
Original article
Chevalier B, Glatt B, Royer T, Guyon P. Placement of coronary stents in bifur-
cation lesions by the ‘culotte’ technique.Am J Cardiol 1998;82:943 – 949
Posted in cath lab tips and tricks | Tagged cullotte technique for bifurcation, ptca pci tips | Leave a Comment »
The humble looking strip of ECG recorded in millions , every day across the globe has a complex definition.
And this definition is the most apt I have found.
An electrocardiogram (ECG) is a curve showing the potential variations against time in the whole body stemming from the heart, which is an electrochemical generator suspended in a conductive medium.
Einthoven(Dutch) is the the man who invented the ECG , got a Nobel price for not only inventing the string galvanmeter to record ECG, but also making us understand the rules of the electrical wave front that emanates from the heart.( Not to forget the original concept of who demonstrated electrical activity from heart by by capillary electrometer. by Waller.(British). In my opinion waller should have shared the Nobel prize. I am sure ,even Einthoven would agree to it.
Of course , do not ask which comes first ” Ionic flow” or “the current” that comes with it !
Credit goes to the creators of this wonderful book on medical physiology and put that free on the net . Three cheers to them .
The book is from University of Copenhagen , Pannum Institute of Medical Physiology.

Posted in cardiology -ECG, Cardiology journal links, Cardiology teaching websites, Infrequently asked questions in cardiology (iFAQs) | Tagged action potential ecg, definition of ECG, history of ECG, ionic currents in ecg | Leave a Comment »
Posted in cardiology -Therapeutics, Cardiology-Coronary artery disese, Uncategorized | Tagged beta blocker anti anginal action, mechansim of angina relief by betablocker, mechansim of beta blcoker action in stable angina, sub endocardial flow | Leave a Comment »
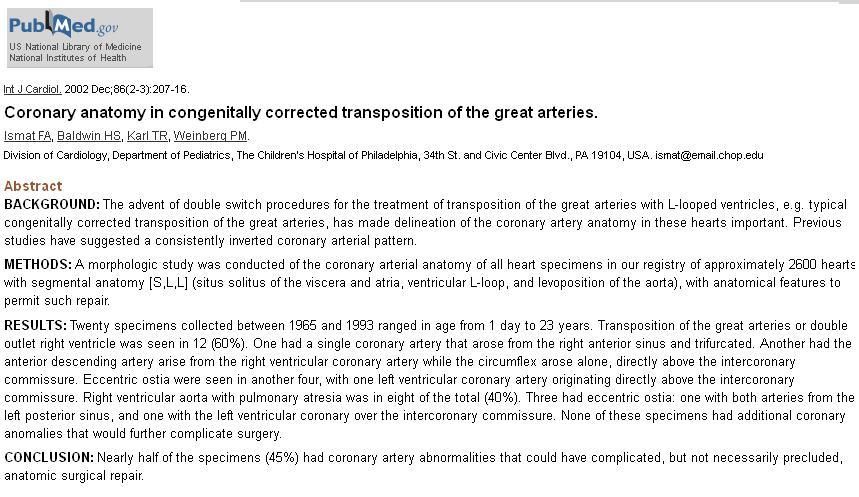
In L TGV ventricles are Inverted . Since , coronary arteries go with the respective ventricle , LAD originates from Right sinus , and RCA arises from Left sinus . (Complex anomalies in origin, course still possible ) LAD supplies venous ventricle . RCA supplies systemic ventricle .
The most surprising Irony is that major epicardial branches run in their respective grooves in the bulk of the patients with L TGV .The LAD runs in anterior interventricular groove and LCX in left AV groove etc. (That’s real power of nature , these epicardial branches home in to their grooves even in the midst of bizarre AV and VA connection !)
Here is the the ultimate reference article ; A study from 255 hearts with C TGV . I wonder , we will never get a study like this !

Questions to ponder
Implication in surgery
Progressive RV dysfunction is a major determiant of long term outcome . Unless we do an arterial switch diverting respective ventricular flow it is not going to help much in the long term
Posted in cardiology -congenital heart disease, Cardiology-Land mark studies | Tagged coronary angiogram in ctgv ltgv, coronary artery inversion in ctgv ltgv, lad from | Leave a Comment »
Wandering pacemaker is benign cardiac arrhythmia . The only danger is , it can create false alarm .This patient was referred as AV dissociation

Posted in Cardiology-Arrhythmias | Tagged changing p wave axis, coronary sinus rhythm, p wave twist, wandering pacemaker | Leave a Comment »
In the 2013 American diabetic association(ADA) annual meet a paper was presented which raised many eye brows ! . The results were flashed across mainstream media. Published in New England journal of medicine online.

It may be a well conducted trial but poorly interpreted one . It reports one of the dubious observations as a major conclusion and confuse the public.
Life style modification is the key to prevent major diabetic and cardiac events . This is well proved beyond doubt.
Epidemiological evidence from various global health statistics accumulated over a century will vouch for primary prevention of diabetic and cardio vascular disease .
Link to Editorial on Look Ahead : http://www.nejm.org
Why this study wants to make a mockery of this fact ? .Fortunately the accompanying editorial has realistically reported the implications of this study.
Final message
I argue the medical fraternity and patients to ignore this study . It can be convincingly concluded something is seriously wrong with the outcome analysis , however modern may be the statistics. Some groups are obviously worried about the natural and effective control of diabetic by good life style alone . It is a clear case of confusing the public .
There is huge collective evidence and common sense for the increased physical activity to reduce cardio vascular risk (INTERHEART)
Final Message
If life style modification is not going to help . . . what is the alternative to our patients ?
Drugs . . . yes . . . one has to depend on it . . . this study seems to suggest .
To me, this is a dangerous study . It plays a spoil sport on a great fact and belief . This paper should never have been published in a journal like NEJM . Atleast the conclusion should have been re-written !
I guess this study would promote the Homo-sapiens to be inactive and make them diabetic and consume drugs perennially !
Reference
Posted in Diabetes and Heart, Social medicine | Tagged american diabetes association, diabetes and life style, Look Ahead | Leave a Comment »
This is a wonderful and realistic article on the Issue by none other than former Health secretary of the Government of India Ms Sujatha Rao

http://www.thehindu.com/opinion/lead/doctors-by-merit-not-privileg
Posted in bio ethics, Medical education | Tagged ethics in medicine, Medical education in India, private medical colleges In India, Waht price medical degree | Leave a Comment »
I stumbled upon this web site . I think this can be glorified as the standing example for “Democracy of science”

http://www.intechopen.com/subjects/cardiology-and-cardiovascular-medicine
Posted in cardiology innovation, cardiology journal club, Cardiology journal links, cardiology journals, Cardiology teaching websites, Cardiology-Land mark studies, Great websites in cardiology | Tagged great learning websites, INTECH open science open mind, OPEN ACCESS JOURNALS, SCIENTIFIC DEMOCRACY | Leave a Comment »
Doctor , I am getting sudden compressing type of pain which starts in the centre of the chest and soon transmits to the left shoulder and gradually reach the inner aspect of the hand up to the little finger . And occasionally it is very severe and some times i feel like sweating as well ! I am unable to predict when it comes doctor !
Final message
Pain is a feeling . It can be perceived at multiple levels . The site of origin , spill over on transit and at the level of brain . A patient with multiple potential source for pain can either summate , deduct , reflect or cancel out .This can confuse the clinician in a dramatic fashion as it did to us ! . To complicate the matters further , gastric pain can trigger a cervical pain and vice versa . (Spill over effect)
Posted in cardaic physiology, cardiac physiology, Cardiology - Clinical, Clinical cardiology | Tagged atypical chest pain angina, classical angina, clinical cardiology, differential diagnosis for chest pain, gastrits and cervical spondylosis equals angian | Leave a Comment »
Only fools will manage unstable angina medically !That was exactly the statement , one popular Interventional cardiologist told a small gathering in one of the weekly meet . Do you agree ? Answer We can’t make a blanket statement like that . We have clear guidelines (Of course as licensed and certified cardiology practitioner you have every right to violate it !) . UA is risk stratified in Low , Intermediate and High risk categories .Only high risk group require emergency Intervention .Even in high risk group there are some reservation.(ICTUS study ) There are some very mild forms of UA (High grade stable angina precipitated by an emotional stress will exactly mimic UA. Similarly most secondary UA due to tachyardia , Anemia etc should not cause an alarm .) *Please note , currently coronary angiogram is included in medical investigation in most patients with UA . The confusion in interpreting such statements is partly because many physicians/ cardiologists consider doing a coronary angiogram by itself an Interventional management Reference
Posted in Cardiology -Interventional -PCI, cardiology- coronary care | Tagged ictus study unstable angina, pci for unstbale angina, risk stratification of nstemi, unstable angina nstemi medical management | Leave a Comment »



