Recurrent myocardial infarction following an ACS is a fairly common clinical problem. Many times this is not recognised because it is difficult to establish the diagnosis.
The issues relevant here is
When does the first infarct (Index infact) process end ? and when the second infarct process start ?
Can the first infarct be a STEMI and the reinfarct be NSTEMI ? ( Dual acute coronary syndrome )
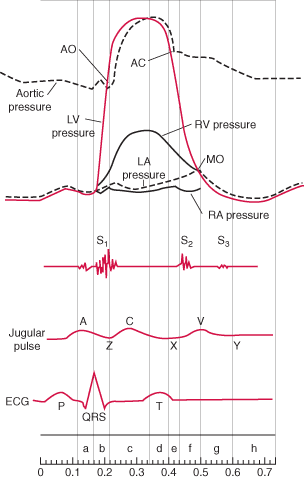
The only way to confirm a diagnosis of reinfarction is to document raising titres of cardiac enzymes and second peaking of CPK MB . New fresh ST elevation after a succesful thrombolysis is also a useful sign. But ST elevation in a q lead simply reflects a wall motion defect . So it requires enzymes to confirm it.
When there is tachycardia the ST segments tend to elevate following MI.
Other confounders are Infarct expansion and infarct extension .
These are macropathological entities almost impossible to dignose with surface ECG. What we diagnose as re-infarction could be an infact a infarct expansion.The modern terminology for infarct expansion is ventricle remodeling .The extreme remodeling results in ventricular aneurysm .Adverse acute ventricular remodeling can closely mimic a reinfarction .
What is clinical relevance of diagnosing reinfarction ?
Nothing great !
In modern day cardiology it is not a bother whether the infarct is expanding, extending or reinfarcting !All one has to do in a patient with chest pain ,showing a fresh ST elevation following STEMI is to take him/her to cath lab .
The only issue here one has to remember there are mechanical cause also for ST elevation following STEMI .
Dr.S.Venkatesan,Madras medical college, Chennai.








{kind=link}