September 28, 2008 by dr s venkatesan
The pleura and pericardium are very close anatomical companions within the thorax. Both contain minimal levels of physiological fluid. It is quiet common to find combined pleural and pericardial effusion. While the commonest explanation for combination of pleural and pericardial effusion is inflammation of both in systemic disorders like polyserositis or malignancy . In cardiac failure also both effusions can occur explained by raised venous pressure.
But there has always been a curious relationship between these two spaces.
Is there a antomical or physiological link between these two spacs ? In fact a large pleural effusion some times result in sympathetic pericardial effusion. Tapping of pleural effusion may regress this pericardial fluid as well.
This is purely a clinical observation and needs an explanation .It is believed , there is some non functional lymphatic channels shared between pericardial and pleural spaces.This may get opened up in pathology of either of them.

Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged anatomy of pleura, cardiology, chest, drsvenkatesan, pericardial effusion, pleural effusion, pleuro pericardial rub, pleuropericardial effusion, polyserositis, sle, thorax | 1 Comment »
September 28, 2008 by dr s venkatesan
Heart is externally covered by two layers of pericardium . Pericardial space is formed between parietal and visceral layers of pericardium . It is a narrow space which is normally lubricated with pericardial fluid up to 25ml. When these two tissue surfaces come into contact , pathological rub takes place.It is heard whenever the pericardium is inflammed . Pericardial rub is a distinctive but uncommon clinical sign .
Common clinical conditions
- Acute pericarditis
- Uremic pericarditis.
- Rheumatic pericarditis
- Post myocardial infarction
Pericardium has two layers .
There are four possibilities for pericardial rub to take place.
The rub can occur
1.Between the two layers of pericardium
2.Between the visceral pericardium and the epicardial layer of heart*.
3.Between parietal pericardium and the chest wall
4.Pericardium can rub with the adjacent pleura( Pleuro pericardial rub )
The second and third mechanisms are very rare.
An update
We have realized one more possibility . Diaphragm forms the floor of the heart on which the hanging heart rests . Rubbing of pericardium over diaphragmatic surface is a beat to beat affair that lasts the entire life !. In inflammatory states of diaphragm especially the contagious ones from abdomen , can result in pericardio- diaphragmatic rubs .These rubs are almost impossible to hear clinically.

*The anatomic mystery : Is epicardium same as visceral layer of pericardium ?
Some anatomist feel that both are same entities. If that is the case myocardium can never split its relationship with visceral pericardium.But it is also a anatomical fact visceral pericardium engulfs the coronary artery and are located sub epicardially.

How many components of pericardial rub are clincally heard ?
Pericardial rub classically has three components. Systolic, mid diastolic, and pressytolic atrial components. Pericardial rubs are typically described as to and fro rub. Systolic component is most consistent. In atrial fibrillation mono component pericardial rub is heard.
Quality
Superficial , scratchy, high pitched ( Can also be low pitched)
Location
Left sternal border , left 2nd or 3rd space .Best heard in sitting , leaning forward in inspiration. Many times the rubs are transient and evanescent . Since it has multiple components it may be mistaken for added heart sound like S 3 or S 4.
What is the mechanism of pericardial rub in the immediate post MI phase ?
Presence of pericardial rub post MI indicate a transmural involvement or atleast significant epicardial involvement . Recognition of this is important as presence of pericardial rub increases the risk of rupture and hemorrhagic effusion if anticoagulants are used.
What is the relationship between pericardial effusion and pericardial rub ?
Generally it is said with the onset of effusion pericardial rub disappear.But this is not necessarily true.
Rubs after contusion chest and fracture ribs can be with the chest wall and may have no relationship with effusion.
Is pericardial rub a painful condition ?
Pericardial rub associated with acute inflammatory pathology is severely painful (like a pleuritis).But pericarditis associated with chronic inflammatory conditions are less often generate pain.The exact reason is not known.
What is pleuro pericardial rub ?
This clinical entity is poorly defined , often taught by veteran professors in clinical auscultation classes.It can be heard in the mid segment or diaphragmatic pleuritis with or without pericardial effusion in patients with atypical pneumonias.
Posted in Cardiology - Clinical, Tutorial in clinical cardiology | Tagged auscultation, bmj, clinical cardiology, drsvenkatesan, epicardium, lancet, parietal pericardium, pericardial effusion, pericardial rub, pericarditis, spodick, to and fro murmur, venkatesan sangareddi, visceral pericardium | 6 Comments »
September 24, 2008 by dr s venkatesan
No reflow is the terminology used primarily in cath labs where, even after a successful opening and stenting of a coronary artery the coronary blood flow is not restored to myocardium . The point to be emphazised here is blood do cross successfully the site of the obstruction but fails to enter the muscle segment to which the coronary artery is supplying. So the paradoxical situation of artery being open but the myocardium is closed to receive blood flow happens . This is termed as no -reflow. Actually it is a misnomer , and ideally it should be called “no flow” because normal distal flow does not occur (After PCI) in the first instance to get interrupted later on and be labeled as no re-flow. .The only positive effect of PCI in these situation is blood flow would have improved by few centimeters ie till it reaches but falls short of myocardium . In fact no reflow , can be termed as glorified and concealed terminology for PCI failure . It needs urgent action . No reflow is also called as myocardial epicardial dissociation.
Mechanism of no reflow.

Curious case of open coronary artery and closed myocardium !


Coronary microvascular plugging is mainly due to thrombus and atheromatous debri , myocardial edema , microvascular spasm may also contribute.
Where can it occur ?
- First described in cath lab, especially following primary angioplasty.
- It can very well happen following thrombolysis in STEMI.
-
Can occur in venous grafts.
How do you recognise no reflow?
In cath lab it will be self evident from the check angiogram. Some times it is less obvious and may require, myocardial blush score, TIMI frame count, contrast echocardiography, PET scan etc. In post MI a very simple method to recognise this entity could be the observation of persistent ST elevation in ECG .
Treatment.
Extremely difficult. Almost every coronary vasodilator has been tried.(Nitrates, nicorandil, calcium blockers, etc).Success is less than 30%. High pressure flushing with saline inside the coronary artery is advocated by some.Others believe it’s dangerous to do it. So prevention is the key. Avoid doing PCI in complex, thrombotic lesions. Use thrombus suction device like export catheter(Medtronic). Distal protective devices are double edged devices , useful only in experienced hands.
Unanswered question
What is the size of the particle (thrombotic and atheromatous debri) the coronary microcirculation safely handle and push it into the coronary venous circulation and the coronary sinus for disposal ?
If we can lyse the thrombus into micro particles by some mechanism and make it traverse the coronary circulation this complication of microvascular plugging can be treated and prevented .
What is the final message ?
- No reflow is relatively common condition during emergency PCI done for ACS patients
- More common in complex thrombotic lesions.
- Can also occur in STEMI
- Treatment is often vexing . In fact the treatment of this condition is so difficult , it can be termed almost synonymously with “Failed PCI” if flow is not restored.
- Successful treatment of no- reflow means not momentry restoration of myocardial flow by mechanical and pharmacological modalities ,but to maintain sustained myocardial perfusion. This we realise, as patients who have had a no reflow during a PCI, do not perform as well in the follow up .
- So prevention is the key.
Posted in Cardiology -Interventional -PCI, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, cath lab, ccu, complications in cath lab, distal protection device, drsvenkatesan. cardiology, epicardial myocardial dissciation, europcr, export catheter, failed primary pci, failed thrombolysis, jacc, lancet, medtronic export, micro vascular plugging, myocardial edema, nicorandil, no reflow, nstemi, pci, primary angioplasty, primary pci, scai, slow flow, stemi, tct md, thrombus aspiration, timi 3 flow | Leave a Comment »
September 22, 2008 by dr s venkatesan
Differential response of thrombolysis between left and right coronary system
- Thrombolysis is the specific treatment for acute myocardial infarction. ( Privileged few , get primary PCI))
- Failed thrombolysis occurs in significant number of patients ( 30-40%).
- Persistent ST elevation 120 minutes after thrombolysis is best indicator of failed thrombolysis.
- It has been a consistent observation failed thromolysis is more frequent in anterior or LAD myocardial infarction.
In a simple study we have documented patients with inferior MI rarely had persistent ST elevation and thrombolysis was successful in vast majority of patients ( Except in few patients associated lateral MI)

The mechanism of better thrombolysis in right coronary artery is simple.The success of thrombolysis , apart from early time window , is directly correlated with pressure head and the duration of contact between the thrombolytic agent and the thrombus. In right coronary circulation the blood flow is continuous , occurs both in systole and diastole that facilitates the maximum delivery of the thrombolytic agent . Further there is a favorable pressure gradient across RV myocardium as the transmural occluding pressure across RV is considerably less then LV myocardium.

This paper was presented in the “Annual cardiological society of India scientific sessions”
at Chennai, Tamil Nadu.India December 2000
Click to down load PPT full presentation
Posted in Cardiology -Interventional -PCI, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, acute myocardial infarction, angiogram, bmj, cardiology, ccu, circulation, coronary, coronary circulation, failed thrombolysis, lancet, left anterior descending, nejm, nstemi, persistent st elevation, stemi, streptokinase, successful thrombolysis, thrombolysis, tissue plasminogen activator, tpa | 7 Comments »
September 21, 2008 by dr s venkatesan
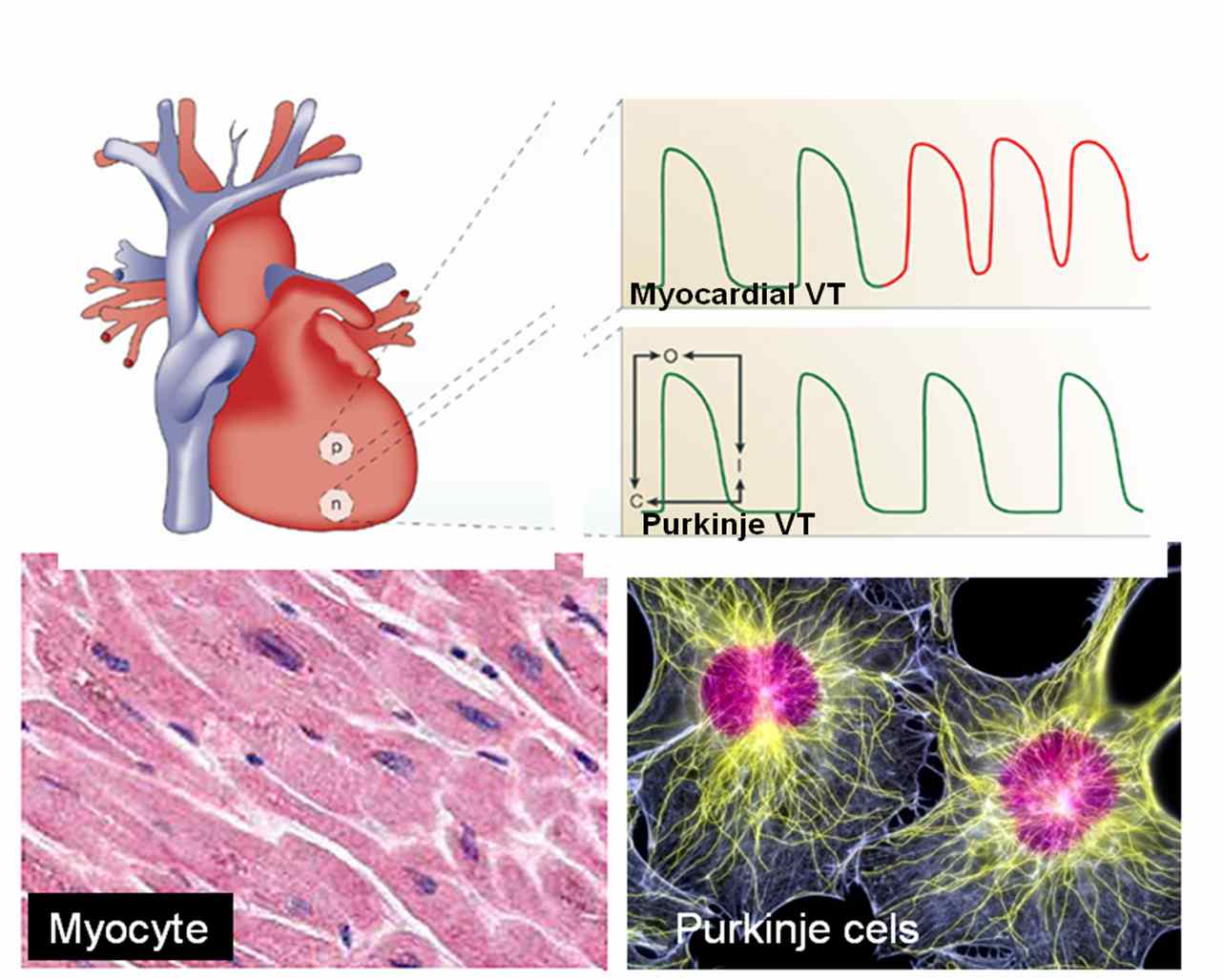
The cell of origin of ventricular tachycardia is rarely discussed at bedside. It is still in research labs !
Ventricles are not made up off entirely myocytes. Apart from myocytes it contains specialised purkinje cells , fibrocytes, interstitial cells and some times primitive mesenchymal cells. Ventricular tachycardia can arise either in purkinje cells, the myocytes or even the fibrocytes. The myocyte VT classically occur during ACS or post infarct VTs.They are more often hemodynamically unstable and quickly degenerate into ventricular fibrillation. Myocardial VT is likely to be pulseless and require DC cardiversion frequently. Purkinje VTs are relatively less unstable. If VT arise proximally in the septum near the distal his, or in bundle branches (BBR) the VT is more stable.They are likely to respond to be medical management.

What is the therapeutic implication of knowing myocardial VT ?
In fact ,simply knowing the cell of origin of VT is not suffice .The ionic currents inside the cell that trigger and sustain the VT is more important. There are few ionic circuits responsible for VT. Sodium , Intra cellular calcium, potassium , beta receptor mediated calcium current.If we know the individual ionic culpirit we can block that specifically . Now we have multi purpose ion blockers like amiodarone which acts like a broad spectrum antibiotic and terminates a VT.
So as of now there is no real purpose of breaking our head in locating the cell of origin and the ions responsible for VT at the bed side ,( Researchers will do that for us !). We have only few antiarrhythmic drugs available in our crash cart .Our job is to choose the optimal drug which will fit in for our patient. In electro physiology labs, radio frequency ablation is done .This is nothing but shooting down the abnormal electrical focus (Cluster of cells or a samll segment of myocardium). In future, a single abnormal cell could be selectively neutralised with cell based therapy assisted by nanopore robots !
Posted in cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, amiodarone, bundle branch reentry, jacc. drsvenkatesan, journal of electrophysiology, myocardial ventricualr tacycardia, nejm. lancet, stemi, ventricualr tachycardia, wellens, zipes | Leave a Comment »
September 20, 2008 by dr s venkatesan
Cardioversion with DC shock offers immediate cure in many of the dangerous ventricular and atrial tachycardias. It is often taught , any hemodynamically unstable tachycardia refractory to medical therapy respond to electrical cardioversion. One should also remember electricity is in fact be called as a drug ! and it should be delivered in proper form and dose. Here it is the paddle size, paddle position and the axis of current flow all are important. Now we have bi phasic currents for better efficacy.

While it is true, most of cardiac arrhythmias respond to shock, there are few which do not respond or respond very transiently.There are few arrhythmias in which ,DC shock is not only ineffective but may precipitate a ventricular fibrillation.
Generally arrhythmias of reentrant etiology respond well to DC shock were interuption of electrical circuit by external current is easily possible. In arrhythmia’s of enhanced automaticity , and ectopic tachycardia it is difficult to extinguish the tachycardia focus with DC shock .
Arrhythmias where DC shock is not going to work are
A. Mutifocal atrial tachycardia(MAT)
B. Digoxin induced arrhythmias.Patients who are on digoxin, has enhanced ventricular automaticity.These patients if they get a DC shock will unmask the ectopic foci.
C. In elderly with atrial fibrillation and sinus node dysfunction it may be dangerous to shock them with out temporary pacing support as sinus node goes for prolonged sleep mode.
D.In electrical storm with VT , if more than three shocks are required within a minute, the VT will most often going to be permanent and the electrical therapy can be termed as a failure. These patients will require intensive pharmacological management( Including magnesium, bretyllium etc)
E. And finally , sinus tachycardia (whatever the rate) is an absolute contraindication for DC shock.
Verapmil is often effective in MAT but correction of hypoxia and acidosis may be critical.For digoxin induced arrhythmias phenytoin may be tried.
What to do when the DC shock fails?
- It will be a tricky situation and one wonder what to do next when the so called universal antidote for cardiac arrhythmia fails !
- Cellular internal millieu is altered by hypoxia and acidosis .It may prevent the effectiveness of cardioversion.So try to correct them .
- Over dirve atrial pacing is one option for automatic tachycardia.
- And now ablation of arrhythmic focus is possible with radio frequency waves in some of these patients.( Diffiuclt as an emergency procedure)
Posted in Cardiology - Clinical, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged atrial fibrillation, binphasic shocks, bmj, cardiology, cardioversion, ccu, coronary, dc shock, digoxin, heart rhythm, jama, lancet, nejm, pace, svt, ventricular arrhythmias, ventricular tachycardia | 4 Comments »
September 19, 2008 by dr s venkatesan
Indication for thrombolysis in ST elevation MI is mainly determined by clinical and ECG features. ST elevation of more than 1mm in two consecutive leads with a clinical suspicion of acute coronary event demands immediate thrombolysis.
Early repolarisation syndrome(ERS) is a is typical mimicker of STEMI . In ERS , ST segment elevation occurs in many leads especially precardial .This entity is estimated to occur in nearly 3-5% of population where a genetic variation in the potassium channel activation is reported.

If they land in ER with some sort of chest pain , chances are high for labelling them as ACS . It is not uncommon for CCU physicians to witness an ERS being lysed . Even in many of the land mark trials (ISIS ) there has been many inappropriate thrombolysis , recognised later on.
What can really happen if you thromolyse them inadvertently ?
Generally nothing happens . But they are exposed to the risk of thromolysis. The ECG changes persist. And troponin will be negative and echocardiogram will not reveal any wall motion defect.
Are we legally liable if a patient with ERS was thrombolysed and he ends up with a bleeding complication like stroke ?
While the physician may feel guilty , there is no reasons for him to feel so.The guidelines are kept little lineant for the indication for thromolysis. When we are promoting a strategy of early thrombolyis on a population based approach in STEMI , there is bound to have a overlap with normality .The benefits out of early thrombolysis for eligible patients for outweigh the few inappropriate thromolysis.
When you want to catch a real criminal it is unavoidable, one gets hold of all suspected criminals before letting them free . Unfortunately in this exercise , some of the innocent might experience intimidation or even a injury at the hands of law enforcers.
Similarly if a patient with ERS develop a severe esophageal spasm and typical angina like chest pain he is absolutely certain to receive thrombolysis. (Troponin, CPK come later , and the results never veto the clinical and ECG criteria ,except probably in LBBB) .Many times critical time dependent decisions are prone for errors in CCU. So it may be unscientific to ask why an ERS was thrombolysed !
How can one prevent inadvertent thrombolysis in ERS ?
Always ask for the previously recorded ECGs .If it is available and look exactly similar to the current ECG chances are unlikely for ACS. In ERS ST segment is generally concavity upwards . ACC/AHA guideline for STEMI ,is aware of this fact , but still advices thrombolysis for all ST elevation irrespective of the morphology of ST segment elevation. This is propably intentional, not to incorporate morphology cirteria of ST elevation for thromolysis .It would potentially make many true STEMIs diagnosed falsely as ERS and deny thrombolysis.
What is the latest news about ERS ?
Now data are coming up, ERS is not entirely benign condition.Some of them ( Even a fraction of ERS population could be a significant number) can have a overlap between Brugada syndrome and they could be prone for dangerous ventricular arrhythmia when challanged with ischemic or other stress.
Posted in cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acc stemi guidelines, acc.aha, american college of cardioogy, bmj, brugada syndrome, cardiology, ccu, chest pain, coronary care, drsvenkatesan, early repolarisation syndrome, emergency room, ers, jama, legal medicine, medical error, nejm, stemi, streptokinase, thrombolysis | 2 Comments »
September 18, 2008 by dr s venkatesan
The pressure tracing between two chambers of the heart are distinctly different .
Apart from the magnitude of the pressure ,(LV at systemic pressure ) The morphology also changes.
- RV pressure curve is triangular in shape,
- Upstroke is not rapid , (Low dp/dt)
- There is no sustained peak ,
- There is an early fall and
- The pressure falls to zero which never happens in LV.
Contary to this LV pressure curve is bullet shaped, with a rapid upstroke, sustained peak, fall later, and does not touch zero.

RV/LV pressure curves in normal persons .Adapted from , Curtiss 1975 Circulation
Note : The shapes of RV curve will change in pathological states.Example in TOF, large VSD there will be left ventricularisation of RV pressure wave forms. Also in pulmonary hypertension RV pressure may mimic a LV curve.
Posted in Hemodynamics, Tutorial in clinical cardiology | Tagged aortic pressure, cardiology, cath lab, drsvenkatesan, hang out interval, Hemodynamics, left ventricle, pressure curve, pressure tracing, pulmonary artery, right ventricle | 2 Comments »
September 18, 2008 by dr s venkatesan
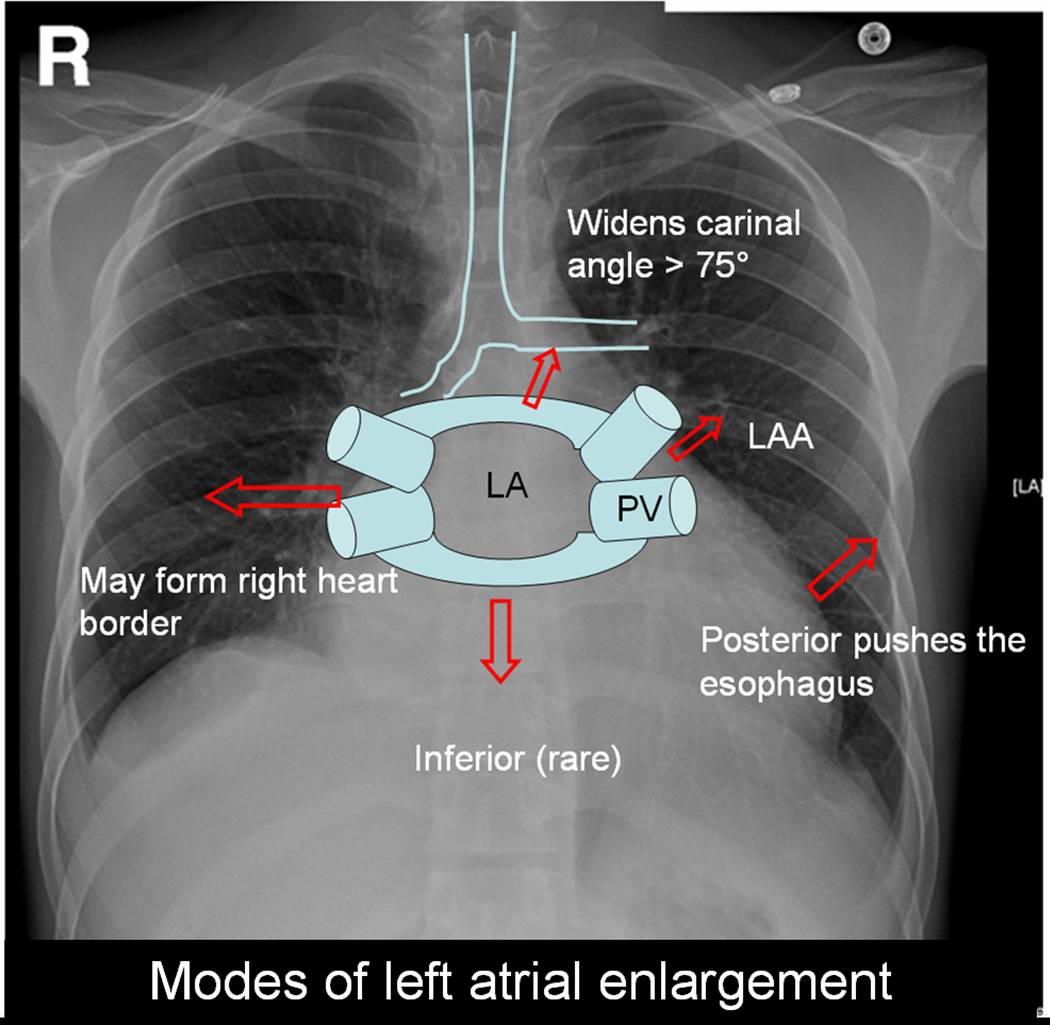
Left atrium is the posterior most chamber of the heart. It is almost a mid line structure. The normal size of left atrium is about 4 / 4 cm. Normal left atrial volume is 46ml in men and 38 ml in women .(Atrial volume in a normal adult population by two-dimensional echocardiography Y Wang, Chest, Vol 86, 595-601.) Left atrium is not an easy chamber to identify in the X ray chest as it does not form the cardiac border.( Except a small circumference of left atrial appendage.(LAA)
Left atrium can enlarge in multiple directions.Generally it dilates in the path of least resistance.

- It is believed left atrial appendage enlargement occur early . LAA enlargemnet seen as a fullness beneath the pulmonary artery shadow. It may be the earliest finding of LAE in X ray. ( This may appear as straight left heart border , as in classical mitral stenosis where MPA is also enlarged). The LAA enlargement is not necessarily in in proportion with LAE.
- LA could also enlarge posteriorly by pushing the esophagus towards the spine.This is visible only in barium swallow.
- Then LA can enlarge either to left or right ( Usually towards right) and reach the right heart border or over shoot it and form the right heart border by itself.This occurs very late in the course.
- The other direction LA goes on to enlarge is superiorly. When LA enlarges superiorly it hits on the left main bronchus and lifts it.This is measured by the widened subcarinal angle which is normally less than 75 degrees.
- LA can enlarge anteriorly sometimes , but it is resisted by right ventricle but rarely right ventricle yields to the LA push and produce a left parasternal lift which could be mistaken for RV enlargement.
- Inferior enlargement can not happen in a significant way as it is limited by the AV groove and strong fibrous skeleton.
With the advent of echocardiography X ray assessment of LA is redundant .(Academic value and in fellows training programs).The upper limit of normal LA size is around 4.5cm.
LA enlargement is commonly seen in
- Rheumatic mitral stenosis, regurgitation. Gross enlargement up to 10 cms are common.
- Hypertensive heart disese.
- Cardiomyopathy, especially restrictive where both atria enlarge.
In all these conditions if atrial fibrillation occurs LA size increases further.
Posted in Cardiology - Clinical, X ray | Tagged annals of radiology, atrium, barium swallow, cardiology, carinal angle, chambers of heart, drsvenkatesan, lancet, left atrial volume, left atrium, left heart border, mitral stenosis, nejm, radiograpgy, radiology, rheumatic heart disease, right heart border, X ray | 1 Comment »
September 14, 2008 by dr s venkatesan

Chest pain is one of the commonest presenting symptom in any hospital both as an emergency or non emergency. Reaching an accurate diagnosis is very important. The main purpose of evaluation of chest pain is to recognise it as cardiac or non cardiac origin . Cardiac chest pain almost always means ischemic chest pain . That is called angina. (Of course there are few important causes for non ischemic cardiac chest pain which Will be discussed later).
Standard features of typical angina.

Chest pain which falls short of typical features are called atypical chest pain . Some recommend at least three typical features to label it as angina.
After the clinical examination patients should be categorised in one of the following .
- Typical angina
-
Atypical chest pain
-
Non cardiac chest pain** Non cardiac chest pain is not a diagnosis. Any physician (or a specialist) should take some effort to localise it. (Muscle, nerve , pleura , anxiety etc) . But generally once these patients are ruled out of cardiac pain they become less special and are simply referred back to their family physician, only to return back with another cardiac pseudo-emergency in a different hospital .
Why we are diagnosing atypical chest pain liberally ?
Currently more number of patients as well as the physicians are aware of the looming epidemic of CAD. The other major reason is the lack of application of mind during foirst clinical appraisal and examination. Many of the patients with non cardiac chest pain (Muscle, nerve , pleura ) are termed as atypical chest pain. Though some of the popular texts use atypical chest pain and non cardiac chest pain interchangeably , it is not correct to do so. For example don’t ever label a patient with chest pain with chest wall tenderness as atypical chest pain and order a cardiac work up .It is a poor model to emulate , that consumes time and resources!.Instead they should be diagnosed a confident non cardiac chest pain and dealt properly.

Once a patient is diagnosed atypical chest pain what’s next ?
They should get a complete physical examination,ECG, and undergo exercise stress test. In the screening of CAD , angina can be termed a hard sign, atypical chest pain is a soft sign, resting ECG is surprisingly a soft sign again (unless you record it during chest pain). Exercise stress testing is the ideal investigation in evaluation of chestpain.( 70-80% accuracy). This can be improved upon by Thallium, SPECT, stress echo etc. As of now coronary angiogram is considered the ultimate gold standard (Not pure gold !) to rule out CAD.
It is also worthwhile to remember non anginal chest pain can also be an emergency and life threatening
- Pulmonary embolism
- Pneumothorax
- Thoracic tumors
- Aortic aneurysm (Dissection and non dissection) The list is not exclusive
Final message
What do we really mean by atypical chest pain ?
In reality we don’t mean any thing !
When a cardiac physician is confused or rather , unable to rule out angina , at the same time he is not confident of calling it as non cardiac chest pain, he has the luxury of using this terminology . It is obvious this terminology should minimally be used. Once diagnosed these patients can’t carry on with this tag for long. They should be reinvestigated , (Right from history and clinical ex) .They should either enter the cardiac work up protocol or a non cardiac source for pain should be fixed immediately.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, angina, annals of internal medicine, approach to chest pain, atypical angina, atypical chest pain, bmj, cardiology, chest pain, chest wall tenderness, coronary, drsvenkatesan, ECG, emergency room, er, Heberdens, jama, lancet, myalgia, nejm, non cardaic chest pain, troponin, unstable angina | 4 Comments »
« Newer Posts - Older Posts »

















{kind=link}
{kind=link}
{kind=link}
{kind=link}