first chart exposes the problem .The second one tries to address the issue
Please bear with me . . . if the stuff sounds too crazy !
* Too much care is also referred to as inappropriate care
And for the solution . . . try this
Posted in Cardiology -Interventional -PCI, cardiology -Therapeutics, cardiology- coronary care, cardiology-ethics | Tagged commercial guidelines for stemi, etical guidelines for stemi, guidelines for stemi, primary pci thrombolysis | 1 Comment »
Soft skills in pPCI
Experience would tell us only about 70-80 % of STEMI are truly eligible for a good quality pPCI .(Multivessel CAD, Complex bifurcation lesion, difficulty in identifying IRA, No IRA-sapsms , complete spontaneous reperfusion ) The remaining 20-30 % should , logically be included in the failed pPCI category .This fact is largely concealed in the literature .
Beware of huge thrombus load in every patient with STEMI .The contribution of mechanical occlusion vs thrombus (in the total occlusion ) is the single most important factor in determining the intervention strategy.
Deploying a stent in a poorly prepared (debrided of thrombus ) lesion confers further continuous risk of a STEMI .Stents smartly jail even large thrombus against the coronary vessels and they release it into the lumen in a controlled fashion and prolong the acute coronary risk phases
If thrombus aspiration does a neat job and establishes a good flow , if the lumen appear good , think twice or even thrice before deploying a stent .It is akin to stent a zero % lesion and we know it is foolish to do that at any stretch of imagination .(Stenting has never been proven to convert a vulnerable ulcerated lesion into stable one )
IVUS, OCT are not the answer in the above situations as we are dealing with emergency coronary fire fighting !
Of course the intensive anti-platelet protocols , will take care of potential after effects of the intra coronary contact sport we play ! . But . . . there is a limit for every thing. So spend as little time as possible when attempting catheter based reperfusion during STEMI.
Posted in Cardiology -Interventional -PCI, PCI PTCA Hardware, STEMI-Primary PCI | Tagged export catheter, pPCI, priamry pci, pronto v3, soft skills in pci, thrombus aspiration during primary pci, tips and tricks in primary pci | Leave a Comment »
In the early 20th century , Waller invented the ECG machine. Wilson created leads and methods to record it. Eienthoven formulated the concepts the electrical theory behind ECG.
Between 1940-197os one man ruled supreme in the world of electro cardiography . He is Dr Sodi pallares from Mexico. His deep insights revolutionised and helped us understand how the cardiac electricity is generated and propagated in various pathological states that is the beginning new age electrocardiography! It adds much to his credit , as in those days scientists from non American and European countries were hard to come in the global limelight.
Some of his thought processes and Inventions
Please remember , Sodi pallare’s conscience is still largely unexplored .There are lots of hidden truths .We now know fever can influence qrs voltage and febrile illness can trigger ventricular tachycardia as in of Brugada syndromes.
Today’s youngsters can take a few cues from this great man and enlighten the field of electro-cardiology

Demetrio Sodi Pallares (1913-2003 )
If modern-day cardiologist is able to interpret the ECG by a cursory 3 second scan of strip of waves , we are greatly indebted to the knowledge imbibed by this great man from Mexico !
Reference
http://onlinelibrary.wiley.com/doi/10.1002/clc.4960110616/pdf
Posted in cardiology -ECG, Great websites in cardiology, history of cardiology | Tagged history of cardiology, sodi pallares ecg mexican cardiologist | Leave a Comment »

mid diastolic murmur in sinus rhythm
With the onset of Atrial fibrillation
Link to Echo Image of Mitral stenosis .
https://www.youtube.com/watch?v=3qvOMwOshg4
How to assess the severity of MS in the presence of AF ?
Other signs are often useful
Low volume pulse
Inconspicuous LV impulse
Presence of any significant Pulmonary hypertension
Posted in Cardiology - Clinical | Tagged effect of atrial fibrillation on mdm opening snap pre systolic accentuation, mdm of ms, mitral stenosis | Leave a Comment »
Squatting is a simple physical maneuver that can be done in bed side.
It is ideal to do “Stand -Squat -Stand” sequence to appreciate the attenuation during squatting and augmentation during standing

Hemodynamics
MVPS-MR is a pre load (LV volume ) dependent phenomenon.The degree of prolapse is inversely proportional to the LV size.
Squatting increases the venous return and after load both tend to increase the LV volume. More blood in the LV , means mitral leaflet floats much closer to the mitral annulus . Hence the force of LV contractility is not only less on the prolapsing leaflet , it reaches late , hence the click is delayed and murmur is short (It may be less intense as well * )
(* Squatting increases aortic after load hence the murmur of MR may get amplified .)
Reference
Posted in Cardiology - Animations, Cardiology - Clinical, Clinical cardiology, dynamic auscultation, valvular heart disease | Tagged dynamic auscultation, lv cavity during squatting, squatting increases venous return and preload, squatting mvps click occurs later murmur shortens, standing increases mvp murmur | Leave a Comment »
We know new onset LBBB creates considerable anxiety . We experienced a reverse situation recently . A 72 year old man who is known to have chronic LBBB for over 5 years came to CCU with vague chest discomfort .
His ECG was perfectly normal . . . every one was curious !
![]()
![]()
My ECG always looked like this doctor ! Now you say it has normalised and you say it concerns you ! I am really worried doctor !
What does it mean doctor ?
Cardiologist : I do not know . Any sudden change in rhythm even if it is from abnormal to normal is to be given importance .
Patient : Is the going bad ?
Cardiologist : I do not know
Patient : Should I get admitted ?
Cardiologist : I think so but you need to undergo few blood tests and repeat an ECG .
Patient : Oh what ? you are not sure either ! Are you not an expert in heart disease doctor ?
Cardiologist : I think I am . I wish I have an answer to your question .
Follow up
This patient was admitted in intermediate care ward and observed for 12 hours .
His enzymes and Troponin were negative . Echo showed normal LV function .
He was discharged later and adviced a stress test .
What is the the mechanism of normal ECG here ?
Intermittent LBBB due to rate dependency is common .But this man had persistent chronic LBBB for > 5 years which got normalized .That mystified us !
Can transient ischemia of left bundle accelerate the conduction ?
Posted in cardiology -ECG, Cardiology -unresolved questions, Cardiology-Arrhythmias, Cardiology-Coronary artery disese | Tagged intermittent lbbb vs intermittent normal ecg, lbbb, new onset lbbb normal ecg, transient lbbb | 4 Comments »
Sinus node is the electrical high command of our heart .When it gets injured seriously (or shot down as in sinus arrest ) there is utter chaos in the lower ranks !
This is what happened in this patient .
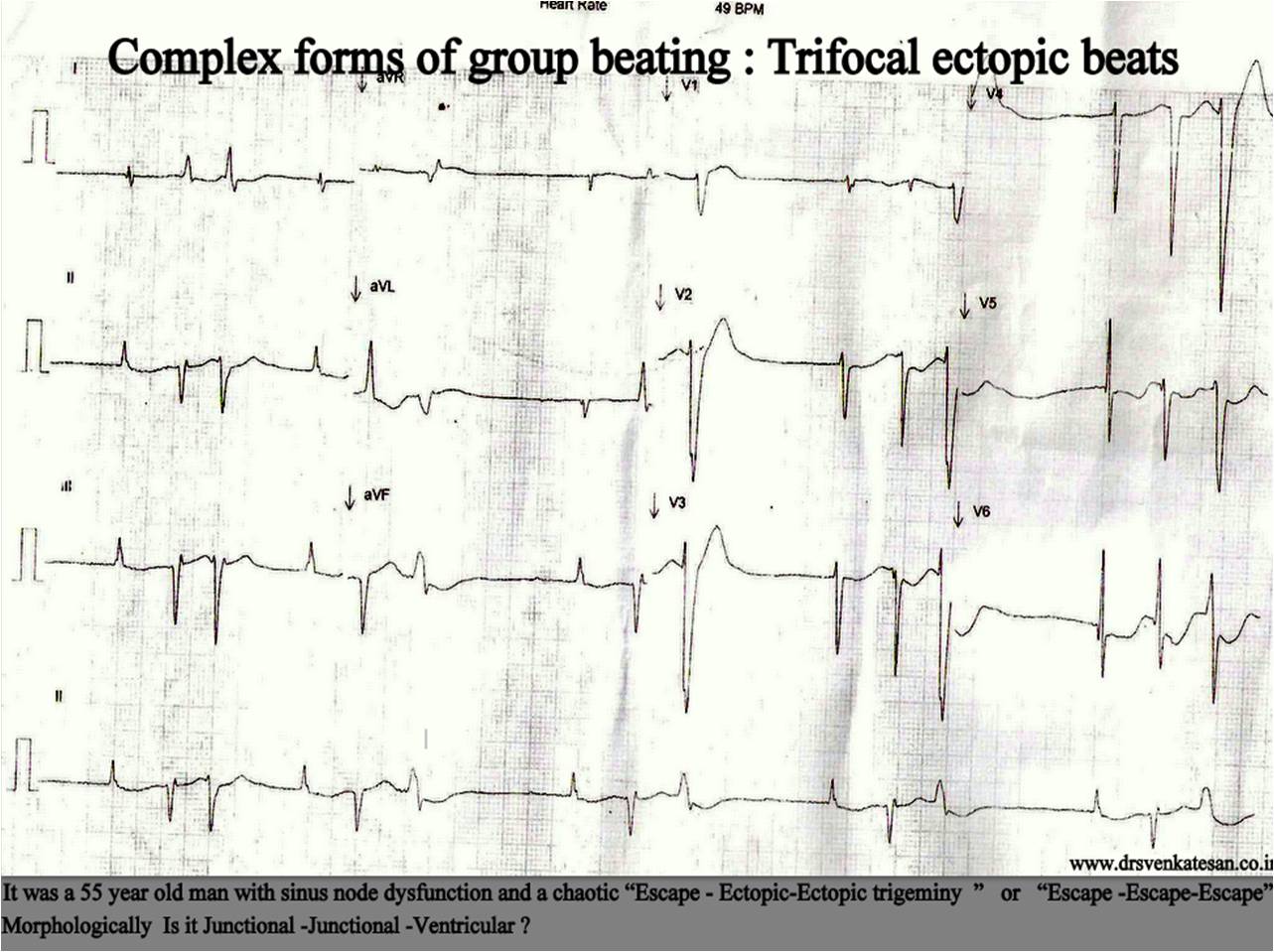
The lower pacemkers can either passively release themselves as escape rhythm or actively fire with a ectopic focus . Any combination of escape / ectopic beats can occur .If occasional sinus beats capture the ventricles things can become further complicated .
It is obvious , this random intra-cardiac shooting makes the life of the myocardium miserable . It is a perfect setting for syncope, tachcyardic cardio myopathy , extreme brady induced VT , VF even SCD.
*Meanwhile , It is heartening to note SND rarely lead to sudden death in spite of all the chaos .However extreme bradycardias that occur in complete heart block does not enjoy this immunity as fatal complications are common if not intervened .
Posted in Cardiology - Electrophysiology -Pacemaker, cardiology -ECG | Tagged abberrant conduction in apd jpd, apd, apd jpd vpd, escape caputre escape ectopic trigeminy, group beating ectopics, jpd, pause dependent vpds, premature ventricular beat, sinus arrrest and jpd vpd, sinus node dysfunction snd with escape and ectopic rhythm, VPD | Leave a Comment »



