I stumbled upon a TV reality show where a mother of a child was crying inconsolably ,whom she lost when it fell into a open bore-well pit .She was blaming it as her fate and the hole was sent by Lord Yama (God of death )
I just got curious ! This article was written in a flash.
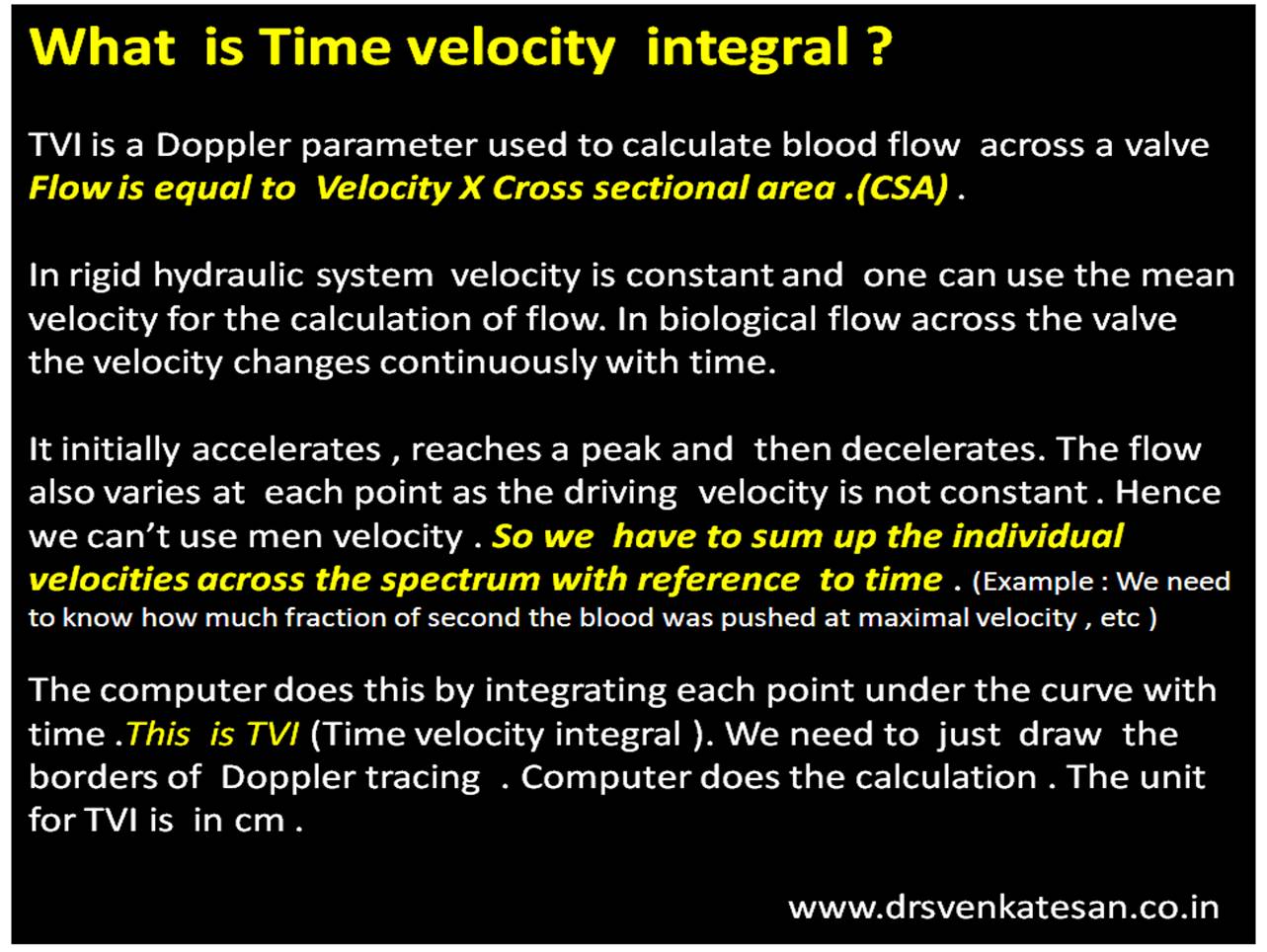
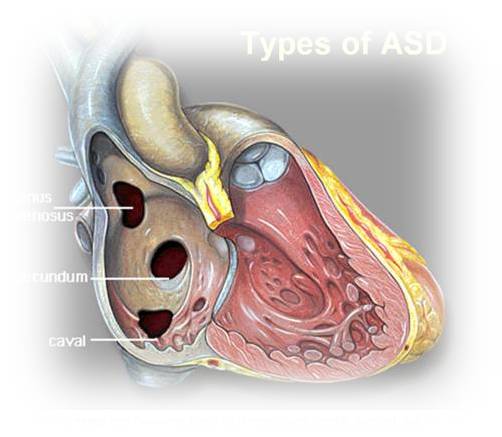
I used to get questions from anxious parents of children with holes in the heart .(Asymptomatic small VSDs or ASDs who come for periodic echo-cardiograms) .I reassure and convey the message , most of these holes are tiny and will close automatically and they need not worry.Even if it doesn’t, it poses little problem.

But .after watching that haunting TV show, I have started to warn the parents that holes in the heart may not be that dangerous but be wary of holes in the roads and unclosed bore wells in our country !
Every single parent was amused with my statement ! Some how it appeared sense to me !
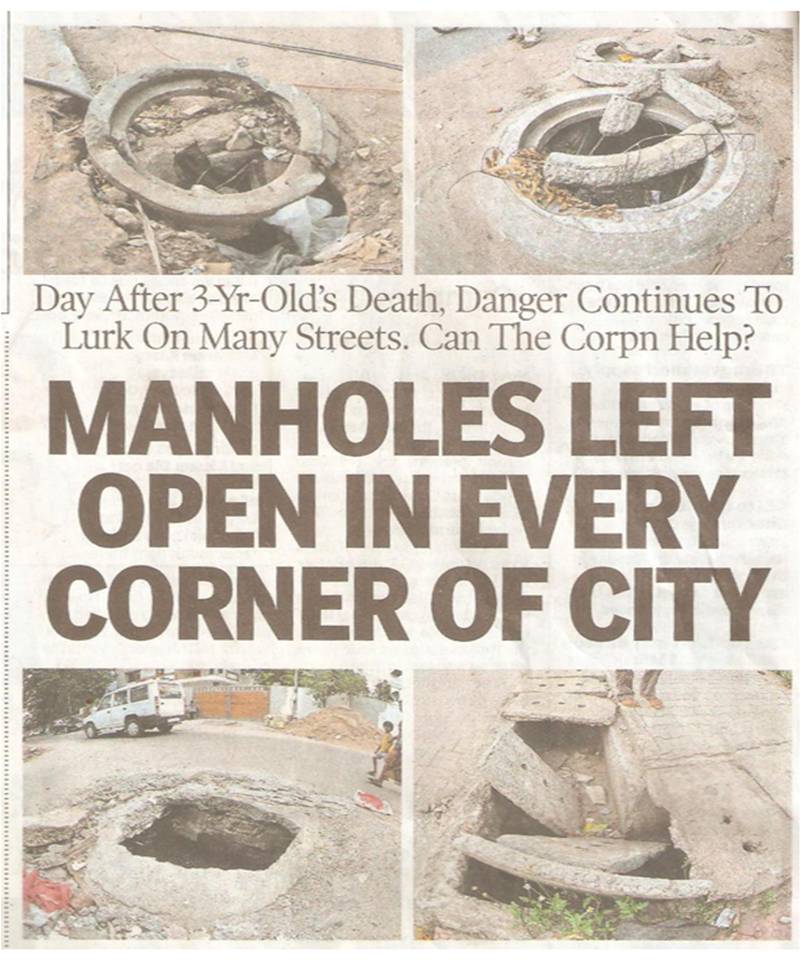
I made a mini google research. It is estimated thousands of bore-wells are dug every day and kept open in allover the country side .It is like live land mines . Some press reports suggest at least one child dies in India every day due to uncovered bore-wells and man holes ! (May be really true !)
The following are some of the samples.
One

One more

Two
You can understand the gravity of the problem , one engineer has devised a special child retrieval Robot for such accidents.

Three
A news report in Times of India .What shall we do about these ?

It is a horrific truth in this civilised world .Nature creates holes in the heart due to defective gene in some . It appears less dangerous to me. After all a hole in the heart threatens only one life,while a hole in the road kills many people.
As a cardiologist , I am saying this with anguish as our team along with surgeons work over time to close intra-cardiac holes with device , the holes in the road are often callously kept open forming death traps for our children .The men responsible for such things deserves no pardon.
The story is never ending . . .

Post-amble:
Doctors are not just the noble professional who provide relief from illness . They have other social responsibilities too !
I believe , as physicians bound by Hippocratic oath , we should help tackle issues that threaten our pubic health system , especially in this case were the victims are vulnerable children !
In fact , pediatricians should come forward to work with Govt to improve safety issues for children and orthopedicians should help prevent road traffic accident while cardiologists shall work with the Govt to prevent heart disease . . . etc etc .
Though bore-well deaths are a pan India phenomenon , One state in India ( TN) has taken a new initiative recently and has banned digging bore-wells without prior permission and stipulated strict guidelines .Others can take a cue from here !