September 11, 2008 by dr s venkatesan
Infective endocarditis is a serious clinical cardiac problem. The disease has evolved over many decades and now we are witnessing the most virulent forms of the disease . Infection of heart , can occur in a native healthy valve, native diseased valve, or a prosthetic valve. Further, IE can occur either as an acute (usually non diseased valve) , or sub acute form (usually in diseased valve).The changing microbial pattern has made this entity very complex. The vigorous treatment protocols are available for IE. Still the prognosis and outcome with medical management is dismal even in best centers.So the role of surgery in IE has increased over the years.We propose here, a radically different approach to the problem.
Traditionally there is a set of criteria for surgery in IE : These include
- Abscess formation
- Worsening valve lesion
- Refractory cardiac failure
- Persistent fever even after 2 weeks of appropriate and adequate anti microbial therapy .
- Vegetation of more than 10mm size.
- Failed medical treatment
(The list is not exclusive)
In any large tertiary hospital series, if you apply the above rule more than 50 % of all patients with IE will be the candidates for immediate surgery.
In the remaining 50% the mortality in medical management is very high. The reason being, the medical treatment is often prolonged over weeks. Many of the complications occur during the course of medical treatment.The common ones are abscess formation, embolic episodes, renal failure etc.Once a complication set in we call it as failed medical treatment and ask our surgical colleagues to operate.By this time patient’s general condition deteriorates and either the surgeon refuses to take up the case or patient dies on the table.
So the key point is , failure of medical treatment is so common , it is simply not acceptable to delay the surgery in these patients as majority of them are doomed to fail the trial of medical therapy.

What is the incidence of failed medical management, how to recognise it ? what is the impact of recognising it late ?
- Failed medical therapy is around 60-70% even in best centers.
- Failed medical patients constitute the greatest surgical risk .
- So it is proposed all IE patients should be triaged early and the dominant theme should be surgery (Commonly valve replacement, or valve repair) .
- If there is large vegetation surgery may be done for the sole purpose of physical removal of the vegetation*.
Final message
In Infective endocarditis experience has taught us, surgery should be the default management protocol and medical therapy should be offered to selected few who don’t require surgery.This is especially true in preexisting rheumatic valve disease.
*The fundamental principle of management of infectious diseases, state that when there is a resistant focus of infection .Always remove the focus whenever possible.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged antibiotics, aortic valve, cardiology, cdc, chordal rupture, culture, drsvenkatesan, duke's, durant, fuo, heart, infectious disease, infective endocarditis, micro biology, mitral valve, myocardial abscess, prolonged fever, prosthetic valve, puo, staphylococcus, valve replacement, valvular heart disese, vancomycin, vegetations, viridans, von ryan | 1 Comment »
September 10, 2008 by dr s venkatesan
This is a 15-year-old post about LVH, written in 2008. Few of my colleagues, now agree with this, still hesitate to oblige in the open, suggesting it is too good to be true! Re-posting it for your own assessment. Surprised, why cardiology community didn’t consider this observation worthy to pursue.
Advantages of Left ventricular hypertrophy (LVH)
Left ventricular hypertrophy is one of the most common clinical cardiac entity.It is recognised either by ECG or echocardiography.LVH has a unique place in cardiology as it can imply a grossly pathological state or a marker of healthy heart as in physiological hypertrophy in athletes.
Logic would suggest, in this era of stem cells and nano medicine , every muscle fibre in ventricle is worth in gold !. So when the nature provides an extra reserve of myocardium in the form of LVH one should welcome it , if otherwise not harmful.

Is LVH due to systemic hypertension benign ?
Not really, LVH has been shown to be an independent cardiac risk factor. (The famous Framingham study)Further LVH can result in diastolic dysfunction and the risk of cardiac failure increases.
But in spite of these observations, an astute clinician with considerable experience will appreciate , patients with LVH fare better during an acute coronary syndrome !
This has been a consistent clinical observation . (Shall we call it as class C . ACC /AHA evidence ? )
Is LVH an asset during ACS ?
- A hypertrophied heart takes ischemic injury very easy , it doesn’t really hurt much . Another possibility is that in LVH myocytes are relatively resistant to hypoxia .
- Patients with LVH rarely show significant wall motion defect following an STEMI.This is probably because the full thickness transmural necrosis is almost never possible even if extensive MI occurs.
- This is also reflected in ECG as these patients rarely develop q waves in following STEMI .
- Persistent ST elevation and failed thrombolysis is very uncommon in pateints with LVH.
- LVH provides a relative immunity against development of cardiogenic shock . It requires 40% of LV mass destruction to produce cardiogenic shock.This can rarely happen in LVH. In a long term analysis we have found none of the patient with LVH developed cardiogenic shock following STEMI.
- LVH patients are also protected against development of free wall rupture.
Concluding message
“Lack of published evidence is the weakest evidence to dismiss a true myth”
LVH , either pathological or physiological, has a hitherto unreported beneficial effect.It acts as a myocardial reserve and helps limit the impact of STEMI.
Posted in Cardiology - Clinical, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, atheletes heart, cardiac failure, cardiac reserve, cardiology, coronary, framingham study, hypertension, left ventricular hypertrophy, LV mass, lvh, myocardium, nstemi, pci, ptca, stemi | 1 Comment »
September 10, 2008 by dr s venkatesan
Intra coronary thrombosis is the sine qua non of acute coronary syndrome ( Both STEMI and NSTEMI.) But thrombolysis is the specific therapy in STEMI and is contraindicated in NSTEMI/UA.

Why is this apparent paradox ? What is basic differnce between UA and AMI ?
 In STEMI there is a sudden & total occlusion of a coronary artery usually by a thrombus with or without a plaque .The immediate aim is to open up the blood vessel . Every minute is important as myocardium undergoes a continuous process ischemic necrosis. So thrombolysis (or more specifically fibrinolysis should be attempted immediately) .The other option is primary angioplasty, which will not be discussed here.
In STEMI there is a sudden & total occlusion of a coronary artery usually by a thrombus with or without a plaque .The immediate aim is to open up the blood vessel . Every minute is important as myocardium undergoes a continuous process ischemic necrosis. So thrombolysis (or more specifically fibrinolysis should be attempted immediately) .The other option is primary angioplasty, which will not be discussed here.
The thrombus in STEMI is RBC & fibrin rich and often called a red clot. Number of fibrinolytic agents like streptokinase, Tissue palsminogen activator,(TPA) Reteplace, Tenekteplace etc have been tested and form the cornerstone of STEMI management.The untoward effect of stroke during thrombolysis is well recognised , but usully the risk benefit ratio favors thrombolyis in most situations except in very elderly and previous history of stroke or bleeding disorder.
Unstable angina is a close companion of STEMI . Many times it precedes STEMI often called preinfarction angina. During this phase blood flow in the coronary artery becomes sluggish gradually,and patients develop angina at rest .But unlike STEMI there is never a total occlusion and myocardium is viable but ischemic, and emergency salvaging of myocardium is not a therapeutic aim but prevention of MI becomes an aim. It is a paradox of sorts , even though thrombus is present in UA , It has been learnt by experience thrombolytic agents are not useful in preventing an MI .
Why thrombolysis is not useful in UA ?
1.In unstable angina mechanical obstruction in the form of plaque fissure/rupture is more common than completely occluding thrombus. So lysis becomes less important.
2. Even if the thrombus is present , it is often intra plaque or intra lesional and the luminal projection of thrombus is reduced and hence thromolytic agents have limited area to act.
3.Further in UA/NSTEMI since it is a slow and gradual occlusion (Unlike sudden & total occlusion in STEMI) the platelets get marginalised and trapped within the plaque .Hence in UA thrombus is predominantly white . Often, a central platelet core is seen over which fibrin clot may also be formed.
4.All available thrombolytic agents act basically as a fibrinolytic agents, and so it finds difficult to lyse the platelet rich clot.There is also a small risk of these agents lysing the fibrin cap and exposing underlying platelet core and trigger a fresh thrombus.This has been documented in many trials( TIMI 3b to be specific) So if we thrombolyse in UA , there could be a risk of recurrent ACS episodes in the post thrombolytic phase.
5. UA is a semi emergency where there is no race against time to salvage myocardium .Administering a stroke prone thrombolytic agent tilts the risk benefit ratio against it.
6. Among UA, there is a significant group of secondary /perioperative UA due to increased demand situations. Here there is absolutely no role for any thromolytic agents, the simple reason is , there is no thrombus to get lysed.
7.Many of the UA patient have multivessel CAD and might require surgical revascualarisation directly .
So fibrinolytic agents are contraindicated in UA so what is the next step ?
The emergence of intensive and aggressive platelet-lytic agents.
A combination of aspirin, clopidogrel, heparin, glycoprotien 2b 3a antagonist formed the major therapeutic protocol in these patients.Even though these are called antiplalet agents some of them like 2b/3a antagonist eptifibatide, tirofiban, and many times even heparin has a potential to dissolve a thrombus. So technically one can call these agents as thrombolytic agents.
What are the unresolved issues
Even though clinical trials have convincingly shown thrombolytic agents have no use in UA .There is a nagging belief THAT there could be group of patients with UA , still might benefit from thrombolysis as total occlusions have been documented in some cases with UA.This is especially true in peri-infarction unstable angina (Pre & post) as there is a fluctuation between total and subtotal occlusions ) .But bed side recognition of this population is very difficult.
Many would consider this issue as redundant now, since most of these patients are taken up for emergency revascularisations
Posted in Cardiology - Clinical, cardiology- coronary care, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, angioplasty, aspirin, bmj, cardiology, clopidogrel, clot, coronary thrombosis, drsvenkatesan, eptifibatide, fibrinolytics, fuster, heparin, jacc, lancet, madras medical college, nejm, nstemi, pci, platelet, ptca, red clot, reteplace, stemi, streptokinase, thrombolytic agents, tisue plasminogen activator, tnk tpa, tpa, unstable angina, virchow, white clot | 9 Comments »
September 8, 2008 by dr s venkatesan
Diuretics are the most commonly prescribed anti hypertensive agents.Thiazide diuretics which was introduced many decades ago , lost popularity in recent years , again got a second life after the publication of ALLHAT trial recently. Now diuretics has become the the drug of first choice in almost any hypertension unless any specific contraindication.
The most commonly used thaizide is hydrochlorthiazide ,and chlorthalidone.The blood pressure reducing effect is so consistent and smooth , all the currently popular molecules like ACE inhibitors and ARBs come with a combination with thiazide. While every one is clear diuretics are effective anti hypertensive agent How it does is not clear.

How does a diuretic reduce blood pressure?
A. The exact mechanism is not clear. May not be uniformly effective in all patients with HT.
B . Salt sensitive HT respond well to diuretics.
C. Volume correction /free water clearance might be a factor
D. Direct effect on vascular smoth muscle documented.The sodium transporter is blocked and hence calcium : sodium exchange is prevented .This depletes intracellular calcium in vascular smooth muscle cells .Less calcium for actin myosin interaction and hence vasodilatation
E. Thiazides combine well with all other antihypertensive drugs (ACEI, ARB, Beata blockers, calcium blockers)
F. Loop diuretics like frusemide can never be a good antihypertensive agent.
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged acei, allhat, ARBS, diuretics, drsvenkatesan, hypertension, jnc7, lancet, loop of henle, reanl hypertension, salt sensitive, sodium, thiazide | Leave a Comment »
September 7, 2008 by dr s venkatesan
CURRENT CARDIOLOGY PRACTICE: EVIDENCE OR EXPERIENCE BASED ? AN ANALYSIS OF ACC/AHA GUIDELINES.
S. Venkatesan, Madras Medical College. Chennai
If a major therapeutic procedure is adviced based on simply by experience or expert opinion how can we say evidence based medicine is practiced !
Evidence based cardiology is the buzz word in global cardiovascular health care organizations. All diagnostic and therapeutic interventions are undergoing rigorous randomized trials for proof of efficacy and safety.  ACC/AHA have published management guidelines and it has been accepted as de-facto standard of clinical cardiology practice world wide. In these guidelines class 1 indication is defined as Conditions for which there is evidence for and/or general agreement that the procedure is useful and effective. These indications are supported by three levels of evidence.(A,B,C) .It has been observed, many of the recommendations in class 1 were supported by only level C evidence. (Expert consensus or agreement ). We analysed how much of todays guidelines is agreement based and how much is evidence based. The latest practice guidelines of ACC/AHA for Acute myocardial infarction , Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction , chronic stable angina ,coronary angiography were analysed. The no of class 1 indications were counted in each set of guidelines and each of the indication were sub grouped with reference to the levels of evidence to which it was supported. There were a total of 210 class 1 indications.
ACC/AHA have published management guidelines and it has been accepted as de-facto standard of clinical cardiology practice world wide. In these guidelines class 1 indication is defined as Conditions for which there is evidence for and/or general agreement that the procedure is useful and effective. These indications are supported by three levels of evidence.(A,B,C) .It has been observed, many of the recommendations in class 1 were supported by only level C evidence. (Expert consensus or agreement ). We analysed how much of todays guidelines is agreement based and how much is evidence based. The latest practice guidelines of ACC/AHA for Acute myocardial infarction , Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction , chronic stable angina ,coronary angiography were analysed. The no of class 1 indications were counted in each set of guidelines and each of the indication were sub grouped with reference to the levels of evidence to which it was supported. There were a total of 210 class 1 indications.
|
|
Class 1
Level A
|
Class 1
Level B
|
Class 1
Level C
|
P value
1A vs 1C
|
|
AMI(54)
|
7
|
25
|
22
|
<.0001
|
|
UA (66)
|
11
|
26
|
29
|
<.0001
|
|
CSA(59)
|
8
|
29
|
22
|
<.0001
|
|
CAG(31)
|
3
|
12
|
16
|
<.0001
|
|
Total(210)
|
29(13.9%)
|
92(43.8%)
|
89(42.4%)
|
<.001
|
13.9% of class 1 indications were based on level A evidence. 42.4% of class 1 indication were based on Level C ( agreement of experts).Though evidence based cardiology is considered to define the standards in Cardiology practice in reality we lack evidence in most of the situations.
We conclude that consensus or agreement based cardiology practice is the dominant theme in current ACC/AHA
Posted in Cardiology -Interventional -PCI, cardiology-ethics, Infrequently asked questions in cardiology (iFAQs) | Tagged Add new tag, american college of cardiology, bmj, cardiology, cardiosource, coronary, ebm, evidence based medicine, guidelines, lancet, md consult, nejm, pci, unstable angina, who | Leave a Comment »
September 6, 2008 by dr s venkatesan
There are numerous complex grading for bifurcation lesions available.
The one proposed by Medina is simple and most useful.

In this grading three segments
- Proximal main vessel
- Distal main vessel
- Branch vessel
Are given a code 0, and 1 if lesion is present or absent .
This grading gives simple and fast method to label a bifurcatiuon lesion and to asssess the response to PCI. The only issue here is the individual lesions are not graded , for example branch vessel ostium just involved about 20 % is not addressed . Further TIMI flow in these vessels may also be incorporated
How medina grading can be used to assess effectiveness of
angioplasty ?
A patient with 1.1.1 after the treatment should revert back to 0.0.0. if converted into 0.0.(.5) may indicate a residual side branch lesion .5 shall indicate 50% residual lesion, .3 , 30% etc
What is the best management strategy for bifurcation lesions?
The topic has been discussed extensively for over a decade in various forums.
Though the lesions and intervention techniques appear complex the basic concept is simple.
Following is the 8 point algorithm
1. Assess the bifurcation lesion accurately.
2. Apply the general rule and ask the first question whether PCI is neccessary at all ? if decided for PCI
3. Stent the main vessel.Protect the side branch.
4. Dilate the side branch with a balloon.(KIss or through the struts)
5. Very rarely, if the side vessel is more significant and large stent it and balloon the main vessel.
6. Use drug eluting stents with caution .
7. Resist the temptation of using two stents unless the situation demands and is absolutely required.
8. Never attempt to do bifurcation angioplasty during ACS as apart of primary angioplasty.( Unless you’re extremely competent, even then aim of primary PCI is to salvage myocarium quickly , not to provide TIMI 3 flow in non IRA vessel.)
Dr.S.Venkatesan.Madras medical college.Chennai.
Posted in Cardiology -Interventional -PCI, Infrequently asked questions in cardiology (iFAQs) | Tagged acc, acs, bifurcation angioplasty, cardiology, coronary, cypher, des, drsvenkatesan, drug eluting stent, europcr, jacc, medina, nejm, pci, primary pci, ptca, scai, side branch, stenting, taxus, tctmd, unstable angina, xience v | Leave a Comment »
September 1, 2008 by dr s venkatesan
 Edema is considered the cardinal feature of cardiac failure for decades. It is one of the minor criteria of the Framingham protocol to diagnose cardiac failure.
Edema is considered the cardinal feature of cardiac failure for decades. It is one of the minor criteria of the Framingham protocol to diagnose cardiac failure.
The mechanism of edema in cardiac failure is multifactorial . The major mechanism attributed is raised venous pressure. This is transmitted backwards into the circulation and resultant increase in hydrostatic pressure in the venous end of capillaries results in edema .
Even though this is considered as the dominant mechanism for decades , it may not be true. Apparent reduction in cardiac output (Effective circulatory volume) and resultant reduction in renal blood flow triggers renal ischemic response and RASS activation (Rennin angiotensin aldosterone system). This is a powerful stimulus for sodium and water retention . This could be the major mechanism of cardiac edema. While there is clearcut explanation for the mechanism of edema in cardiac failure the explanation for lack of edema in many is not available in literature.
Does the activation of neuroendocrine happen in every one with cardiac failure ?
We think so ! but it may not be. Further, activation of RASS trigger a counter hormone response mediated by atrial natriuretic peptide that promotes active water loss from the distal tublues which could prevent edema formation in many. So there is a distinct group of patients with cardiac failure who rarely develop edema .
In which type of cardiac failure edema is common and gross?
- Predominatly right sided failure.
- Corpulmonale
- Tricuspid valve disese
- Constrictive pericarditis
Posted in Cardiology - Clinical, Infrequently asked questions in cardiology (iFAQs) | Tagged angiotensin, anp, cardiac failure, cardiology, clinical signs in cardiology, davidson medicine, drsvenkatesan, edema, harrison's medicine, hutchisons clinical, macleod, neuroendocrine, neurohormonal, odema, rass, rennin | 4 Comments »
August 31, 2008 by dr s venkatesan
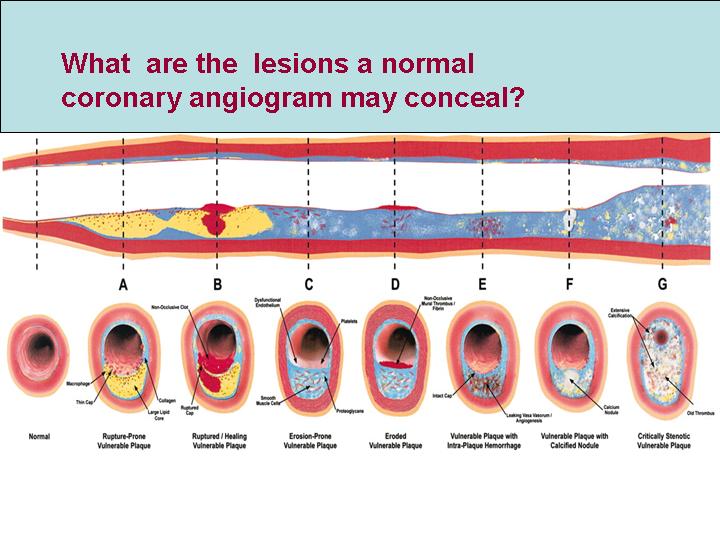
Coronary angiogram is a video graphic snap shot of coronary arterial lumen which is filled with radio opaque dye. This is some times called as coronary luminogram . It is a paradox , when we say normal coronary angiogram we can only mean normal coronary lumen. But generally, this can provide sufficient information regarding the status of coronary blood flow.There are three structured layers in coronary artery wall . Coronary angiogram can not give any information about the status of the intima, media or adventia .
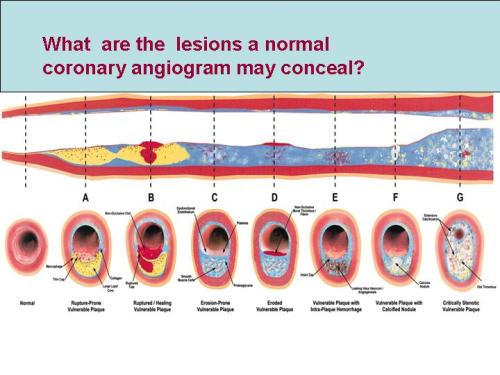
Lesions A to F may be totally missed by conventional coronary angiogram
A patient with normal coronay angiogram can have diffuse atheroscelrosis or localised atherosclerosis within the media of coronary artery .Many times these atherosclerotic plaques grow outward into the adventia and fail to encroach upon the lumen to be detected by coronary angiogram. These plaques , even though has an hemodynamic advantage, in that it doesn’t block blood flow , has a serious risk for sudden rupture and result in an acute coronary syndrome.
So what is the message?
A normal coronary angiogram can never convey a meaning of normal coronary arteries.

A person who has a normal coronary angiogram has no guarantee that he won’t develop a coronary event in the near future.(But the the chances are very low)
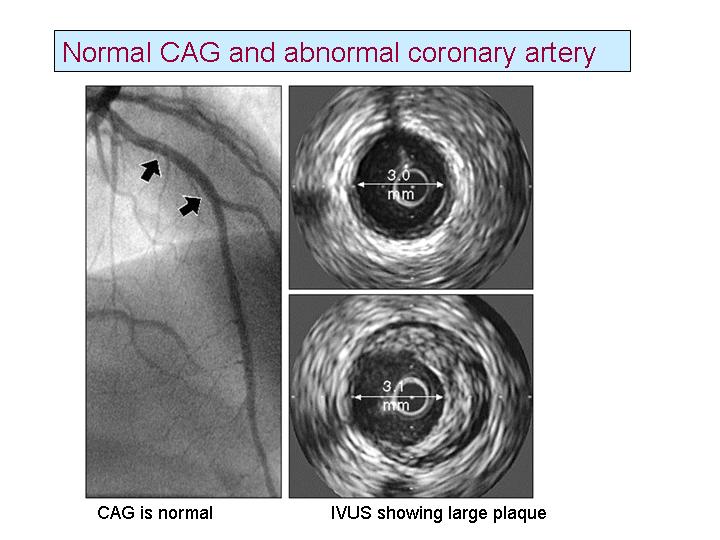
If coronary angiogram has serious limitations what is the next alternative ?
Intra vascular ultra sound imaging(IVUS) can give us an idea of the coronary arterial wall anatomy. This investigation , though available for clinical application is too complex for regular use.So , you can’t subject every patient with normal CAG to an IVUS (Intra vascualar ultra sound) to confirm the normality. The best option is what we follow every day in our practice .Tell your patients with normal coronary angiogram , that they are likely to have normal coronary arteries ! don’t add up to their anxiety by saying, in spite of normal CAG still they can carry gross atherosclerosis in their arteries. Anxiety can precipitate an coronary event. Too much technical information to the patients can be counter productive. Instead advice regular life style modification, blood pressure ,diabetes, lipid control etc .
Posted in Cardiology - Clinical, Cardiology -Interventional -PCI | Tagged cad, cardiology, cleveland, coronary angiogram, coronary artery, intra vascualr ultrasound, ivus, mayo clinic, pci, ptca | 1 Comment »
August 24, 2008 by dr s venkatesan
All is not well, that ends well !
Treatment guidelines in cardiology practice are periodically published by ACC/AHA/ESC.These guidelines represent the current scientific practice. They are called some times as recommendations. Medical professionals tend to adhere to this guidelines whenever possible.They are not legally binding in most of the countries.In USA some states believe it, to be legally binding.
The problem with these guidelines are , they are classified as class 1 ,class 2 , class 3 recommendations.
Class 1, A drug , device or a procedure Is definitely useful and must be prescribed.
Class 3, A drug , device or a procedure Is not useful and should not be used .
Class 2*, A drug , device or a procedure may be useful or may be harmful , and hence may be used or may not be used . (Vaguest possible guideline!)
*Altered to convey the meaning
What are the guideline violations that can be sued in court of law ?
A person with established CAD who is not been prescribed a statin (Cholesterol lowering drug) can be sued straight away, even if the patient has no adverse outcome due to the nonprescription of that drug. The issue here is , the doctor has not prescribed a drug which has proven benefit .The law is clear on that .Most will agree that, the doctor is at fault , and he is never protected even by their colleagues .He can’t defend his action.
What are the medical errors that can never* be sued in court of law !
But the same doctor who opens up a totally occluding coronary artery in an asymptomatic patient(CTO -chronic total occlusion) and lands up in a complication and the patient dies. This could be major guideline violation as opening a CTO in an incidentally detected , asymptomatic patient is a class 3 recommendation. Neither the physician, patient , institution nor the regulatory authorities bother about this even though there is strong case for censure , in reality it never happens. Number of experts from leading hospitals do this procedure in live work shop all over the world with full media glare, It is an irony the same experts are only writing in their guidelines that these procedures should not be done inappropriately.
And this medical error ( Should we call it a crime if it is knowingly done ! ) keeps growing as the physician never feels guilty about it .
The message here is
A physician of a state of the art hospital, in a scientifically advanced country goes scott free and guilt free even if he openly violate the scientific guidelines and do a inappropriate procedure that result in a patient death. Mean while a small time physician in a remote place in the same country can be taken to task for not prescribing a officially recommended drug (By standard guidelines) .He will be labelled unscientific and unethical even if his non prescription , had not caused any untoward health outcome .
In short , in today’s modern medical practice
Even a ” Minor error of ommision” attracts guilt and perceived fear among the physicians. Meanwhile many of the ” Major errors of commission” done by professionals are rarely frowned upon and thus these mistakes continue to perpetuate !
*There should be a strong provision in medical law to address the issue of inappropriate procedures even if the procedure has not resulted any untoward effect to the patient.
Posted in Cardiology -Interventional -PCI, cardiology- coronary care, cardiology-ethics | Tagged cto, drsvenkatesan, ebm, ethics in cardiology, evidence based medicine, medicine, modern medicine, pci, ptca, statins | Leave a Comment »
August 16, 2008 by dr s venkatesan
Interventional cardiology as a speciality is in cross roads.
The number of coronary interventions (PCI) has increased exponentially world over. With increasing Cath labs and growing expertise , access to PCI has enormously increased even in underdeveloped countries. Meanwhile , public lack specific technical information about the appropriateness of these costly procedures. It is our duty to do self audit on this issue. .
In this context, the evaluation following a PCI should look beyond lumen oriented endpoints. Many land mark trials on DES report 3 months are 6 months angiographic outcome and better luminal appearance . Many tend to worry more about the status of the stent rather than the patient ! This is primarily because the device companies have repeatedly stressed the technical end points rather than clinical end points .
It is a well recognised fact that ,stented coronary artery never guarantees against future coronary events (ACS) either within the stent or away from it .It is an explict fact that , a patient after getting a coronary stent , especially a drug eluting stent carries a life long risk of acute stent obstruction and possibly SCD .This information is rarely passed on to the patient in and hence they are not able to take “learned consent”
It is true , one gets a gratifying feeling when opening up a obstructed artery , but we also need to answer this simple question What is it’s impact on patient’s life ?
COURAGE & OAT trials have put a break on the prevailing precondtioned behaviour in the labs, namely any obstruction must be relieved if technically feasible .
One should recall the Gruentzig’s legacy . Whaterver, we do inside a patient’s coronary artery must have some useful purpose . We should not use patient’s coronary artery to show our expertise and skills !
Dr.S.Venkatesan, Madras Medical College, Chennai, India
Posted in Cardiology -Interventional -PCI, Infrequently asked questions in cardiology (iFAQs) | Tagged acs, cardiology, cath lab, chronic stable angina, drsvenkatesan, ethics in cardiology, ethics in medicine, gruentzig, pci, ptca, stemi | Leave a Comment »
« Newer Posts - Older Posts »








{kind=link}